
Abstract
Objective
To investigate the clinical effect of dexmedetomidine combined with dezocine in local anesthesia for endoscopic dacryocystorhinostomy (DCR).
Methods
Ninety patients undergoing elective endoscopic DCR were randomly divided into two groups, local anesthesia group (LA group n = 45) and general anesthesia group (GA group, n = 45). These subjects were all American Society of Anesthesiologists (ASA)-Physical Status I-II patients. The changes of mean arterial pressure (MAP) and heart rate (HR) were observed and recorded before anesthesia (T0), after anesthesia (T1), at the beginning of surgery (T2), and at the end of surgery (T3). The visual analogue scale (VAS) score was observed and recorded immediately after awakening from anesthesia and at 1, 2, 6, and 12 h after surgery. Additionally, the occurrence of adverse reactions after surgery and the sedation-agitation scale (SAS) score after awakening were recorded.
Results
Compared with the LA group, the MAP and HR of the GA group were significantly lower at T1 and T2, but significantly higher at T3. Local anesthesia was associated with lower VAS score immediately after awakening and at 1, 2, 6, and 12 h after surgery. Also, local anesthesia caused a lower incidence of postoperative agitation, nausea, and vomiting. The SAS score in the LA group was markedly higher than that in the GA group.
Conclusion
Local anesthesia with dexmedetomidine and dezocine as adjuvants in endoscopic DCR has more stable hemodynamics and reduces the stress response during perioperative period. Also, this anesthesia achieves better postoperative sedation and analgesia effects, reduces postoperative complications, and improves the quality of awakening from anesthesia. Collectively, local anesthesia is a comfortable and safe option for patients with high risks of general anesthesia and those unwilling to receive general anesthesia.
Introduction
Chronic dacryocystitis is a common ophthalmic disease in clinical practice, and surgery is the main treatment. In recent years, traditionally used for chronic dacryoadenitis include nasal lacrimal sac anastomosis, lacrimal sac removal surgery, and lacrimal duct placement surgery.1,2 With the gradual development of surgical techniques, endoscopic dacryocystorhinostomy (DCR) has gradually replaced the traditional external approach because of its advantages of clear operative field, less tissue trauma, and without external scarring. 3 The type of anesthesia has changed accordingly. At present, most patients undergoing DCR are under general anesthesia.4,5 However, it is found that general anesthesia causes a higher incidence of adverse reactions, such as intraoperative and postoperative bleeding, postoperative agitation, and vomiting. This type of anesthesia is also associated with worse pain intensity experienced by patients during postoperative awakening, which does certain harm to the patients. Additionally, for some patients with high risks of general anesthesia and unwillingness to accept general anesthesia, it is still necessary to find other safe and effective anesthesia options for surgery. In recent years, studies have shown that local anesthesia with sedative and analgesic adjuvants has a good safety record for endoscopic DCR,6,7 but there are still few reports on this field.
Dexmedetomidine is a widely used sedative and analgesic drug in clinical practice, causing no respiratory depression and reducing stress response. Dezocine is also a commonly used analgesic without respiratory depression in clinical practice.8,9 However, there are few studies on the application of dexmedetomidine combined with dezocine as an adjunct to local anesthesia. Given this lack, this study investigates the safety and efficacy of this combination in local anesthesia for endoscopic DCR, aiming at exploring a safe and effective anesthetic technique for endoscopic DCR.
Materials and methods
Baseline data
This study was approved by the hospital ethics committee, and all patients and their families signed informed consent. A total of 90 patients who received nasal endoscopic DCR in our hospital between October 2017 and October 2019 were selected and randomly divided into two groups. The local anesthesia group (LA group, n = 45) was given local anesthesia, while the general anesthesia group (GA group, n = 45) was given general anesthesia.
Inclusion criteria were: (1) Patients with American Society of Anesthesiologists (ASA)-physical status I-II, I: A normal healthy patient, II: A patient with mild systemic disease; (2) Patients aged 18–70 years old; (3) Patients with a body mass index (BMI) of 18–25 kg/m2; and (4) Patients with normal heart, lung, liver, and kidney function before the surgery. Exclusion criteria were as follows: (1) Patients allergic to the anesthetic drugs used in the study; (2) Patients with severe cardiovascular disease; (3) Patients with a long history of analgesic and sedative drug use; (4) Patients in pregnancy and childbirth; and (5) Other contraindications for general anesthesia.
Research methods
All patients were required to fast for 8 hours and forbidden to drink for 2 hours before surgery, and no premedication was given. After the patient was admitted to the operating room, venous access was established and blood pressure, electrocardiogram, and SpO2 were monitored. Additionally, before surgery, the patients in both groups were treated with an intravenous injection of 5 mg tropisetron to prevent vomiting.
The LA group was given adjuvants as local anesthesia (nerve block anesthesia). Before local anesthesia, 0.3 µg/kg dexmedetomidine micropump was infused within 15 min by the anesthesiologist, followed by the intravenous injection of 5 mg dezocine, and then the ophthalmologist injected 3 mL of 1:1 mixture of 2% lidocaine and 0.1% ropivacaine for infraorbital nerve block anesthesia, 3 mL of the mixture for infratrochlear nerve and anterior ethmoidal nerve anesthesia. During the operation, 0.3 µg/kg/h dexmedetomidine micropump infusion was maintained by the anesthesiologist, with oxygen inhalation via a mask at a flow rate of 3–4 L/min.
The GA group was given general anesthesia. Induction of anesthesia was achieved as follows: the anesthesiologist intravenously injected fentanyl 2 µg/kg, propofol 2 mg/kg, and rocuronium 0.06 mg/kg in turn. After successful induction, the laryngeal mask airway was inserted. Ventilatory parameters were set up as shown below: oxygen flow 1 L/min, tidal volume 6–8 mL/kg, respiratory rate 12–14 breaths/min, inspiratory and expiratory ratio 1:2, peak airway pressure < 25 cm H₂O, and PetCO₂ 35–45 mmHg. Subsequently, anesthesia was maintained with a continuous inhalation of 1%–2% sevoflurane, intravenous pump injection of remifentanil 0.1–0.3 μg/ (kg • min); the depth of anesthesia was timely adjusted according to the operation and the patient’s vital signs.
Nasal endoscopic DCR was performed by the same group of doctors after the onset of anesthesia in both groups.
Outcome measures
Mean arterial pressure (MAP) and heart rate (HR): before anesthesia (T0), after the implementation of anesthesia (T1), at the beginning of surgery (T2), and at the end of surgery (T3) at four time points, MAP and HR were recorded separately for both groups.
Visual analogue scale (VAS) 10 and adverse reactions: VAS (rating scale: 10 as severe pain; 5–9 as unsatisfactory analgesia; 3–4 as basic satisfaction; 1–2 as satisfactory analgesia; 0 as no pain) and adverse reactions (including agitation, nausea, and vomiting) were recorded after awakening from anesthesia and at 1, 2, 6, and 12 h postoperatively.
Sedation and agitation score (SAS) 11 : The SAS score was performed immediately after awakening, and the assessment criteria: 1 as unresponsive; 2 as deeply sedated; 3 as sedated but easily awakened; 4 as calm and cooperative; 5 as agitated and calm to verbal instructions; 6 as agitated and in need of restraint; and 7 as dangerously agitated.
Statistical analysis
Statistical software SPSS 23.0 was used for statistical analysis. Measurement data were expressed as mean ± standard deviation (SD), and an independent sample t test compared the means of the two groups. Enumeration data was expressed as n (%) and χ2 test was used for comparison. P < 0.05 was considered statistically significant. Repeated measure analysis of variance could be used for comparison of the parameters at the same time point.
Results
Baseline data of two groups
Comparison of baseline data between two groups.

Data was n or mean ± SD.
Abbreviation: LA, local anesthesia; GA, general anesthesia.
Mean arterial pressure and heart rate at different time points in the two groups
During each period of anesthesia (T0–T3), HR and MAP in the LA group remained relatively stable, while in the GA group, there was a trend that HR and MAP first decreased during T1 and T2 and then increased rapidly during T3. This result indicated that HR and MAP were more stable during anesthesia in the LA group and were closer to the pre-anesthesia level.
Mean arterial pressure and heart rate at different time points in the two groups.
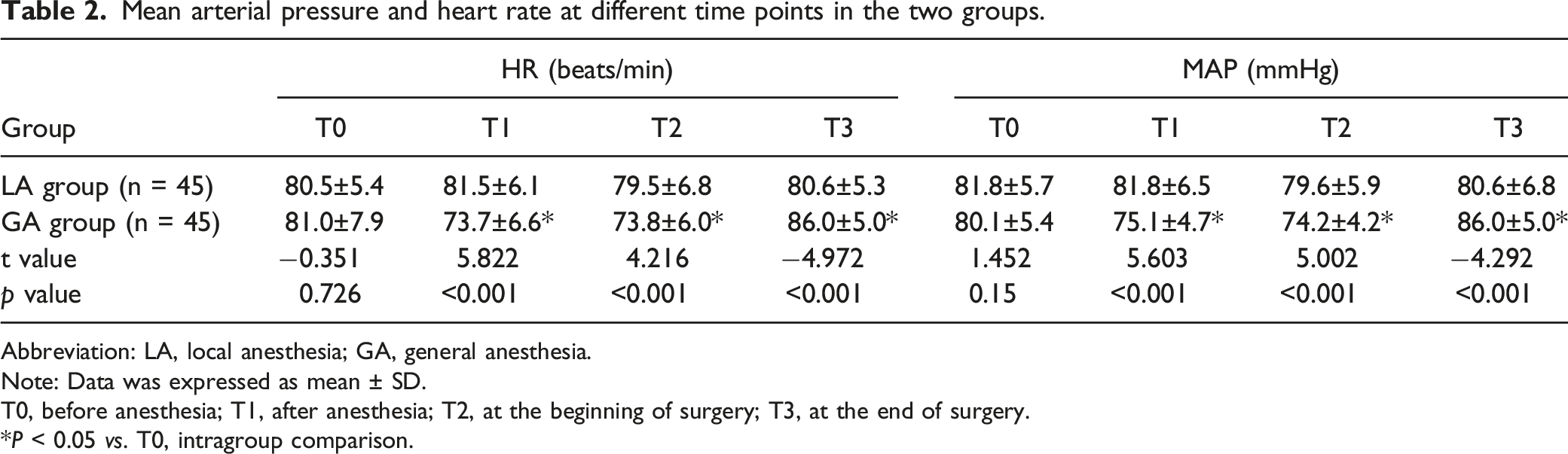
Abbreviation: LA, local anesthesia; GA, general anesthesia.
Note: Data was expressed as mean ± SD.
T0, before anesthesia; T1, after anesthesia; T2, at the beginning of surgery; T3, at the end of surgery.
*P < 0.05 vs. T0, intragroup comparison.
Postoperative VAS scores at different time points between the two groups
Comparison of postoperative VAS score at different time points in the 2 groups.
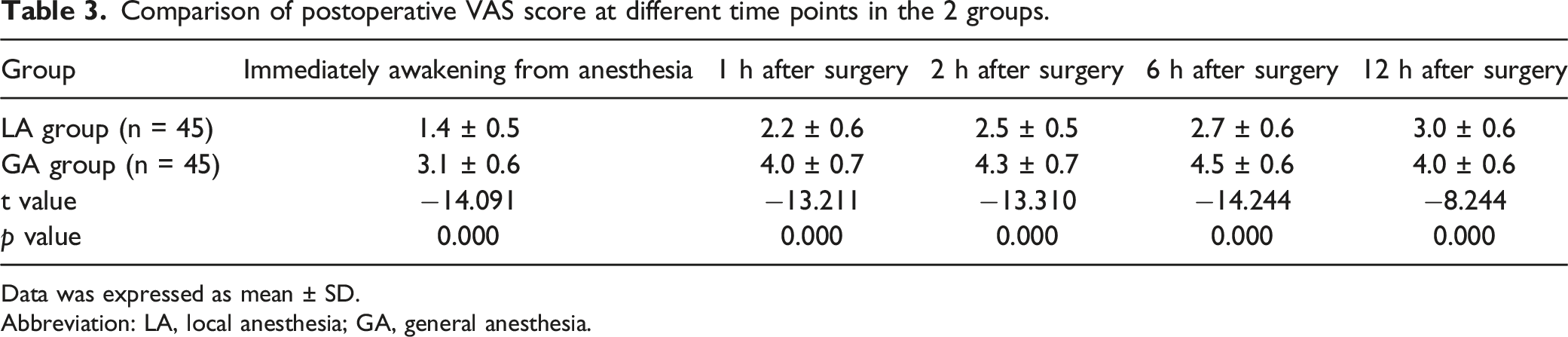
Data was expressed as mean ± SD.
Abbreviation: LA, local anesthesia; GA, general anesthesia.
Incidence of postoperative adverse reactions and SAS score in the 2 groups
Comparison of postoperative adverse reactions and SAS score between the two groups.
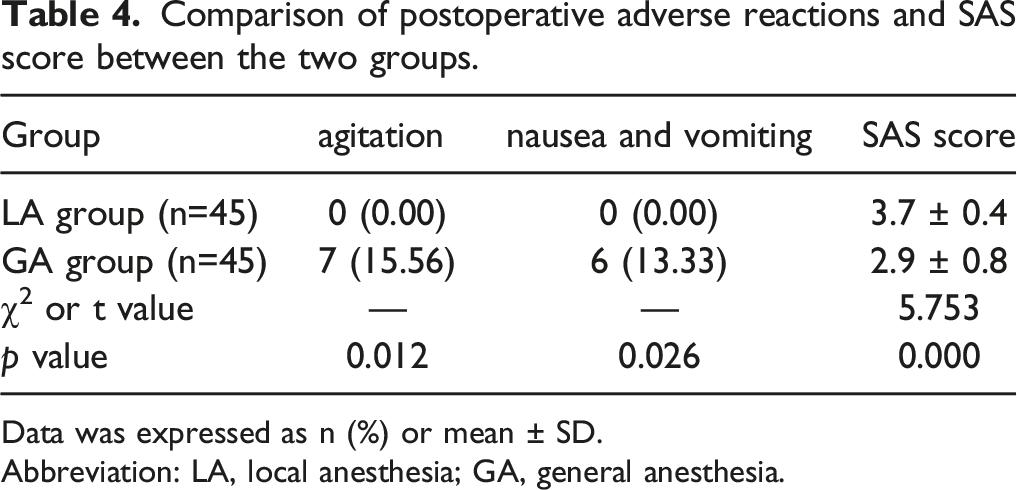
Data was expressed as n (%) or mean ± SD.
Abbreviation: LA, local anesthesia; GA, general anesthesia.
And the SAS score of LA group was kept at 3–4 (sedation and calm cooperation), which was significantly higher than that of GA group; the GA group of general anesthesia had 7 patients who were agitated, but the rest were mostly in deep sedation and had lower VAS score. It is suggested that patients are more likely to maintain a better mental state after local anesthesia (Table 4).
Discussion
According to research and practice on nasal endoscopic DCR for patients with chronic dacryocystitis, anesthetic effect is an important basis for the smooth progress of the surgery. General anesthesia is an anesthesia method used more frequently in endoscopic DCR, which can effectively assist the smooth operation. Nevertheless, this type of anesthesia causes a high frequency of adverse reactions such as agitation, nausea, and vomiting, and easily leads to rebleeding of the surgical wound, nasal stoma blockage, and other conditions, seriously affecting the success rate of surgery. Thus, general anesthesia is gradually replaced by local anesthesia. 12 However, it is found that after simple local anesthesia for nasal endoscopic DCR, patients have poor analgesic effects, excessive drug use, and heavy toxic reactions. What is more, patients have mental stress and greater stress response, which has a certain impact on their life safety. Given those limitations, rational use of sedative, hypnotic, and analgesic drugs to assist local anesthesia is an effective method to ensure a comfortable surgery.
Most of the patients with dacryocystitis are middle-aged and elderly and they often suffer from systemic diseases. 13 Therefore, these patients are at a relatively high risk of surgery under general anesthesia. Also, the cost of general anesthesia is high. Thus, patients prefer local anesthesia, but they cannot cooperate well during the surgery due to tension, fear, pain, and other discomfort. Poor cooperation will result in great hemodynamic fluctuations and intraoperative bleeding, thus affecting surgical operation and prolonging operation time. These are common problems for ophthalmologists and anesthesiologists to solve, which include: how to reduce patients’ intraoperative pain, anxiety, and fear, how to decrease negative stimuli, and how to minimize the incidence of adverse reactions. Enabling patients receiving local anesthesia to achieve physical and psychological comfort is the ultimate aim.
Studies have shown that midazolam, fentanyl, and propofol to assist local anesthesia for endoscopic DCR can replace general anesthesia surgery. 14 Thus, this study has selected the appropriate combination of drugs to explore a new safe and effective anesthetic method for endoscopic DCR. Several studies have found that patients treated with dexmedetomidine show more stable intraoperative anesthesia, good sedative effect, stable hemodynamics, and fewer adverse reactions. 15 Additionally, it has been reported that dexmedetomidine combined with dezocine is a safe and effective method in thoracoscopic gynecological surgery under general anesthesia, which can make the hemodynamics of patients more stable and improve the cure rate of patients. 16 Thus, we selected dexmedetomidine combined with dezocine in local anesthesia for endoscopic DCR, so as to improve the anesthesia method for this surgery.
This study found that MAP and HR at T1 and T2 were significantly lower in the LA group compared with the GA group, indicating that patients had more stable hemodynamics after local anesthesia. In this study, the local anesthesia was achieved by using lidocaine and ropivacaine to anesthetize the anterior ethmoidal nerve, infraorbital nerve, and infratrochlear nerve. This method can anesthetize the skin at the inner canthus, conjunctiva, lacrimal sac, anterior part of nasal lateral wall, ethmoidal sinus, and anterior portion of middle turbinate. The combination of the 2 drugs can shorten the onset time of anesthesia to 3–5 min, and the anesthesia effect can be maintained 4–6 h, which effectively ensures the operation goes smoothly.
This study observed that local anesthesia was associated with a lower incidence of adverse reactions including postoperative agitation, nausea, and vomiting. The SAS score was significantly higher in patients with local anesthesia. These effects are closely related to the drug properties and metabolism of dexmedetomidine and dezocine. Clinically, dexmedetomidine is mostly used for sedation in patients who are required to use intubation and ventilators during intensive care treatment. 17 Dexmedetomidine is a highly selective α-adrenoceptor agonist with sedative and analgesic effects. This agonist has a unique sedative mode—awake sedation. In other words, patients can be easily awakened and communicated when stimulated.18,19 This is the only drug with an electroencephalogram pattern similar to that of natural non-rapid eye movement sleep. 20 Dezocine also has an anethetic effect, which is a κ receptor agonist and a partial μ receptor antagonist/agonist. 21 Dezocine is not only less addictive, but also has better analgesic effect and less incidence of adverse reactions. 22 Additionally, dezocine acting as a partial agonist of μ receptor produces no μ receptor dependence. 23 For advantages given above dezocine is widely used for pain management. Moreover, dezocine has a mild sedative effect and no respiratory depression, which can relax gastrointestinal smooth muscles and reduce the incidence of nausea and vomiting. To conclude, dexmedetomidine combined with dezocine provides more stable hemodynamics during surgery for patients with dacryocystitis. The synergistic effect of these two anesthetic drugs can achieve better sedative and analgesic effects. The initial injection rate of dexmedetomidine is recommended to be 0.7 µg/kg/h, and can be gradually adjusted in the range of 0.2–1.4 µg/kg/h to achieve the ideal level of sedation. 24 As the study by Jia et al. 25 has shown, dexmedetomidine 0.3 µg/kg/h combined with remifentanil was effective in colonoscopy with few adverse effects, while 0.4 µg/kg/h dexmedetomidine combined with remifentanil had the risk of deeper sedation in colonoscopy. Therefore, we selected dexmedetomidine 0.3 µg/kg/h combined with dezocine for local anesthesia in nasal endoscopic DCR.
Since nasal endoscopic DCR is performed in the nasal cavity, blood enters the respiratory tract from the nasopharynx after intraoperative bleeding, thus causing a high risk of aspiration. In order to prevent surgical aspiration, we packed the choanae with brain cotton during surgery, but some blood still penetrates into the oral cavity, so the control of surgical analgesia and sedation depth is vital. The ideal depth is that the patient is not asleep and can be awakened at any time. To this point, the awake sedation of dexmedetomidine meets our needs. Moderate sedation can greatly reduce the potential for aspiration during surgery.
The sedative effect of dexmedetomidine is dose-dependent. In this study, we used low-dose drugs before and during the surgery to achieve moderate sedative effect. The patients were conscious during the whole operation, and the stress response of the patients was inhibited and hemodynamics were stable during the surgery. We only used 0.3 µg/kg/h of dexmedetomidine but failed to compare the anesthetic efficacy of different doses of dexmedetomidine combined with dezocine. There were several patients with insufficient depth of sedation and, consequently, unpleasant experiences during the procedure. Therefore, in future clinical practice, individual differences in relation to drug dosage will be further investigated.
This study suggests that dexmedetomidine combined with dezocine has a better analgesic effect, low adverse effects, and maintains a relatively good mental state after awakening. Therefore, this anesthetic method has some prospects for clinical development. However, this study also has the following shortcomings: (1) few cases were included, which may affect the accuracy of the results due to individual differences, so a larger sample needs to be included in subsequent studies; (2) intravenous dezocine may cause respiratory depression, and this study did not observe this adverse effect.
Conclusions
In summary, dexmedetomidine combined with dezocine for local anesthesia in endoscopic DCR has more stable hemodynamics and reduces intraoperative stress response and intraoperative bleeding. Additionally, this type of anesthesia achieves effective postoperative sedation and analgesia, less postoperative nausea and vomiting and other adverse reactions, and better quality of awakening from anesthesia. Collectively, this local anesthesia is a comfortable and safe option for patients who are at high risk of general anesthesia and unwilling to receive general anesthesia.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.