
Abstract
The purpose of this study was to investigate whether the use of hyaluronic acid/collagen resorbable gel (Regenwel®) has an inhibitory effect on rhinostomy obstruction during endoscopic dacryocystorhinostomy (Endo DCR). A total of 298 patients diagnosed with unilateral primary acquired nasolacrimal duct obstruction from May 2017 to June 2021 who underwent Endo DCR were enrolled. The patients were divided into the Regenwel group (152 patients) and the Control group (146 patients) that did not use Regenwel during surgery, and the medical records were compared and analyzed retrospectively. The mean age of the Regenwel group was 65.8 years, and that of the Control group was 63.2 years. Regarding anatomical success as the primary outcome, the Regenwel group had a higher success rate than the Control group (96.7% vs 86.3%, P = .012), and the functional success result confirmed that the Regenwel group had a higher success rate than the Control group (94.1% vs 84.3%, P = .024). Among secondary outcomes, granulation formation occurred less frequently in the Regenwel group than in the Control group (9.2% vs 32.2%, P < .001), and there was no statistically significant difference in postoperative bleeding between the 2 groups (0% vs 1.4%, P = .478). The Regenwel group had fewer infections after surgery than the Control group (5.3% vs 8.9%, P = .012) and required less frequent revision surgery (2.0% vs 15.8%, P < .001). In conclusion, Regenwel is a resorbable gel containing hyaluronic acid and collagen that is used during Endo DCR and is thought to contribute to the improvement of surgical success rate by preventing complications such as rhinostomy obstruction and bleeding after surgery.
Introduction
Endoscopic dacryocystorhinostomy (Endo DCR) is a surgical method first reported by McDonogh and Meiring in 1989 1 and is a standard procedure for treating primary acquired nasolacrimal duct obstruction. 2 The success rate of Endo DCR ranges from 54% to 96%. 3 Factors that determine the success of the surgery include size and location of rhinostomy and obstruction due to granulation tissue in rhinostomy after surgery. 4 In particular, various methods have been discussed to prevent rhinostomy obstruction, such as using topical mitomycin C or suturing of the mucosal flaps.5-12
Hyaluronic acid is a glycosaminoglycan composed of disaccharide units of glucuronic acid and N-acetylglucosamine and is the backbone of proteoglycan complexes connected by protein linkages. It is also a component of connective tissue and vitreous humor. 13
Studies have shown the effects of hyaluronic acid in the ophthalmic area for anti-adhesion, especially in strabismus surgery.14,15 In sinus surgeries, one study achieved remucosalization and minimized bleeding using hyaluronic acid hydrogel. 16 Another study using hyaluronic acid to prevent adhesion in the field of obstetrics and gynecology.17,18
In addition, a recent study announced that an implant containing collagen as the main component was used for External DCR to prevent the occurrence of fibrosis after surgery. 19 However, the effect of the combination of hyaluronic acid and collagen in Endo DCR has not been analyzed.
Therefore, in this study, we analyzed whether hyaluronic acid/collagen resorbable gel (Regenwel®; Genewel, Seongnam-si, Gyunggi-do, South Korea) was effective in reducing rhinostomy obstruction during surgery in a patient diagnosed with primary acquired nasolacrimal duct obstruction who underwent Endo DCR. In addition, its clinical application was evaluated.
Patients and Methods
From May 2017 to June 2021, we retrospectively reviewed patients aged 18 years or older who were diagnosed with unilateral primary acquired nasolacrimal duct obstruction at Korea University Guro Hospital and who underwent Endo DCR. In all patients, a general ophthalmic examination including fluorescein dye disappearance test (FDDT), probing, and syringing was performed to identify the cause of epiphora. If a clear cause was not found in the overall ophthalmic examination, dacryoscintigraphy was performed to evaluate the nasolacrimal duct. Only patients diagnosed with unilateral primary acquired nasolacrimal duct obstruction through this series of diagnostic procedures were enrolled, and the following were exclusion criteria. 1. Diseases of the cornea or conjunctiva. 2. Problems with punctum or canaliculus. 3. Previous nasolacrimal intervention or surgical history. 4. History of nasal cavity disease or surgical history. 5. Less than 18 years of age. 6. Follow-up period less than 3 months.
All surgeries were performed by one surgeon (S.B.) and were divided into Group A that used Regenwel® in the ostium during surgery and Group B (Control) that did not use it for comparison and analysis.
The surgery was performed under general anesthesia. A mixture of 2 mL of 2% lidocaine and epinephrine was injected into the nasal wall after bosmine gauze was packed into the nasal cavity. An incision was made in the lateral nasal mucosa under visualization with 0° 4-mm endonasal endoscopy (Endoscopic Equipment System, STRYKER, Kalamazoo, MI, USA). Using a 45°-angled 2mm-bite Kerrison punch (CareFusion, San Diego, CA, USA), osteotomies (8 mm x 10 mm in size) were created. The lacrimal sac was tented using a lacrimal probe, and then a posterior lacrimal sac flap was made using a sickle knife. The lateral flap was flattened on the nasal mucosal wall and the medial flap was removed. After a bicanaliculus (Bika, FCI Ophthalmics, Pembroke, UK) was inserted through the upper and lower canaliculi, Regenwel® was injected around the rhinostomy site in group A (Figure 1), In contrast, nothing was inserted in group B. Nasal endoscopic findings in the group A. (A) After inserting a silicone tube, Regenwel® was injected. (B) Intact rhinostomy at 3 months postoperatively.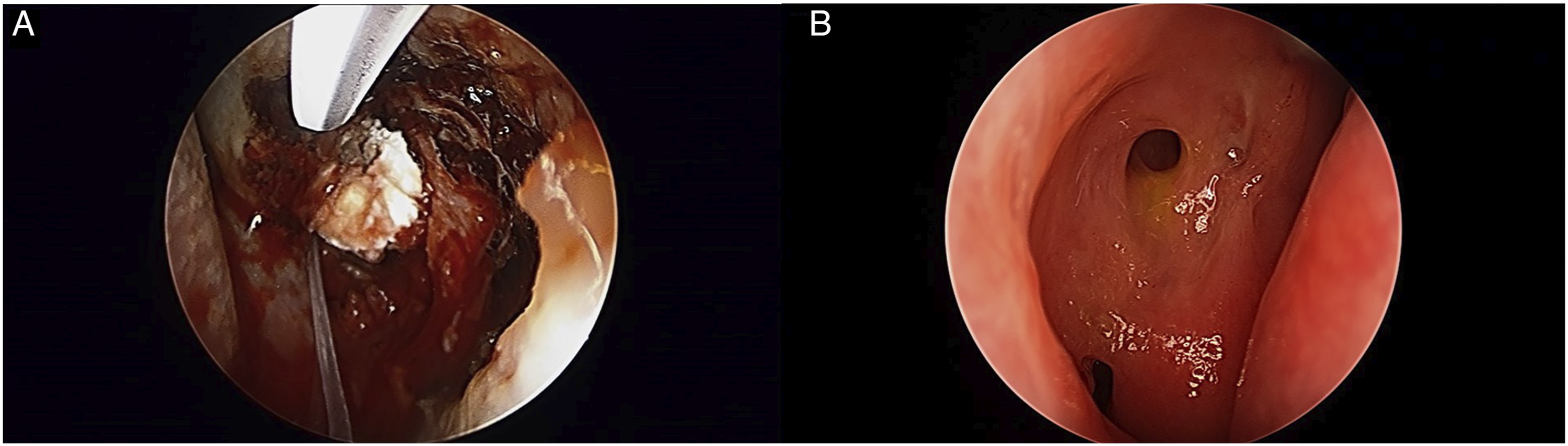
All patients were hospitalized for 3 days, received systemic antibiotics during and after surgery, and were discharged on the day after surgery. After surgery, antibiotic eye drops (Tarivid solution; Santen Pharmaceutical Co, Ltd, Osaka, Japan) and steroid eye drops (Lotemax ophthalmic solution .5%; Bausch & Lomb, North Bridgewater, NJ, USA) were each instilled 4 times a day for 3 months, and the patients were instructed to wash the nose with steroid nasal spray (Nasonex Nasal Spray; Schering-Plough Corp, Kenilworth, NJ, USA).
All patients reported to the outpatient clinic at 1, 3, 8, and 12 weeks postoperatively for follow-up. We evaluated the position of the inserted tube, FDDT, rhinostomy obstruction, and munk score. The inserted bika tube was removed 2 months after surgery. Postoperative bleeding or infection or rhinostomy obstruction due to granulation observed within 1 to 2 mm of the rhinostomy site during follow-up was recorded with photographs and charts (Figure 2). Complications at 3 months after surgery. (A) Postoperative bleeding from a petechiae-like vascular focus. (B) Postoperative infection. (C) Granuloma on rhinostomy site.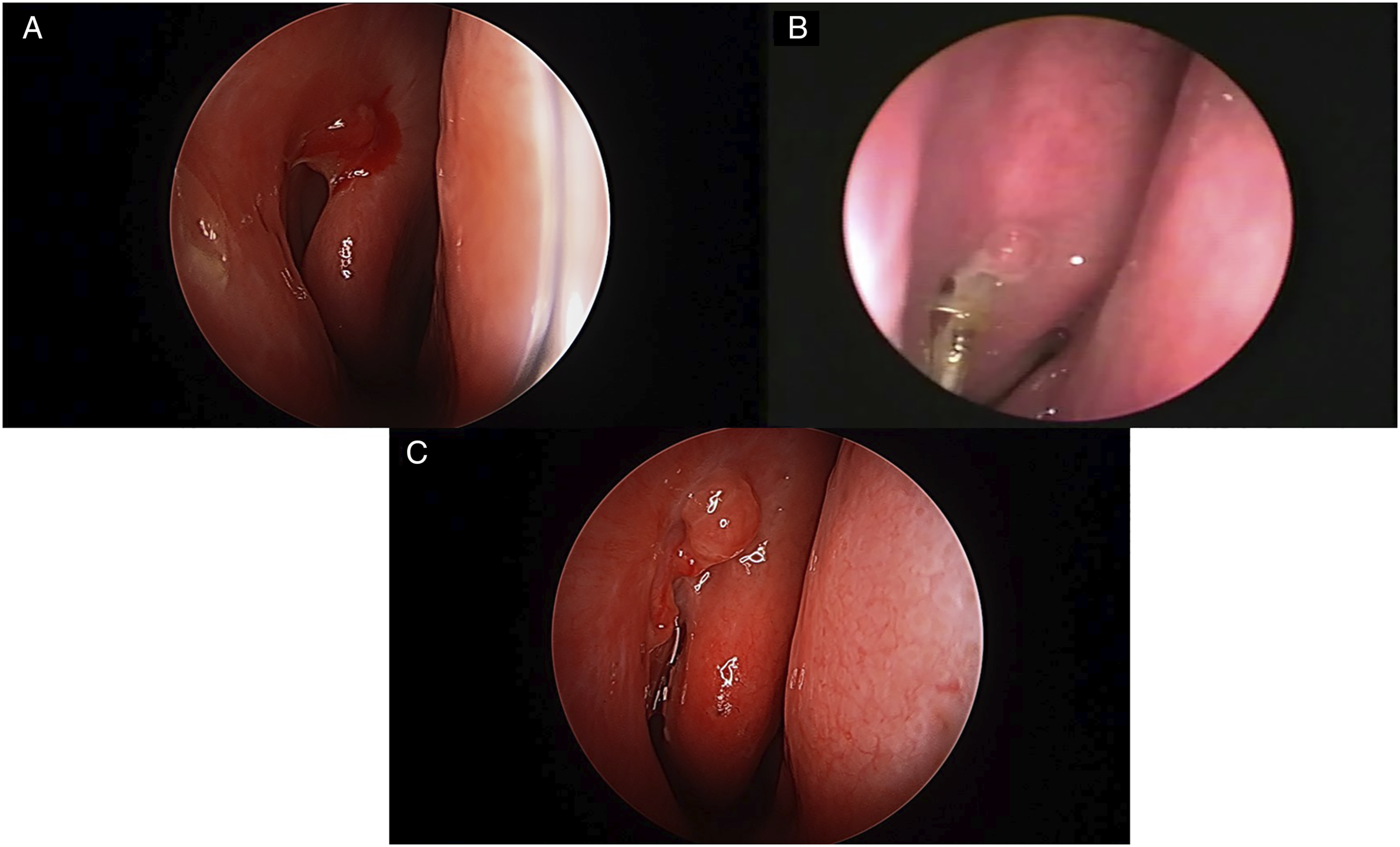
Postoperative outcomes were evaluated as primary outcomes and secondary outcomes. Primary outcomes were evaluated 3 months after surgery and were divided into anatomical success and functional success. Anatomical success was defined as passage without regurgitation as a result of syringing. Functional success was defined as a munk score of 1 or less. Secondary outcomes were postoperative granulation, bleeding, infection, and revision surgery. Based on these primary and secondary outcomes, the results of the group A and the group B were compared.
All statistical analysis was performed with SPSS ver. 22.0 (SPSS Inc., Chicago, IL, USA), and we used the Pearson’s chi-square test. A P-value less than .05 was considered statistically significant.
The study was approved by the Institutional Review Board of Korea University Hospital.
Results
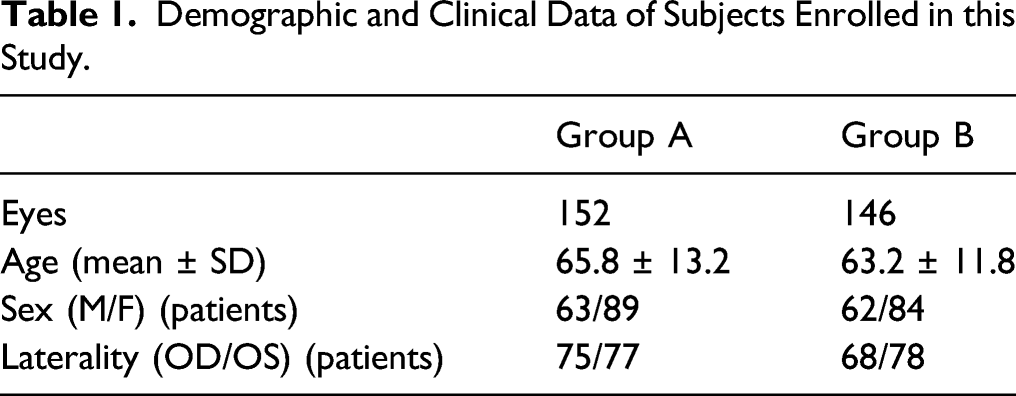
Demographic and Clinical Data of Subjects Enrolled in this Study.
Primary Outcomes Results.

aPearson’s chi-square test was used.
P-values less than .05 were considered statistically significant.
Secondary Outcomes Results.
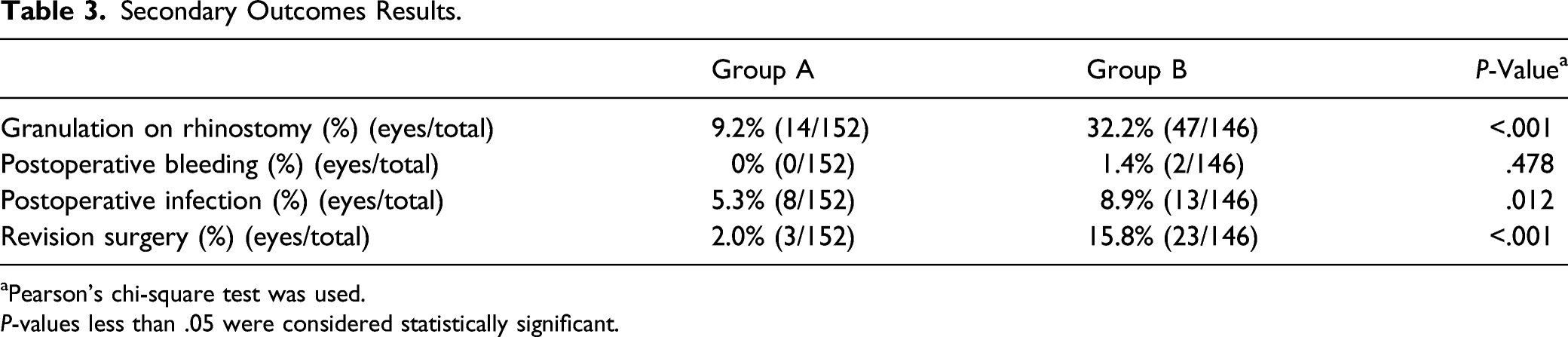
aPearson’s chi-square test was used.
P-values less than .05 were considered statistically significant.
Discussion
Endo dacryocystorhinostomy is a surgical method that has the advantages of low intraoperative bleeding, short hospitalization period, and low scar formation6,20 and is used widely as a treatment for primary nasolacrimal duct obstruction. The main cause of failure of Endo DCR is closure of the rhinostomy opening,20-22 most often caused by excessive scars/synechia or granulation formation at the ostium.20,21 Although some surgeons used mitomycin C to reduce fibrosis formation,8,9 there is a report of granulation tissue generation after using mitomycin C,23,24 so the effect of its use is unclear.
Therefore, in this study, as a method to prevent the failure of Endo DCR, it was studied whether packing a hyaluronic acid and collagen mixture was effective, and it was found that there was a positive effect.
Another study reported the effect of packing resorbable materials, mostly hyaluronic acid, into the nose to prevent granulation after Endo DCR. 25 Hyaluronic acid is a polysaccharide component of the extracellular matrix used for nasal hemostasis and to reduce scar formation and promote wound healing in sinus surgery.26-29
There is a report of sodium hyaluronate use during Endo DCR to reduce granulation after surgery and to improve the success rate of surgery. 30 Another study used self-cross-linked hyaluronic acid hydrogel during Endo DCR to promote mucosal epithelial healing and prevent granulation. 31
Although hyaluronic acid appears to contribute to the prevention of rhinostomy obstruction after Endo DCR, it has been reported that the mixed solution of sodium hyaluronate and sodium carboxymethylcellulose (HACMC) has no biologic influence on adhesions or fibroblasts during wound healing. 13 Kwon et al. 32 reported that a mixed solution of sodium hyaluronate and sodium carboxymethylcellulose in a rabbit model contributed to prevention of tissue adhesion and fibrosis rather than affecting the inflammation process. Summarizing the results of these studies, hyaluronic acid seems to prevent granulation by acting as a physical barrier rather than a biologic influence in wound healing after Endo DCR.
Another major component of the resorbable gel in this study was collagen. Collagen, an extracellular matrix protein, is biocompatible and has biodegradability and osteoinduction.33,34 The triple helix structure of collagen imparts stiffness, providing a natural support base for cell adhesion.35,36 Collagen also promotes cell proliferation, differentiation, and migration. In addition, collagen is a main component formed during wound healing; promotes coagulation, which helps in wound healing and hemostasis,37,38 and plays a role in reducing shrinkage and scarring and accelerating epithelialization. 39 Therefore, collagen is an important component in the controlled release of bioactive molecules related to wound healing. In addition, extracellular matrix-like hydrogel composed of collagen and hyaluronic acid had the ability to promote spontaneous wound healing and to form vessels and an epithelial layer. 40
Most existing studies have reported preventive effects against granulation or scarring after Endo DCR using hyaluronic acid or mixed solution of sodium hyaluronate and sodium carboxymethylcellulose. However, this study is significant in that it is the first study using resorbable gel containing hyaluronic acid and collagen in Endo DCR, this study showed good postoperative results using a resorbable gel containing hyaluronic acid and collagen, and the probability of rhinostomy obstruction and infection after surgery was significantly reduced. Although there was no significant difference in postoperative bleeding between the 2 groups, none occurred in the Regenwel group. Therefore, it was revealed that the role of hyaluronic acid as a physical barrier and the biologic effect of collagen were combined to suppress the occurrence of granulation and bleeding after Endo DCR.
The first limitation of this study is that it was retrospective. Second, the follow-up period was not long. Last, the results were not calculated by size of granulation. Therefore, further study is needed to provide a good method to prevent postoperative rhinostomy obstruction in Endo DCR.
In conclusion, Regenwel® is a resorbable gel containing hyaluronic acid and collagen as its main components. Applying this to the rhinostomy site during Endo DCR can suppress postoperative granulation and bleeding and prevent rhinostomy obstruction to have a positive effect on postoperative outcome.
Footnotes
Authors' contributions
Conception and design of the study (H.L. and S.B.)Conduct of study (H.L. and S.B.).Collection and management of data (H.L., S.Y., and S.B.).Data analysis and interpretation (H.L. and S.B.).Preparation, review, and approval of the manuscript (H.L., S.Y., and S.B.).S.B. contributed the manuscript as a corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
This study was approved by the institutional review board of Korea University Medical Center in Seoul, Korea. All data collection and analysis efforts were conducted in accordance with the tenets of the Declaration of Helsinki. All informed consents were obtained from the patients.
Consent for Publication
All written informed consents were obtained from the patients for the use of the patient's clinical photos and medical records.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.