
Abstract
We report a rare case of traumatic stapes luxation into the vestibule. A 31-year-old female visited an emergency room with sudden onset of vertigo and conductive hearing loss after accidental penetrating injury to the right ear. Temporal bone computed tomography detected pneumolabyrinth, with a shade of whole intact stapes in the vestibule. Under exploratory tympanotomy, we observed a separated incudostapedial joint, and the stapes was depressed into the vestibule. The stapes was pulled out to the middle ear, and stapedectomy was performed; the crus were cut, the suprastructure was removed, and the fractured footplate and the long process of the incus were connected with a piston wire. The stapes footplate was sealed with soft tissue and surgical glue. Vertigo rapidly subsided after surgery, and hearing was improved to normal range. However, hearing loss at high frequencies was not recovered, probably because of inner ear damage due to the stapes depressed into the vestibule or surgical manipulation within the vestibule. Traumatic ossicular dislocation is not an uncommon occurrence in otolaryngologic practice, but stapes luxation is rare. Here, we report a rare case with successful repair. This report could serve as a basis for proper treatment in similar cases in the future.
Introduction
Traumatic ossicular injuries occur mainly after head trauma, but direct ossicle injury through a penetrating injury is very rare. Direct and indirect injuries affect the ossicle in different ways. The most common form of indirect ossicular injury is dislocation of the incudostapedial joint (25%), followed by incus fracture (15%). 1 The incus is the most affected structure in this form of injury, in which all three ossicles simultaneously receive the same vector of force, but the malleus and stapes are protected by their tight anchorage to the surrounding structures. In particular, the stapes is the least involved structure in indirect ossicular injury because it is firmly attached to the oval window (OW) through the annular ligament and is located deep inside the tympanic cavity.1,2 On the contrary, although it is not possible to analyze the frequency and type of ossicular injury significantly due to the rarity, but few cases of stapes injury due to penetrating injury have been reported. Considering the angle from the external ear auditory canal (EAC) to the tympanic membrane, a foreign object entering the EAC could impact the stapes regardless of its depth.
This case is a report of stapes luxation into the vestibule due to penetrating ear injury. In this rare case, stapes luxation was confirmed by imaging, and hearing was successfully restored. This report will serve as a basis for proper treatment in similar cases in the future.
Case report
A 31-year-old woman presented with acute onset vertigo and right-sided unilateral hearing loss after accidental penetrating injury to the right ear. On physical examination, a small perforation with an irregular margin was found on the posterior aspect of the right tympanic membrane (TM). With Frenzel goggles, grade III horizontal spontaneous leftward nystagmus was noted, and the amplitude of the nystagmus increased when the gaze was directed to the left in accordance with Alexander’s law. Gaze-evoked nystagmus was absent. Corrective saccade was noted after rightward head rotation during the bedside head-impulse test. The patient was unable to perform the positional test, head-shaking test, and gait test due to severe vertigo. The fistula test was performed by pressing on the ipsilateral EAC, but no nystagmus was noted. Pure-tone audiometry revealed conductive hearing loss of the affected ear, with an air-conduction threshold of 49 dB HL and bone-conduction (BC) threshold of 16 dB HL (Figure 1A). Temporal bone computed tomography (TBCT) demonstrated a separated incudostapedial (IS) joint, and the stapes and air bubbles were identified within the vestibule (Figure 1B and 1C). Traumatic ossicular disruption, stapes luxation into the vestibule, and perilymphatic fistula (PLF) were suspected and exploratory tympanotomy was planned. Preoperative finding of the patient. Preoperative audiogram (A). Temporal bone computed tomography demonstrates the shadow of the stapes within the vestibule (B, arrow). Air bubbles are seen in the vestibule and are an indicator of perilymphatic fistula (C, arrow head).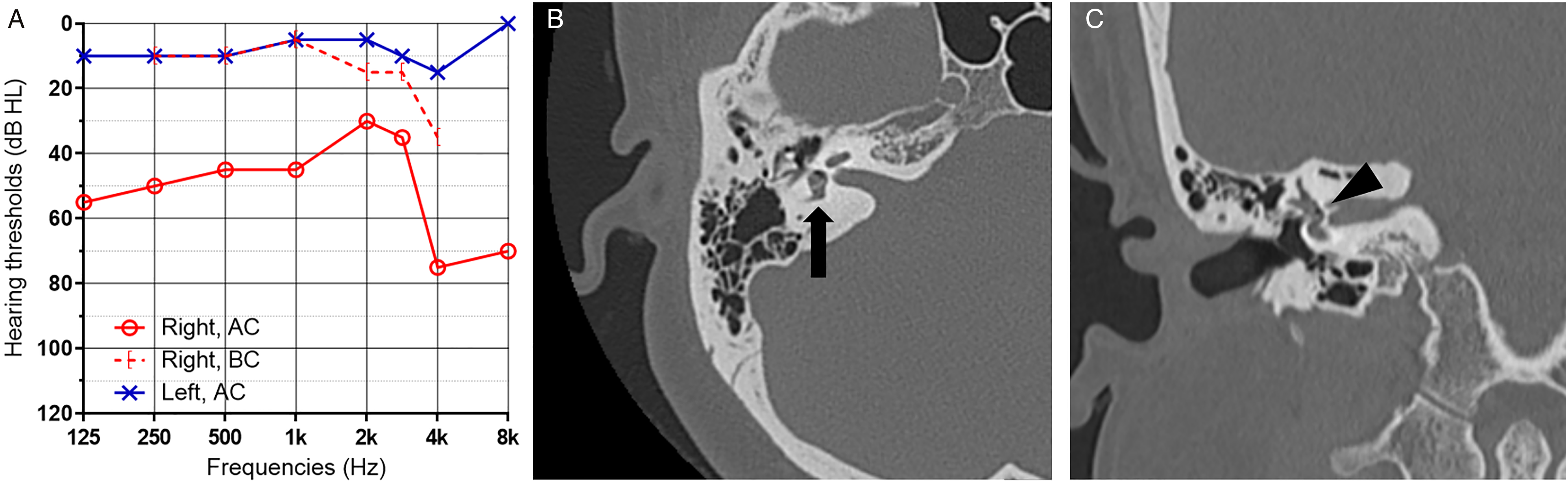
An ear endoscope was utilized for exploration, and a tympanomeatal flap was elevated. The malleus and incus were intact in shape and stability, but the IS joint was dislocated. The separated stapes was deeply depressed into the vestibule so that only the capitulum was visible from the 0° endoscopic view (Figure 2A). The depressed stapes was carefully pulled out to the middle ear using a pick, with care not to damage the vestibule. However, the stapes repeatedly sank back into the vestibule and was unable to maintain its original position (Figure 2B). Therefore, stapes surgery was planned instead of reconstruction of the ossicular chain. Both anterior and posterior crura were cut using crurectomy scissors, and the suprastructure of the stapes was removed. During this process, the footplate was fractured unintentionally, and a piston wire was used to connect the fractured stapes footplate and the long process of the incus (Figure 2C). Soft tissue and surgical glue were applied for better sealing. The TM perforation was closed with tragal perichondrium in the underlay technique. Intraoperative still images from 0° endoscopic view. The separated stapes was depressed into the vestibule such that only the capitulum was visible (A). The pulled-out stapes repeatedly sank into the vestibule (B). A piston wire connected the long process of the incus and the fractured stapes footplate (C). Postoperative 3-month audiogram shows normal hearing except at high frequencies (D). *; stapes.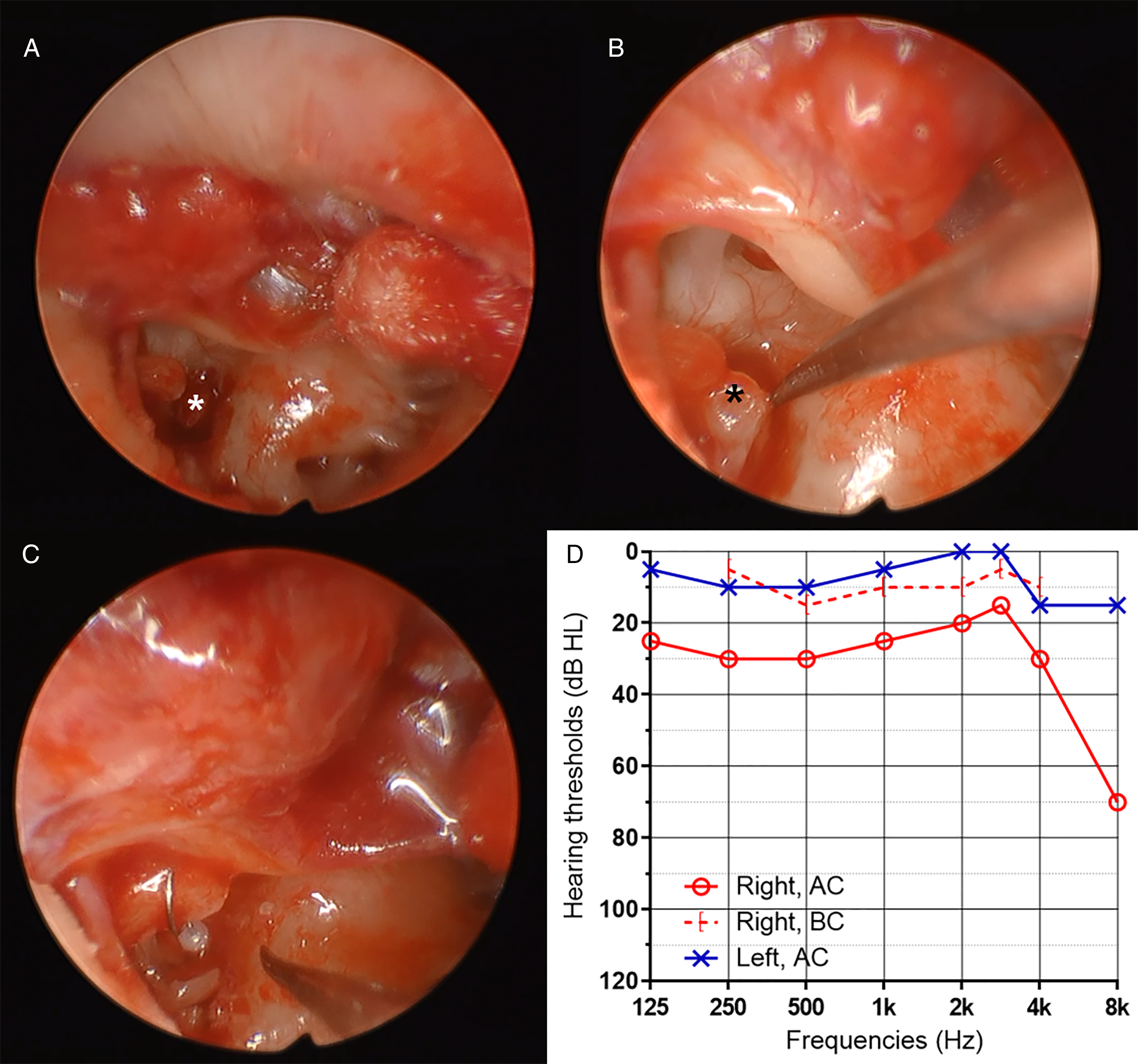
Vertigo rapidly subsided after surgery, and the patient was discharged without complication. Corticosteroid was administered orally for 10 days. Three months postoperatively, pure-tone audiogram revealed normal hearing with an air-conduction threshold of 26 dB HL and BC threshold of 11 dB HL compared to 8 dB HL on the contralateral side (Figure 2D). However, hearing loss was sustained at frequencies higher than 4,000 Hz. Repeat TBCT showed complete resolution of pneumolabyrinth.
Discussion
This is a very rare case report of stapes luxation into the vestibule due to a penetrating injury. Due to its rarity, there is no established treatment protocol for stapediovestibular luxation. While most of the reported cases were surgically treated, some received conservative treatment.3,4 Various factors can be involved in determining treatment options, such as patient willingness and severity of the injury or symptoms; however, the biggest difference between the surgery and conservative treatment groups was whether or not vertigo persisted. In the patients who received conservative treatment, vertigo spontaneously resolved within 1 week, and no additional surgical treatment was performed to restore hearing, most of which recovered from severe to mild loss. When stapediovestibular luxation occurs, the OW that separates the middle ear and the inner ear opens, and PLF develops. There have been some reports of PLF recovering spontaneously with conservative care, but if the fistula remains open with continuous perilymph leakage, vertigo and gradual hearing loss will persist. However, there is no way to predict whether the fistula will recover spontaneously. While some studies suggest that patients with pneumolabyrinth had a linear correlation between symptoms and air volume in the inner ear on CT images,5,6 others showed no such relationship. 7 Furthermore, stapes luxation and pneumolabyrinth might be overlooked in CT images.8,9 When vertigo occurs after penetrating injury, it can be inferred that the stapes is separated from the OW. In such cases, it would be advantageous to perform surgical treatment as soon as possible.
There are two purposes of surgical treatment of stapediovestibular luxation. The first is vertigo control, and the second is restoration of hearing. Of these, vertigo is resolved in more than 95% of cases by repairing the PLF, 10 for which the surgical procedures and technique have been well established and reported. Every reported stapediovestibular luxation case achieved complete vertigo relief after surgical PLF repair. 11 On the contrary, hearing results varied highly. There are two mechanisms for hearing loss in stapediovestibular luxation. One is sensorineural hearing loss (SNHL) caused by inner ear damage due to stapes luxation into the vestibule and/or leakage of perilymph, and the other is conductive hearing loss caused by disruption of the ossicular chain. For resolution of SNHL, timely surgical repair of PLF and application of corticosteroids are essential. Most studies agree that the time window to PLF repair is one of the most important factors in resolution of SNHL. According to Tsubota, who analyzed 24 cases of pneumolabyrinth, there are three factors that affect hearing recovery. 12 The first is the time window to PLF surgery, the second is the initial BC thresholds, and the last is the presence of stapes lesions, possibly suggesting the size of the PLF and the amount of damage to the inner ear. Among these three factors, surgical timing is the one under clinician control. Thus, when PLF is suspected, the clinicians should not hesitate to perform early surgical treatment. In addition, the luxated stapes must be considered. Some studies argue that removal of the stapes is not necessary since the process can produce additional damage or scarring that could cause late damage. 13 On the contrary, it was argued that stapes in the vestibule must be repaired since it can cause vestibular space obstruction and eventually develop inner ear dysfunction. 14 However, there is insufficient evidence to support these two claims. Hatano et al. sealed the OW while leaving the stapes in the vestibule, but the BC thresholds improved more than 30 dB compared to pre-operation, showing only a difference of 10 dB from the unaffected side. 15 In this case, a large amount of perilymph leakage was suspected because the stapes had completely luxated into the vestibule. With immediate surgical treatment, additional perilymph leakage was minimized. Care was taken during surgery to use suction as little as possible, the stapes was gently pulled out, and systemic corticosteroids were administered. These strategies helped to well restore the BC level.
Previous studies used one of several methods to reconstruct the ossicular chain with an intact stapes depressed into the vestibule. The most common method is to rescue the stapes, seal the OW with fascia, and place the stapes or other materials such as cartilage on the fascia to reconstruct the ossicular chain.11-13,16 The air-bone gap decreased in only one of the four cases. There were two cases where the stapes was repositioned without placing fascia between the OW and the stapes,17,18 and hearing gain was achieved in only one case. Another case performed stapedectomy but did not show improved hearing. 19 Due to the rarity and inconsistent hearing results of such an injury, it is difficult to determine the optimal method. In principle, reconstruction should be performed in such a way that vibrations can be effectively transmitted to the OW, while ensuring stapes stability and no leakage. There is a report of a case where stapes luxation progressed slowly over 2 years after cartilage tympanoplasty and produced delayed symptoms, 9 indicating the need for caution in reconstruction. In our case, to minimize the possibility of the separated stapes falling back into the vestibule, stapedectomy was performed rather than ossicular chain reconstruction. No material was positioned between the stapes footplate and OW so as to not interfere with transmission of the vibration. Instead, soft tissue and surgical glue were applied to protect the vestibule. This technique led to successful reduction of air-bone gap and vertigo relief.
This case reports a successful recovery of vertigo and hearing loss through early surgical treatment of stapes luxation into the vestibule after penetrating injury. The most important factor for successful recovery is early PLF repair with careful procedures. This report will serve as a basis for proper treatment of similar cases in the future.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (No. 2020R1C1C1005965) to H.J.L.
Ethical approval
This study was approved by the Institutional Review Board of the authors’ institute (IRB number: OC22ZASI0050), and the requirement for informed consent from the patient was waived. A patient’s anonymity is preserved in the manuscript.
Data availability
The data used to support the findings of the study are included whtinin the article.