
Abstract
Angiomyolipoma is an extremely rare, benign mesenchymal tumor of the nasal cavity, primarily common in the kidney and secondarily common in the liver. According to the author’s knowledge, no cases of angiomyolipoma of the nasal septum have been identified to date. We report a case of a patient with a giant angiomyolipoma at the posterior end of the nasal septum who recovered after surgery without any complication.
Keywords
Introduction
Angiomyolipoma (AML) is a spindle cell tumor composed of vascular, smooth muscle, and fat components in varying proportions; it is more common in adults and in women than in their counterparts. According to these varying proportions, AML can be divided into mixed, smooth muscle, fatty, and vascular types. AML is most common in the kidney and rarely occurs in the nasal cavity; cases with AML originating from the nasal septum have not been reported.
Case report
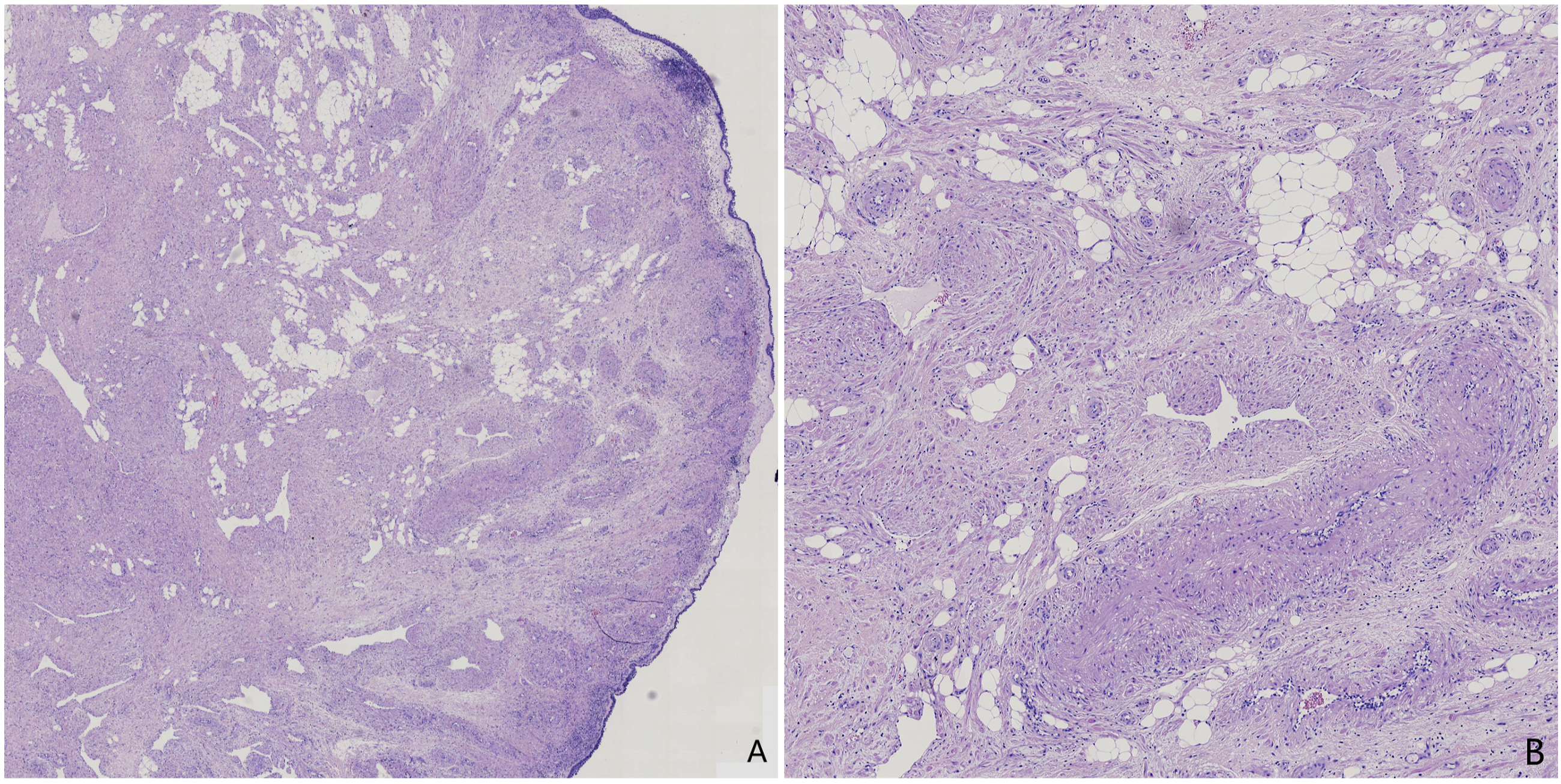
A 51-year-old woman presented with a 2-month history of nasal congestion, which was gradually worsening, with no runny nose and intermittent nosebleed, and no other positive signs. Electronic nasopharyngoscopy revealed a large mass protruding into the nasopharynx at the posterior end of the left nasal septum (Figure 1A). Computed tomography of the improved sinuses showed a promiscuous dense mass at the posterior end of the left nasal cavity (Figure 1B). The mass was first considered a hemangioma. Enhanced magnetic resonance imaging (MRI) confirmed a mass measuring approximately 3.5 × 2.7 × 2.9 cm in the posterior part of the left nasal cavity. This mass had mixed density long and short T1 and long T2, with uneven and obvious enhancement on MRI (Figure 1C). After excluding the possibility of a hemangioma, we formulated a surgical plan to resect the tumor under nasal endoscopic guidance. Intraoperatively, the root of the tumor was found at the posterior end of the left nasal septum, which was prone to bleeding when touched. The tumor and the nasal septum mucosa of the root were removed together (Figure 1D), and the patient’s symptoms were relieved after surgery. Pathology revealed the presence of thick-walled vessels, fat cells, and broad spindle cells, consistent with AML features (Figure 2). Immunohistochemistry results were as follows: S100 (−), HMB45 (−), CD34 (+), SMA (+), and HHF35 (+). Computed tomographic and clinical images (A) Preoperative laryngoscopic image; (B) CT showed a nasal septum mass; (C) Enhanced magnetic resonance imaging showed significant uneven enhancement of the mass; (D) Nasal septum mass. Hematoxylin-eosin stains (A) Original magnification ×20; (B) Original magnification ×200, hematoxylin-eosin stained section of nasal duct smooth mylipoma, showing accumulation of thick-walled vessels, spindle cells and adipocytes.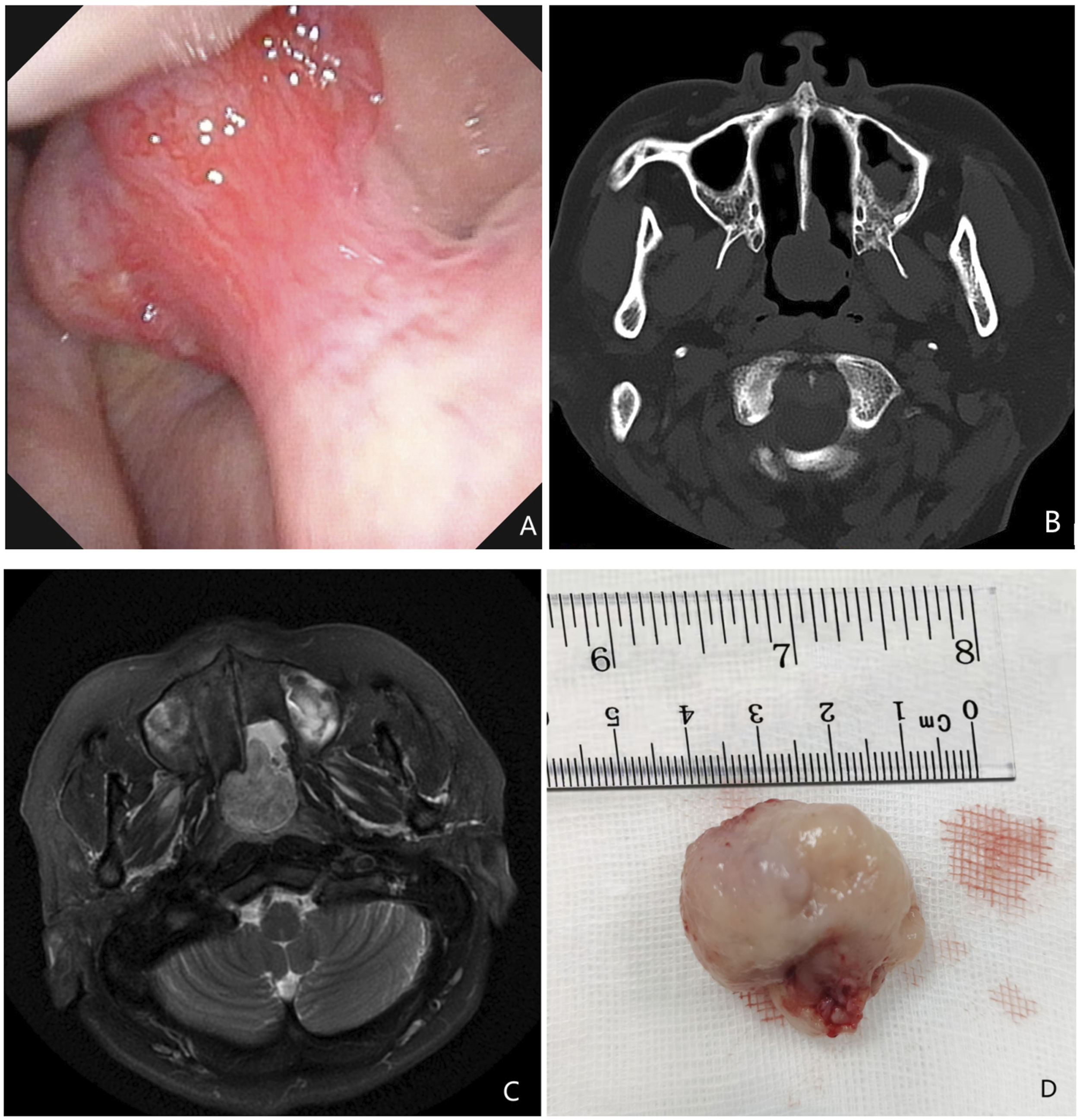
Discussion
AML in the nasal cavity is very rare, with fewer than 20 cases reported worldwide. It was first reported by Dawlatly 1 in 1988; since then, there have been only scattered reports reported domestically and worldwide.2-4 There are no similar reports about the posterior nasal septum. AML of the nasal cavity has no unique clinical manifestations; since this case presented is similar to hemangioma, hemangioma should be considered during differential diagnosis. The definitive diagnosis should be confirmed pathologically. Microscopically, smooth muscle, mature adipocytes, and vascular aggregates of varying thickness can be observed. Immunohistochemical staining with melanin-specific antibody HMB45 is generally positive in liver and kidney AML tissues, and the degree of HMB45 positivity gradually decreases with the differentiation of muscle cells into spindle cells. However, in this case of nasal AML, HMB45 staining was negative. This finding was consistent with previous reports, 5 which may be because mostly mature spindle cells were present in the tumor. The accepted treatment for nasal AML is surgical resection, and few patients have experienced recurrence. The current number of known cases are few, and the clinical manifestations and immunohistochemical characteristics of the disease still require further study and discussion to guide treatment.
Footnotes
Author contributions
Dr Dong Liu had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis; Concept and design: Fengxian An, Maocai Li, Lianqing Li, Lili Gong, Xia Liu, Fuxing Liu; Acquisition, analysis, or interpretation of data: All authors; Drafting of the manuscript: Dong Liu; Critical revision of the manuscript for important intellectual content: Fuxing Liu.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This article was approved by the Ethics Committee of Liaocheng People’s Hospital.
Informed consent
The patient provided us informed consent for the publication of this case report.