
Abstract

Significance Statement
The orbital apex cell is a useful landmark that can serve as a guide to the sphenoid sinus during endoscopic sinus surgery. Surgeons can navigate infero-medially from the orbital apex cell to locate the os of the sphenoid sinus. Proper orientation in and around the sphenoid sinus is essential for minimizing operative morbidity and maximizing patient safety.
Rhinology Clinic
Navigation to the sphenoid sinus is a critical aspect of many procedures such as functional endoscopic sinus surgery or trans-sphenoidal approaches to the skull base. Surgical approaches to the sphenoid bring the surgeon in close proximity to vital structures such as the internal carotid artery (ICA), optic nerve, orbit, and skull base. Reliable surgical landmarks can help minimize risk of injury to these structures intraoperatively.
The authors present the posterior-superior-most ethmoid air cell, herein the Orbital Apex Cell (OAC), as a consistent and useful landmark for endoscopic approaches to the sphenoid sinus. Deliberate identification of the OAC facilitates safe dissection into the sphenoid sinus and helps serve as a reminder of structures at risk of injury if the surgeon’s position within the skull base is not properly identified.
The orbital apex refers to the posterior aspect of the orbit which contains the superior orbital fissure, optic canal, and inferior orbital fissure and serves as a conduit for many neurovascular structures to pass from the intracranial to extracranial compartments. The ethmoid sinuses are located medial to the orbital apices, bilaterally. The OAC is so named based on its close proximity in the anteromedial direction to the true orbital apex. Furthermore, this naming convention is particularly useful when educating trainees by highlighting structures at risk for injury should a mis-interpretation of the local anatomy occur.
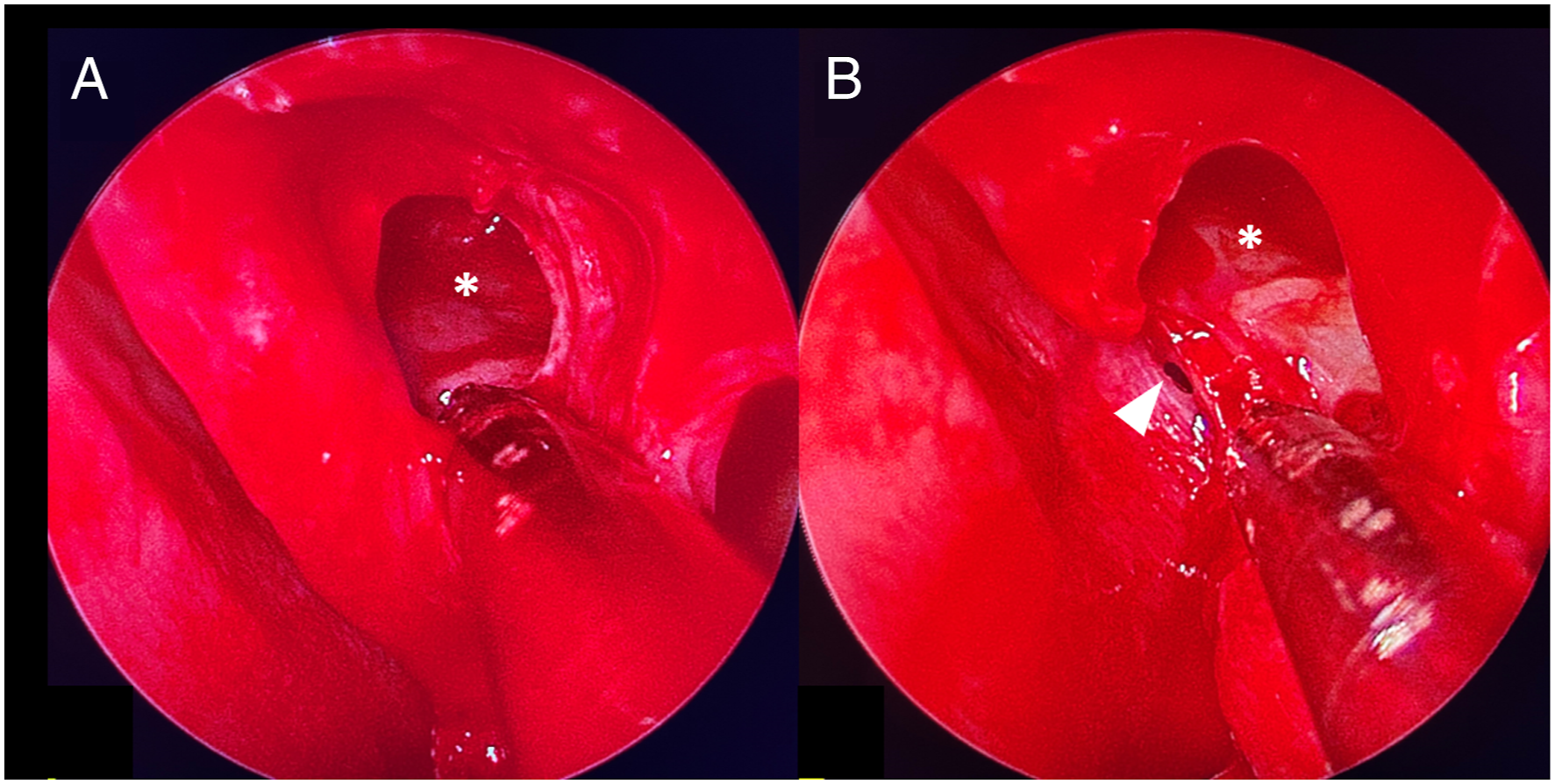
In the authors’ experience, the orbital apex cell is consistently located anterior to the face of the sphenoid sinus (Figure 1, Supplementary Video 1). The borders of the orbital apex cell are comprised of the lamina papyracea laterally, fovea ethmoidalis superiorly, and sphenoid face posteriorly. Variation occurs in the medial and inferior aspects of the cell depending on the ethmoid air cell anatomy, although the most common medial border is the superior turbinate (Figure 2). If only one posterior ethmoid cell is present, then the orbital apex cell comprises the entire space distal to the basal lamella to the sphenoid sinus. Identification of this cell can protect the surgeon by orienting them to the face of the sphenoid prior to posterior dissection. Once the OAC is identified, the surgeon can proceed infero-medially to find the natural os of the sphenoid sinus (Supplementary Video 1). This relationship is typically maintained in cases of variant anatomy such as prior surgery. Intraoperative (A) and CT images (B; axial, C; coronal, D; sagittal) demonstrating typical sinus anatomy of a patient undergoing trans-sphenoidal tumor resection. Asterisks (*) mark orbital apex cell, white arrow heads mark sphenoid sinus. Intraoperative images of the orbital apex cell prior to opening of the sphenoid sinus before (A) and after (B) removing a portion of the superior turbinate. Asterisks (*) mark orbital apex cell, white arrow head marks the sphenoid os, located infero-medially to the orbital apex cell.
In some individuals, the OAC has pneumatized posteriorly and superiorly to the sphenoid sinus, an anatomic variant known as an Onodi cell (Figure 3). Failure to recognize the Onodi cell can place critical structures such as the optic nerve, ICA, and skull base at risk of injury. In such cases, the surgeon first identifies the posterior ethmoid air cells and the OAC using a combination of stealth navigation and endoscopic visualization. The posterior ethmoids are then opened and the location of orbital apex cell posterior wall is noted. The surgeon can visualize its inferior border of the Onodi cell and the depth to which it extends into the sphenoid sinus and proceed infero-medially to the sphenoid os. Deliberate and consistent identification of the OAC prior to entry into the sphenoid allows the surgeon to recognize when an Onodi cell is present and avoid misorientation when dissecting across the face of the sphenoid. Sagittal (A) and coronal (B) CT images demonstrating an Onodi cell present superior to the sphenoid sinus. Asterisks (*) mark Onodi cell, white arrow heads mark the sphenoid sinus.
The clinical utility of structures near the orbital apex have been described previously in the “Canary Island Sign,” named for the location where three colors of bone observed in the orbit come together. 1 Recognition of the OAC and Canary Island Sign together offer an excellent opportunity for proper orientation during endoscopic sinus surgery and minimize risk of intraoperative injury.
Limitations of landmarks used for endoscopic surgical navigation include natural variation in local anatomy. For example, the superior turbinate has been described as a marker of the sphenoid os, but the distance between these structures vary widely across patients. 2 Other landmarks such as the supreme nasal turbinate 3 or approximate distances between the choana and skull base 4 have been proposed, but require more intraoperative approximation and may be less useful in cases of variant anatomy. In regard to the orbital apex cell, surgeons can locate the sphenoid os by moving infero-medially without the need to approximate distances or rely on landmarks such as the middle or superior turbinate, which may have been altered in prior surgeries.
In summary, the OAC is a consistent landmark for sphenoid sinus os identification even in cases of variant anatomy. The orbital apex cell is particularly useful for training residents in safely navigating to the sphenoid sinus and helps minimize the risk of injury to surrounding structures.
Supplemental Material
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.