
Abstract
Objectives
To identify the differences in hearing, anatomical success rate, functional success rate, and complications between over-under tympanoplasty and medial tympanoplasty procedures.
Methods
The clinical data of patients with tympanic membrane perforation repaired by medial tympanoplasty between January 2011 and December 2016 and by over-under tympanoplasty between January 2017 and December 2020 were retrospectively analyzed. We evaluated the differences between medial tympanoplasty and over-under tympanoplasty.
Results
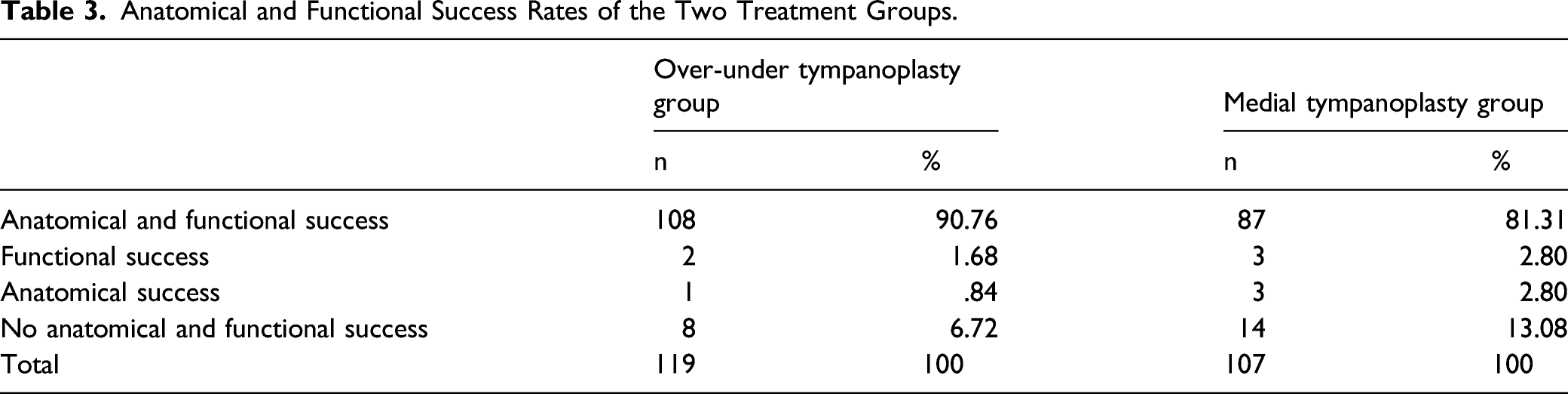
The overall success rate of over-under tympanoplasty was higher than that of medial tympanoplasty (90.76% vs 81.31%). In large perforations, the success rate of over-under tympanoplasty was higher than that of medial tympanoplasty (89.80% vs 71.43%). There was no statistically significant difference in the success rate between the two treatment groups for moderate perforations. Furthermore, there was no statistically significant difference in the incidence of complications between the two groups (P = .2637).
Conclusions
Over-under tympanoplasty is more suitable for large perforations of the tympanic membrane and has a higher success rate as compared to medial tympanoplasty.
Introduction
Tympanoplasty is the repair of a perforated eardrum using the tissue transplantation technique, which restores the integrity of the eardrum and anatomy and function of the middle ear, thus improving the hearing and quality of life. Many authors have modified tympanoplasty in terms of the approach, technique, and materials used for grafting the tympanic membrane. Every method has its advantages and disadvantages.1-3 Nevertheless, subtotal and total perforations have always posed a challenge to otologists. Depending on the size of the perforation and indications, several surgical methods are used, such as overlay, medial, interlayer, and over-under tympanoplasty.4,5 The most common method is medial (underlay) tympanoplasty, wherein the repair material is placed on the inner side of the perforated tympanic membrane and the malleus handle. The over-under tympanoplasty procedure was first reported by Kartush et al. 6 in 2002, wherein the malleus is separated from the tympanic membrane, and the repair material is placed between the residual tympanic membrane and malleus. Over-under tympanoplasty has been performed in our department since 2017 to repair tympanic membrane perforations and has shown good results. This study analyzed and compared the efficacy and complications of over-under tympanoplasty and medial tympanoplasty in the repair of tympanic membrane perforations.
Patients and Methods
Study population
The clinical data of patients with tympanic membrane perforation repaired by medial tympanoplasty between January 2011 and December 2016 and by over-under tympanoplasty between January 2017 and December 2020 at the Affiliated Hospital of Qingdao University were analyzed retrospectively. In this study, tympanic membrane perforation was defined as a perforation area greater than one-third of the tympanic membrane area. The inclusion criteria were no ear discharge for at least 1 month, intact middle ear mucosa, no signs of clinical or radiological infection, no cholesteatoma, no ossicular chain pathology with intact and mobile ossicular chain, satisfactory eustachian tube function, and quiescent underlying disease process. Patients who underwent mastoidectomy, ossicular reconstruction, or cholesteatoma surgery were excluded. The adoption of medial tympanoplasty and over-under tympanoplasty showed a clear temporal division (before 2017 vs after 2017). The study protocol was approved by the Institutional Review Board of the hospital.
Methods
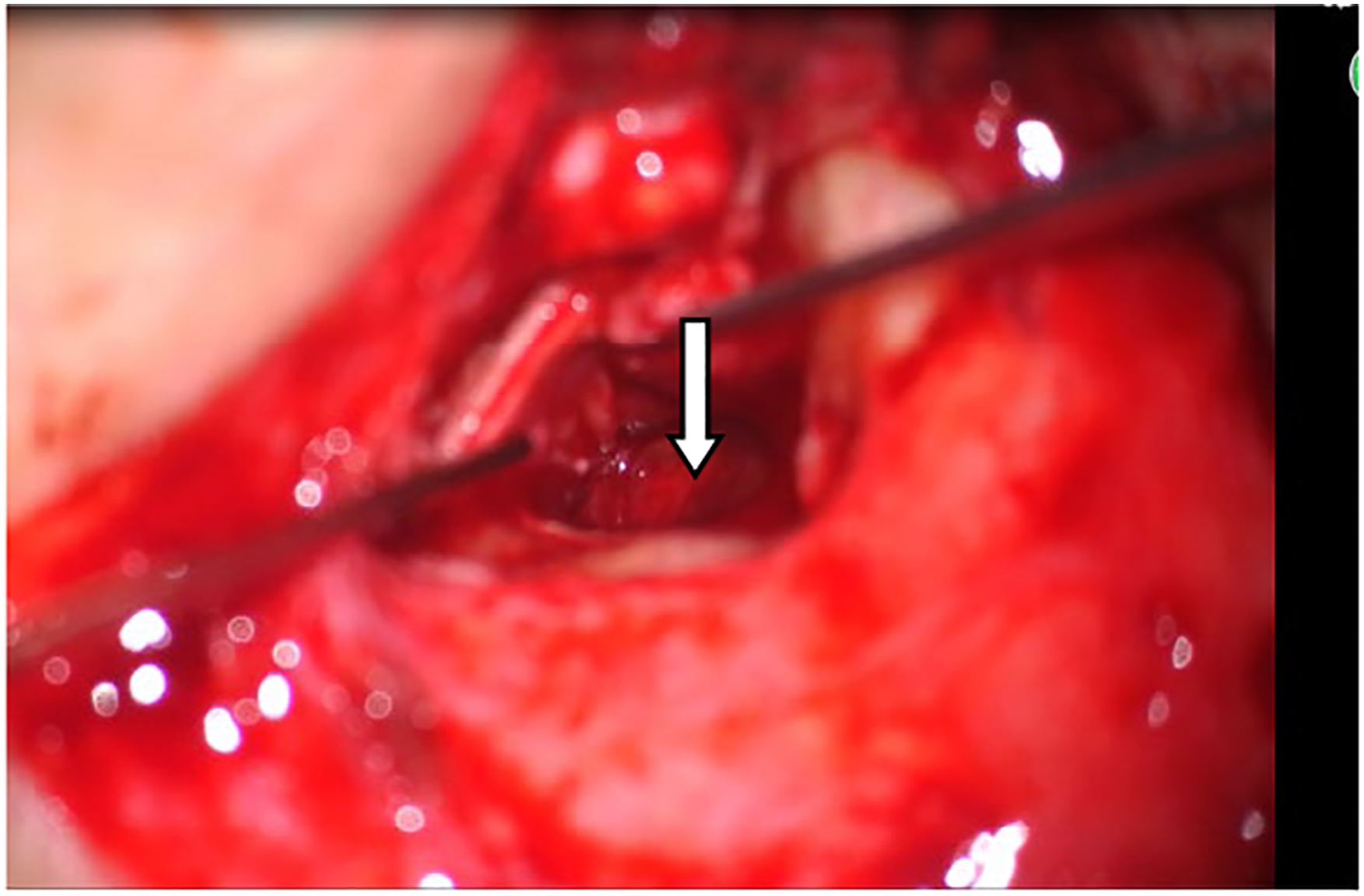
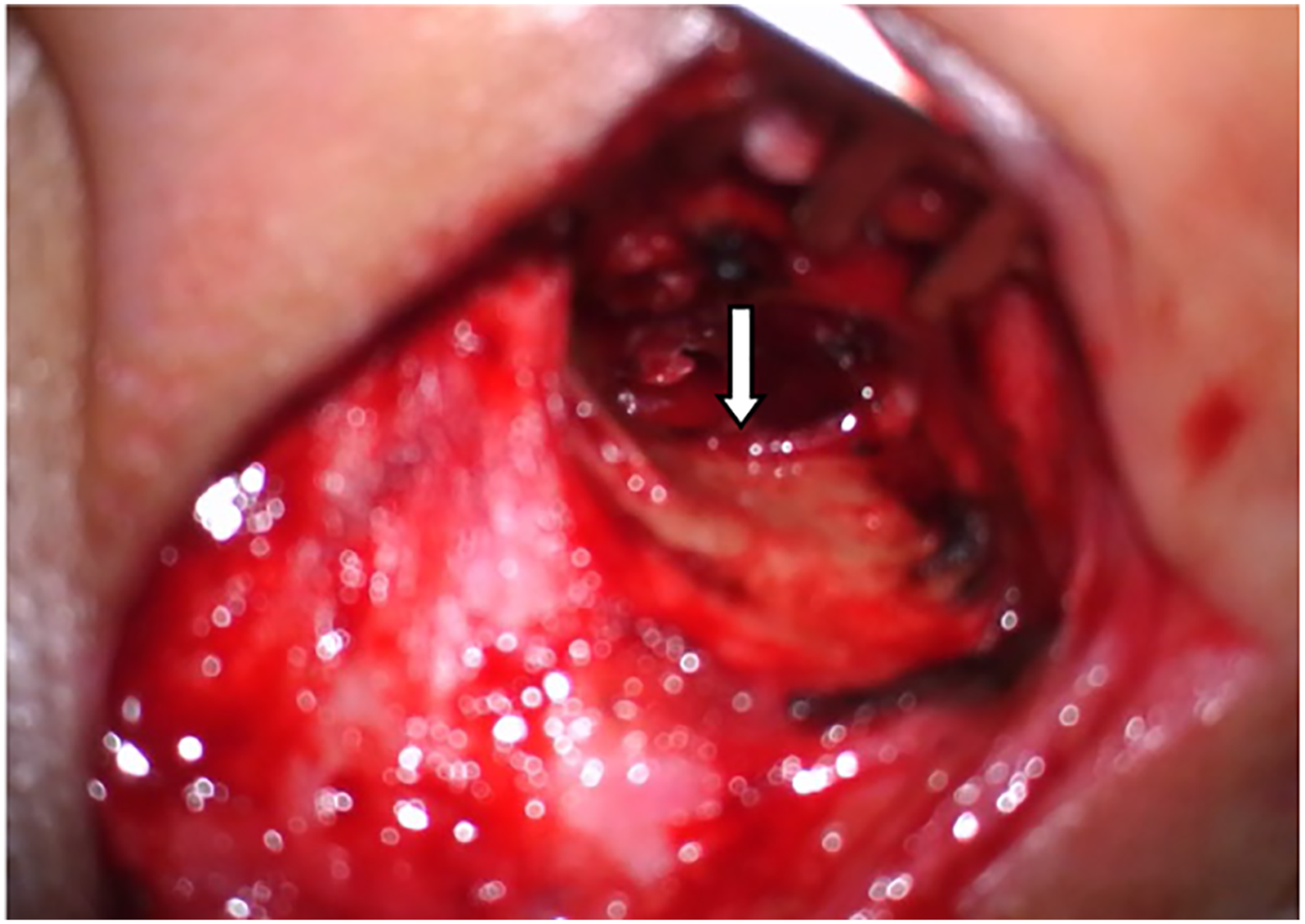
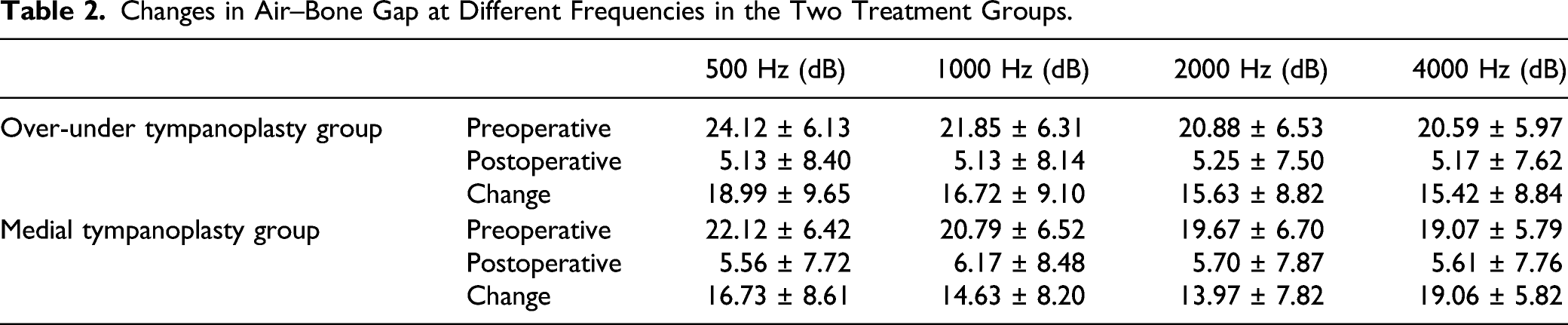
The conventional preoperative examinations, including computed tomography of the ear, pure-tone audiometry, and eustachian tube function, were performed for all patients. They underwent preoperative and postoperative pure-tone audiometry measurements at 500, 1000, 2000, and 4000 Hz frequencies. The preoperative and postoperative air and bone conduction thresholds were measured for these four frequencies. The air–bone gap (ABG) was calculated as the average difference between the air and bone conductions at these frequencies. Based on the size of the perforation area, the tympanic membrane perforation was classified as moderate perforation (1/3< perforation area ≤3/4) and large perforation (perforation area >3/4 or complete perforation). All surgeries were performed under general anesthesia via the postauricular approach. The temporalis fascia was harvested for the graft tissue. A rim of the tissue was removed from the perforation edge, and the edges were freshened to de-epithelialize and encourage migration of the mucosal layer and epithelium. The tympanomeatal flap was elevated to gain access to the tympanic cavity. In over-under tympanoplasty, the tympanic membrane remnant was elevated from the malleus (Figure 1), and the anterior annulus and meatal skin were elevated in cases with little or no edges in the front. In contrast, in medial tympanoplasty, the tympanic membrane remnant was not elevated from the malleus. The temporalis fascia graft was placed lateral to the long process of the malleus and medial to the tympanic membrane remnant and anterior annulus in the over-under tympanoplasty group (Figure 2). In the medial tympanoplasty group, it was placed medial to the tympanic membrane remnant and malleus (Figure 3). The middle ear was packed with Gelfoam soaked in antibiotic solution and dexamethasone. Finally, the external auditory canal was packed with Gelfoam, and the wound was closed. The tympanic membrane remnant is elevated from the malleus. (Arrow indicates the malleus handle). The temporalis fascia graft is placed lateral to the long process of the malleus and medial to the tympanic membrane remnant and anterior annulus. (Arrow indicates the temporalis fascial graft). The temporalis fascia graft is placed medial to the tympanic membrane remnant and the malleus. (Arrow indicates the temporalis fascial graft).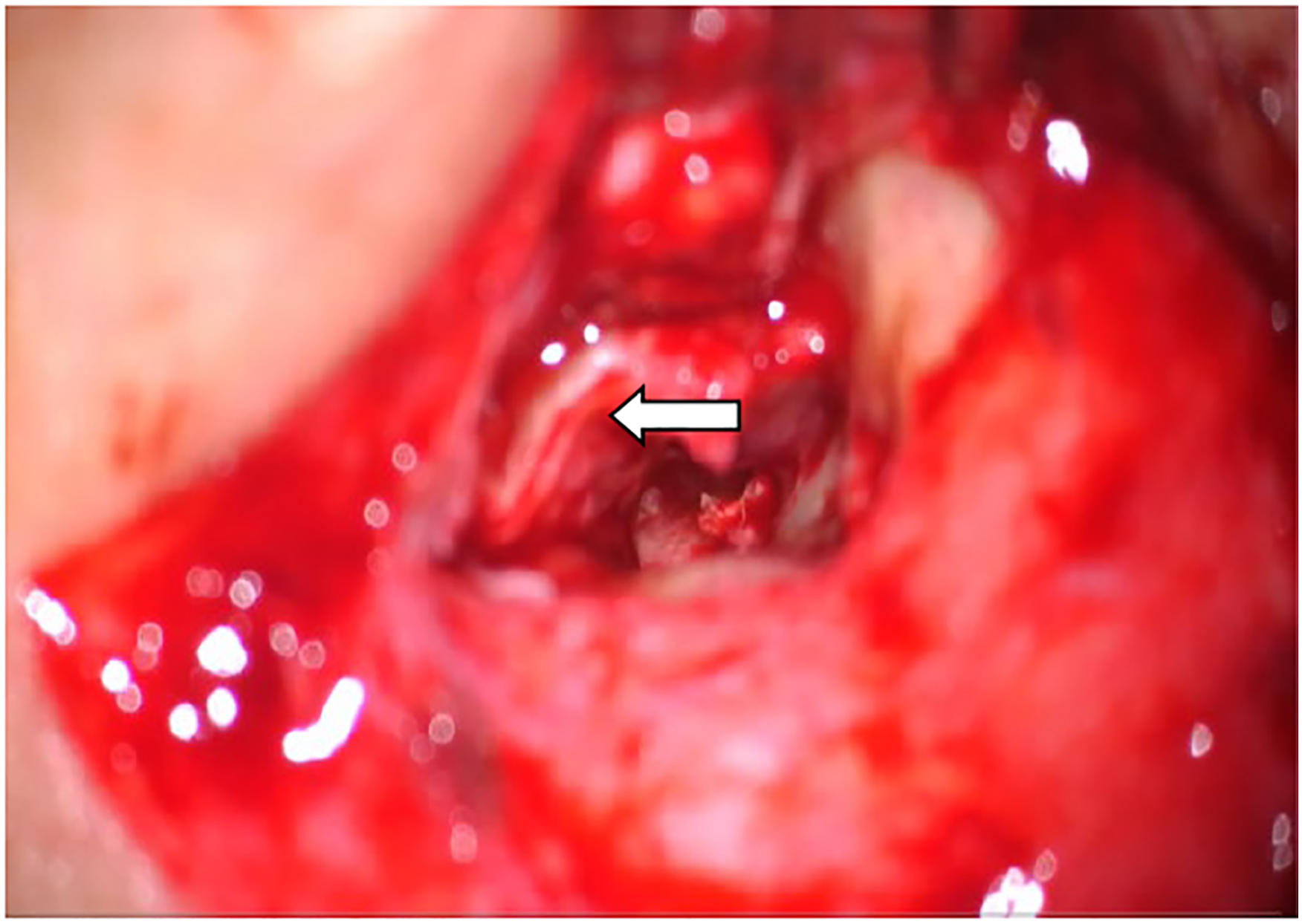
Follow-up visit and data collection
Successful tympanic membrane repair is defined by the following three factors: (1) complete graft; (2) postoperative ABG <10 dB or hearing returned to normal; and (3) complete healing, with ventilation space in the middle ear, graft in the correct anatomical position, and no tympanic membrane at electasis or secretory otitis media. Closure of the tympanic membrane, changes in hearing, and complications were the main outcome measures. Tympanic closure was classified as anatomical success if a closed tympanic membrane was noted during the follow-up period. The follow-up period was at least 12 months. A successful functional result was defined as postoperative ABG <10 dB. Differences in age, sex, changes in hearing, anatomical success rate, functional success rate, and complications were assessed between the over-under tympanoplasty and medial tympanoplasty groups.
Statistical analysis
The data were analyzed using Statistical Product and Service Solutions software (version 20.0; IBM Corp, NY, USA). Chi-square test was used for analyzing categorical variables and t-test for continuous variables; P-values <.05 were considered statistically significant.
Results
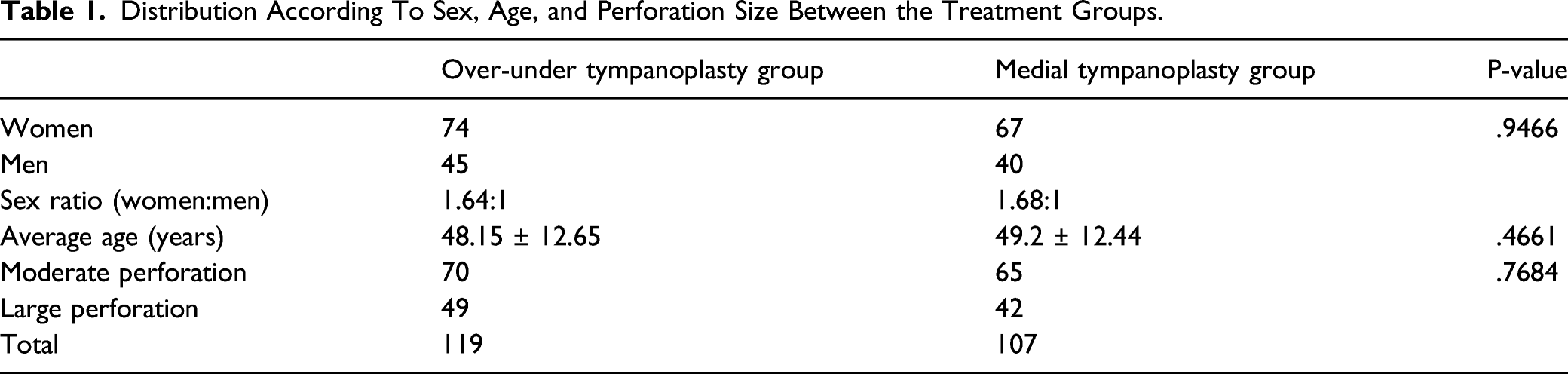
Distribution According To Sex, Age, and Perforation Size Between the Treatment Groups.
Changes in Air–Bone Gap at Different Frequencies in the Two Treatment Groups.
Anatomical and Functional Success Rates of the Two Treatment Groups.
Success and Failure Rates of Moderate and Large Perforations in the Two Treatment Groups.

The medial tympanoplasty group comprised 42 large perforation cases, including 30 successful (71.43%) and 12 unsuccessful (28.57%) cases, and 65 cases of moderate perforations, including 57 successful (87.69%) and 8 unsuccessful (12.31%) cases. There was a significant difference between the moderate and large perforations in the medial tympanoplasty group (P = .0351) (Table 4).
There was a statistically significant difference in the overall success rate and success rate of large perforations between the two groups (P = .0393 and .025, respectively) but not in that of moderate perforations (P = .4768).
The incidence of complications in the two groups was low. The malleus handle separated from the tympanic membrane in one patient (.84%) of the over-under tympanoplasty group, whereas adhesion to the inner wall of the tympanic cavity was observed in three patients (2.80%) of the medial tympanoplasty group. There was no statistically significant difference in the incidence of complications between the two groups (P = .2637).
Discussion
Tympanoplasty was first reported by Berthold in 1878. 7 With the progress in science, its repair materials, methods, techniques, and other aspects have greatly improved. Different types of graft materials have been used in tympanic membrane reconstruction, including the temporalis fascia, papillary periosteum, cartilage, perichondrium, vein, fat, skin, dura mater, and xenografts. 8 The temporalis fascia is the most commonly used graft material in our department. Temporalis fascia repair is favored by clinicians because of its advantages of high success rate, easy access to a large area of repair materials, proximity to the surgical area of repair, thickness similar to that of the tympanic membrane, embryologic derivation from the mesoderm, and no vibration-limiting effects caused by sound waves on the tympanic membrane.9-12
Medial tympanoplasty is the most widely used method because of its ease of operation and high success rate, often achieving a success rate >80%. However, it depends on the surgeon’s skills and expertise, graft, position and size of the perforation, status of the eustachian tube function, and other factors. Iso-Mustajarvi et al. 11 compared the success rate of medial tympanoplasty using different materials and found that the success rate with temporalis fascia and perichondrium was approximately 85.7%, whereas that with perichondrium with cartilage and fat was 61.9% and 71%, respectively. Alharbi et al. 13 concluded that the success rate of medial tympanoplasty using temporalis fascia or thin tragal cartilage with the perichondrium was 94%. Moreover, Hsu et al. 3 found that the success rate of medial tympanoplasty could be >90% with either microscopic or endoscopic methods. Despite its high success rate, medial tympanoplasty is technically challenging. The graft is placed medially under the residual tympanic membrane and malleus handle. Hence, the tympanic volume is reduced, especially in patients with a narrow tympanic cavity, thus increasing the risk of otopiesis and adhesion. Additionally, anterior perforations and large perforations affect the visual field of the implant due to obstruction of the malleus. In this study, the success rate of medial tympanoplasty was 81.31%, with a success rate of 87.69% for moderate perforations and 71.43% for large perforations, highlighting an obvious difference between them. Three patients presented different degrees of otopiesis and adhesions. Surgical failures are difficult to avoid in large perforation cases because of the increased technical difficulty and the area that needs vascularization. The larger the perforation, lower is the success rate. Salcan 12 found that graft success was lower in total perforations than in the other perforation types. A retrospective study by Lee et al. 14 of 423 myringoplasty-only operations showed that the perforation size influenced surgical success; the success rate for small perforations was 74.1% compared to the 56.0% for large perforations (P = .0003). Anterior and edge perforations and large perforations have low success rates because of the less wounded edge and limited visual field. 15 Thus, their clinical application is limited.
Over-under tympanoplasty has been widely used since its introduction by Kartush et al. It has the following advantages: (1) it is ideal for perforations of all sizes in all quadrants of the tympanic membrane; (2) it involves excellent exposure, especially in the anterior middle ear; (3) it minimizes the risk of graft lateralization and anterior angle blunting; (4) it has a high success rate; (5) it is a relatively simple technique; and (6) the middle ear space is not reduced, thus minimizing adhesions from the drum to the promontory.6,16-18
Most studies found that the success rate of over-under tympanoplasty was significantly higher than that of medial tympanoplasty, especially in large, anterior, and marginal tympanic membrane perforations. 19 However, some scholars believe that the success rate of over-under tympanoplasty is comparable to that of medial tympanoplasty. 20 In this study, the success rate of over-under tympanoplasty was significantly higher than that of medial tympanoplasty (90.76% vs 81.31%; P < .05). The difference in the success rate between the two groups was greater for near-total or total perforations of the tympanic membrane than for moderate perforations. Moreover, no obvious difference was observed between the moderate and large perforations in the over-under tympanoplasty group. The over-under tympanoplasty method was more advantageous in repairing large and anterior perforations because of the clear visual field exposure. This corroborated the findings of Babu et al. 16 Yigit et al. 21 reported success rates of 94.9% and 91.5% in the over-under tympanoplasty and underlay groups, respectively. They considered over-under tympanoplasty to be superior to the other two classical methods (underlay and overlay) not only because of its effectiveness, but also because of the results achieved using this technique. Jung and Parks, 22 using a mediolateral graft method to repair subtotal and anterior perforations, demonstrated 97% eardrum closure and reported complications in 5 of 100 cases. An important difference between the over-under tympanoplasty and medial tympanoplasty methods is the separation of the residual tympanic membrane from the malleus. This leads to the following conditions: (1) increased overlap of the graft and the remnant tympanic membrane, with the graft material fitting more closely to the edge of the tympanic membrane; (2) increased wound surface area for better preparation of the graft bed, which is beneficial for growth; (3) precise graft placement guided by the malleus; and (4) excellent medial support provided by the malleus handle to prevent displacement. The malleus handle acts as an additional point of graft fixation to lower the risk of graft retraction6,11; thus, the malleus becomes an asset rather than a liability.
If the patient also has ossicular chain pathology, over-under tympanoplasty is more beneficial than medial tympanoplasty for reconstructing the ossicular chain. Owing to the graft position, over-under tympanoplasty is ideally suited for ossicular chain reconstruction. The availability of the medial surface of the malleus is advantageous, because it allows direct contact between the prosthesis and malleus. This helps “lock” the prosthesis to minimize extrusion or displacement. 6 Therefore, the application scope of over-under tympanoplasty is more extensive than that of medial tympanoplasty. It is advantageous for very large tympanic membrane perforations, extensive middle ear cholesteatoma, or other disease processes extending anterior to the malleus but is not necessarily indicated for limited middle ear disease or small posterior perforations.
To avoid complications and improve the success rate of the repair, some caution should be exercised during over-under tympanoplasty. After generating the wound surface of the residual tympanic membrane, the involution of the epithelial layer should be avoided to prevent the formation of cholesteatoma. The malleus handle should be carefully dissociated, and a sharp crochet needle should be used to separate the malleus handle from the tympanic membrane to avoid neurological deafness. If no or less residual rim is found in front of the tympanic membrane, the anterior external auditory meatus flap should be lifted, and the repair material should be placed below the tympanic membrane flap of the anterior external auditory meatus. Filling materials, such as Gelfoam, should not be placed between the repaired graft and the malleus handle to avoid separation between the tympanic membrane and malleus handle. It is important to avoid overpacking the Gelfoam because this may theoretically increase the risk of tympanic membrane lateralization. After the repaired tympanic membrane is reset, the malleus handle should be pressed tightly, and the surface of the tympanic membrane should be filled with gelatin sponge evenly to ensure that the graft and malleus handle are in close proximity. If the aforementioned points are considered, the risks of sensorineural hearing loss, tympanic membrane lateralization, and no connections between the tympanic membrane and malleus handle could be reduced. 23
Study limitations
First, this was a retrospective cohort analysis. Moreover, missing data were unavoidable, which may have affected the results. Second, the statistical results may have been biased owing to the small sample size. Third, most of our cases were followed up for ≥3 years. However, the follow-up time of the patients in 2020 was not long, which may have influenced long-term complications such as re-perforation. Further prospective studies with larger sample sizes and longer follow-up periods are needed to confirm these results.
Conclusions
In this study, the success rate of over-under tympanoplasty was higher than that of medial tympanoplasty, especially in near-total or total perforations of the tympanic membrane. Over-under tympanoplasty is preferable for large perforations. The risks of sensorineural hearing loss, tympanic membrane lateralization, and no connections between the tympanic membrane and malleus handle are very low with this technique.
Footnotes
Author contributions
Xiaowen Zhang: Study design; data acquisition; chart abstraction; data analysis/interpretation, and manuscript drafting
Caili Ji: Chart abstraction; data analysis/interpretation; and manuscript revision
Aifeng Li: data acquisition and manuscript revision
Zhenju Xu: data acquisition and manuscript revision
Xiaoheng Zhang: Study concept and design; data analysis/interpretation; and manuscript revision
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.