
Abstract
Introduction
Papillary thyroid carcinoma (PTC) is the most common type of thyroid carcinoma, and an explosive rise in the frequency of diagnosing PTC has increased nearly 800% in the United States over the preceding 35 years. Nearly 50% of the increase was due to PTC of 1 cm or less in diameter, with 87% being smaller than 2 cm. This dramatic rise in mostly subclinical disease has been attributed largely to more frequent and widespread use of imaging of the head and neck for unrelated investigations, with the unanticipated discovery of these incidental cancers. 1 Nevertheless, thyroid cancer mortality remained flat, and the overall survival rate is excellent. However, PTC has a high rate of lymph node metastasis, even for microcarcinomas, defined as PTC of ≤1 cm.2-4 Studies have demonstrated that PTC patients with high-risk features such as male sex, larger tumor size, and extrathyroidal extension (ETE), in addition to the lower risk younger aged patients are at increased risk for lymph node metastasis.5,6 The pattern of spread of cervical lymph nodes in PTC typically follows a logical sequence from perithyroidal to deeper central compartment VI nodes, to lower (compartment IV) then eventually higher (compartments III and II) lateral jugular nodes, documented by prior studies.7,8 The intent of our study was to review the lymphadenectomy results of the central compartment in pN1a PTC patients, determine any associated influencing factors, and then quantify and identify any pattern that could provide a basis for future compartment VI surgical intervention.
Materials and Methods
Patients
The study comprised a retrospective review of 443 consecutive pN1a PTC patients treated at the Head and Neck Surgery, Fujian Cancer Hospital between May 2019 and January 2021. Inclusion criteria were as follows: 1) FNA biopsy confirmed stage T3-4 and high-risk (cN+, invasive) T1-2 PTC patients who underwent thyroidectomy combined with central neck dissection; and 2) pathology was PTC and stage pN1a. Excluded were patients with: 1) bilateral tumors and contralateral lobe dissemination; 2) evidence of lateral neck LNM or distant metastasis; and 3) any treatment history of thyroid-associated medication or prior thyroid surgery. Clinicopathologic features including gender, age at diagnosis, tumor location, tumor maximal diameter (TMD), multifocality, ETE, lymph node location, number of DLN, and number of MLN and MR (MLN/DLN) were collected.
Operation
To ensure the consistency of surgical strategies, the operations were performed by the same treatment group. In order to ensure the accuracy of pathological diagnosis, intraoperative frozen section was applied to all patients. Once malignancy of the thyroid nodule was confirmed; central neck dissection was performed on the side of malignancy. Central compartment refers to level VI. A consent to surgery was signed by patients and immediate family member before the operation.
Statistical Analysis
Descriptive statistics were presented as summarized data. Continuous variables were expressed as number (%) or
Results
The average age was (44.5 ± 11.5) years, and the mean TMD was (1.7 ± .99) cm. There were 275 left lobe PTCs and 168 in the right. The mean number of DLN, MLN, and MR were (6.9 ± 4.46), (3.1 ± 2.58), and (.5 ± .3), respectively. The incidence of postoperative hypoparathyroidism was low and transient because all patients underwent dissection limited to one side of the central compartment (4, .9%); 3 patients suffered temporary hoarseness that resolved within 3 months. Due to ETE or contralateral benign tumors with indications for surgery, 107 patients underwent total thyroidectomy and 61 were treated with radioactive I131 therapy. Patients were followed for 5–24 months postoperatively, and 5 were lost to follow-up, but none showed evidence of recurrence.
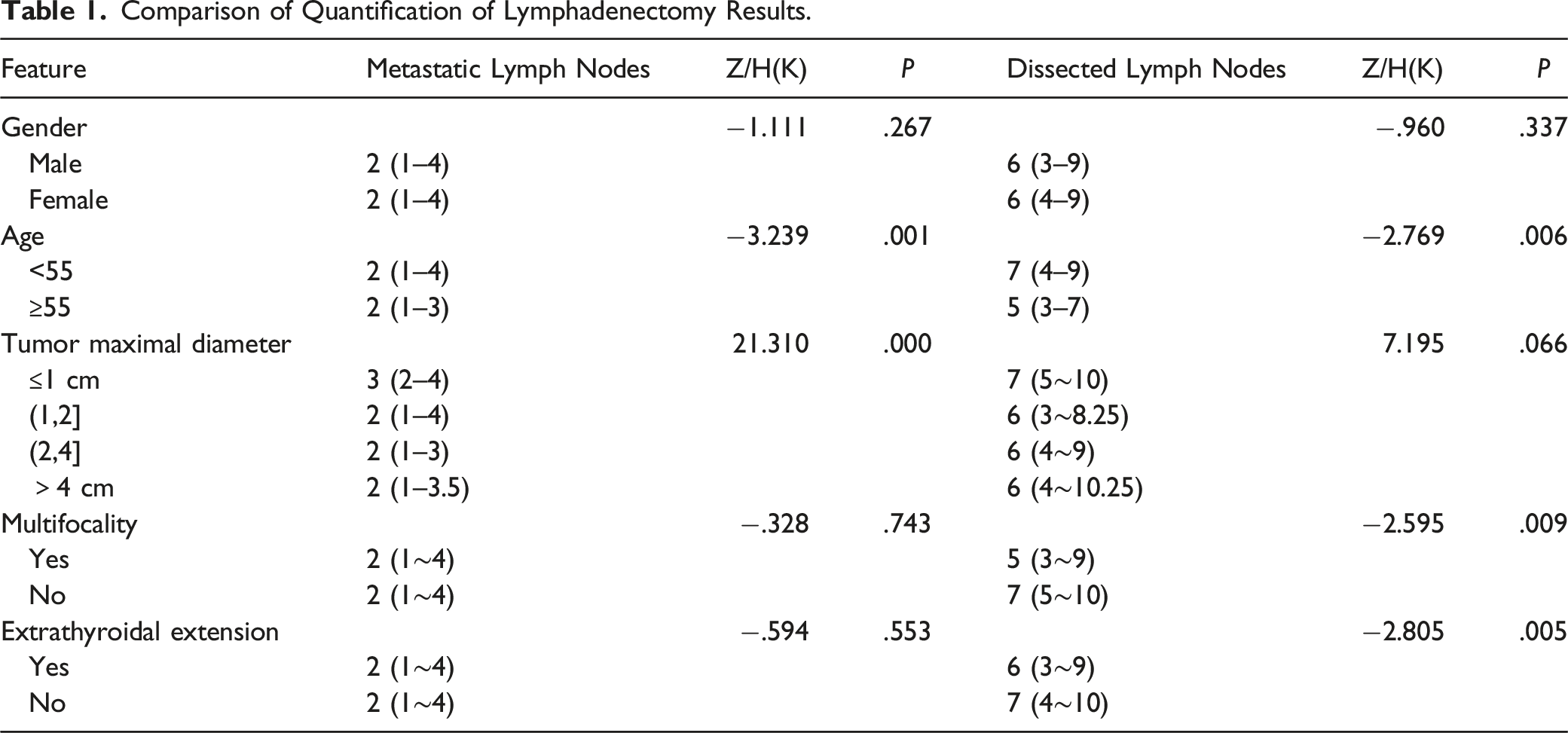
Comparison of Quantification of Lymphadenectomy Results.
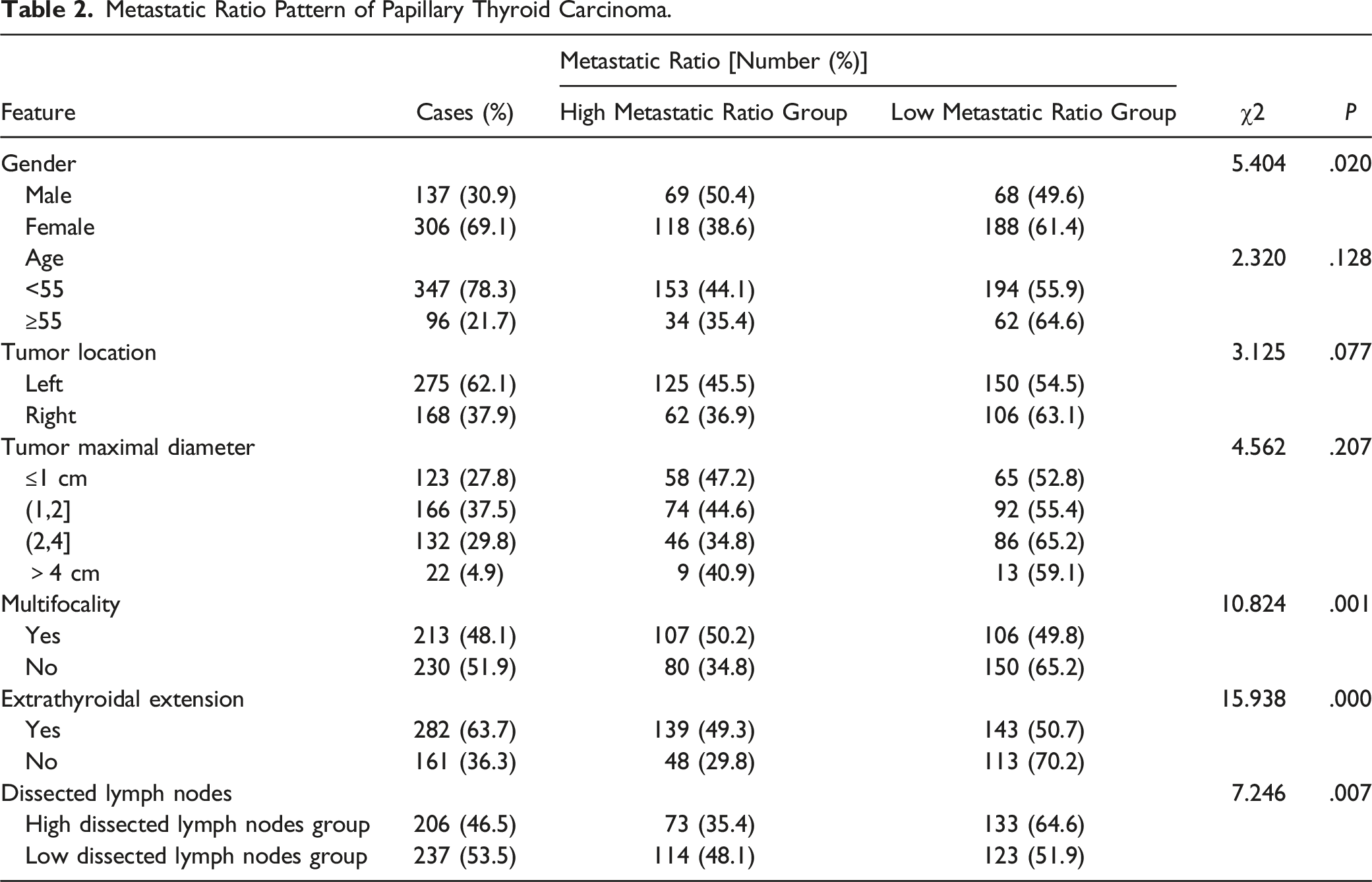
Metastatic Ratio Pattern of Papillary Thyroid Carcinoma.
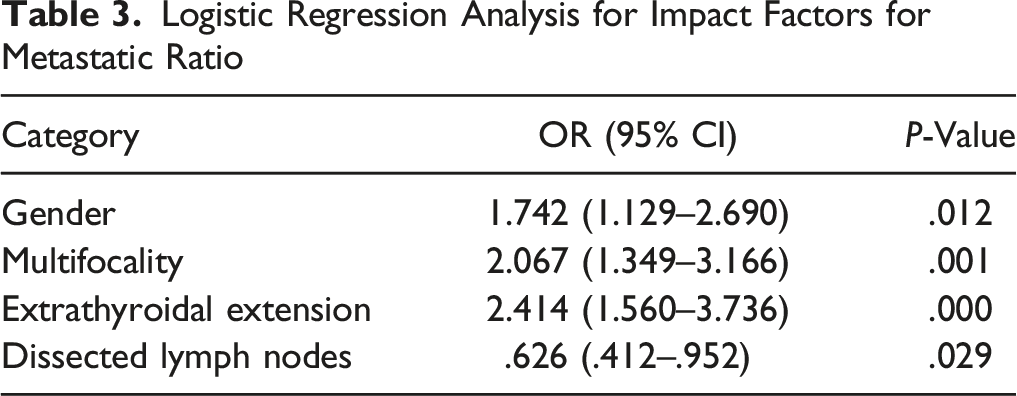
Logistic Regression Analysis for Impact Factors for Metastatic Ratio
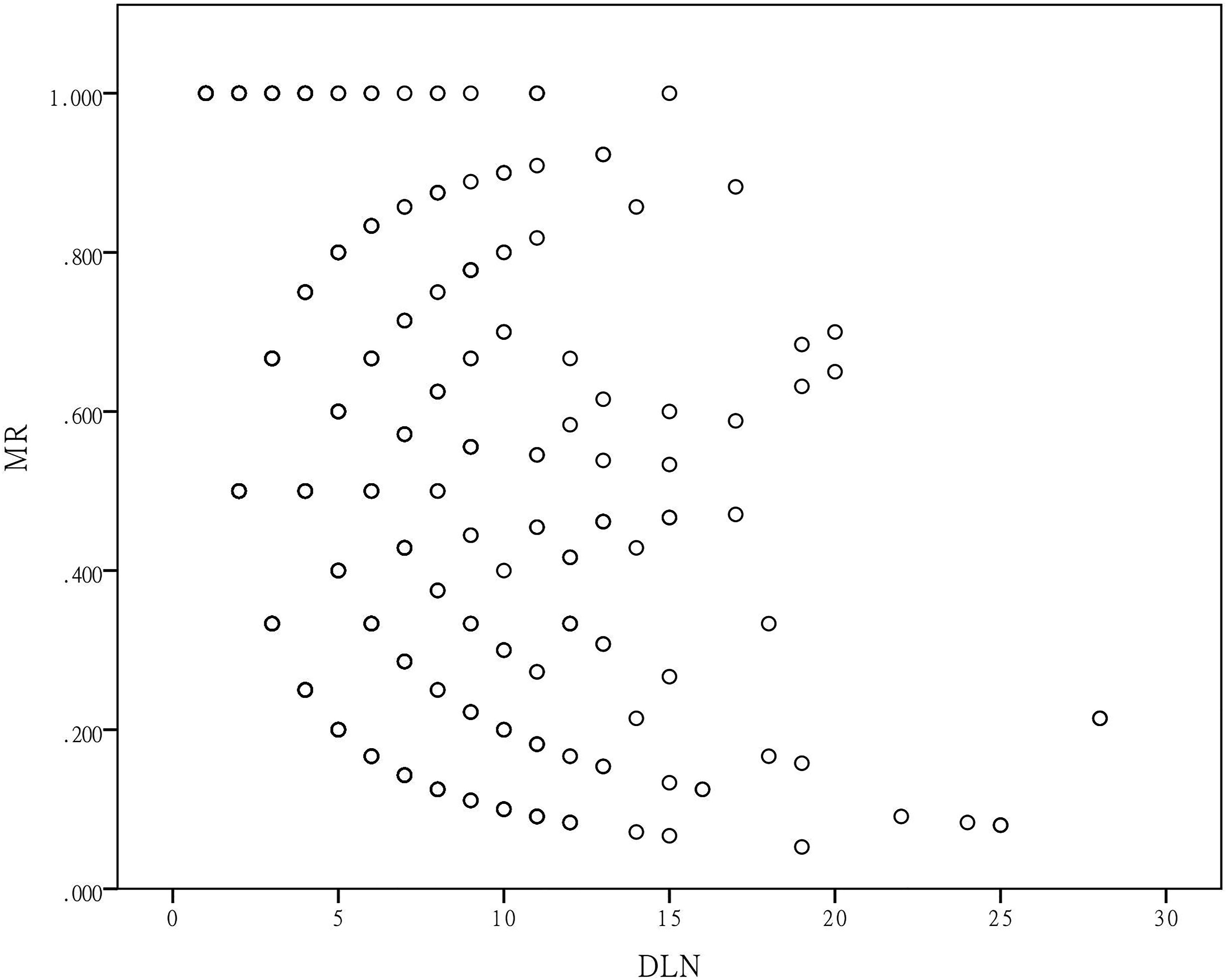
Scatter charts and Spearman tests showed positive correlation between DLN and MLN (ρ = .480, P = .000) (Figure 1), while negative correlation between DLN and MR (ρ = −.394 P = .000) (Figure 2). Correlation between dissected lymph nodes and metastatic lymph nodes. Correlation between dissected lymph nodes and metastatic ratio.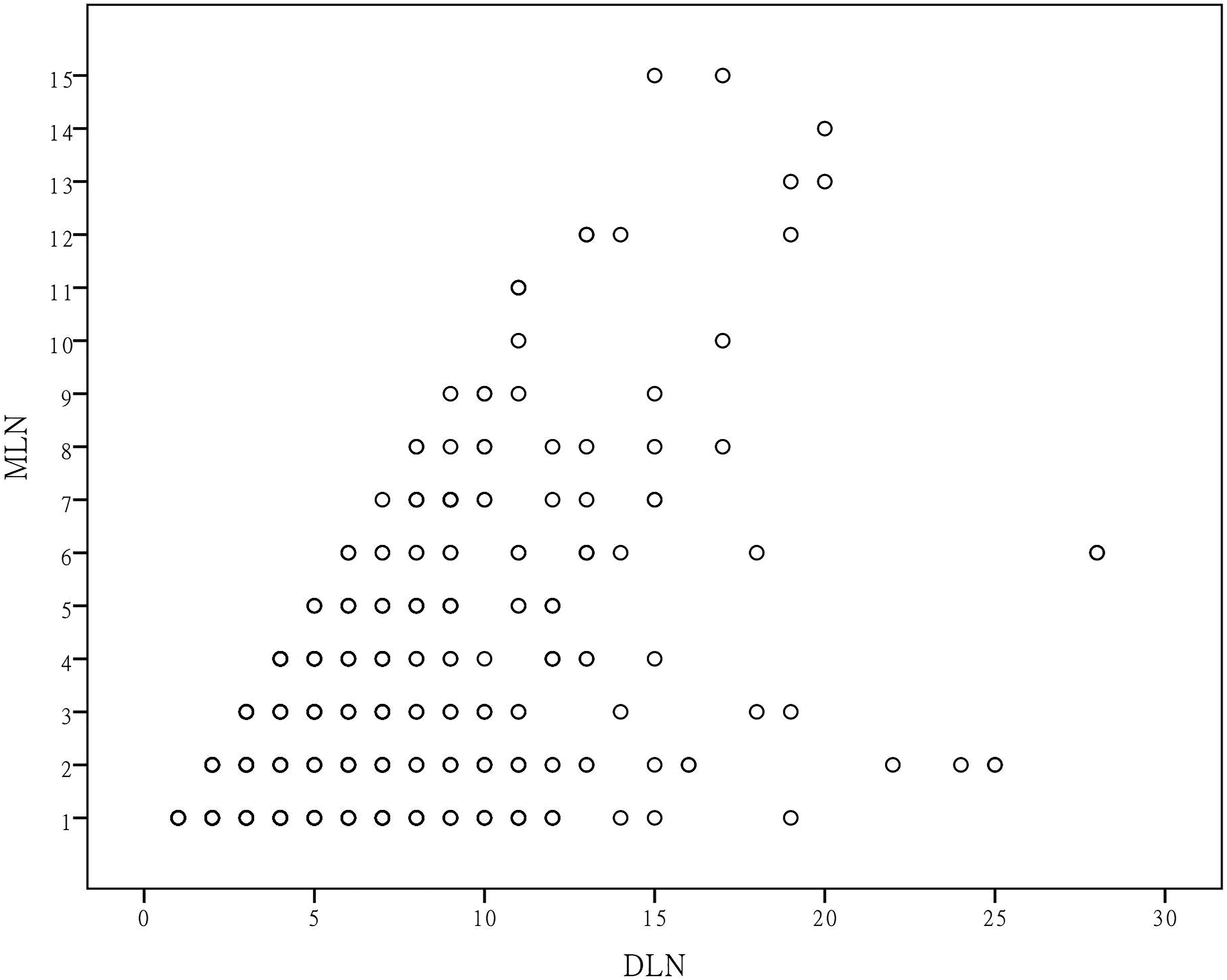
Comparison of Lymphadenectomy Results in Different Lobes.

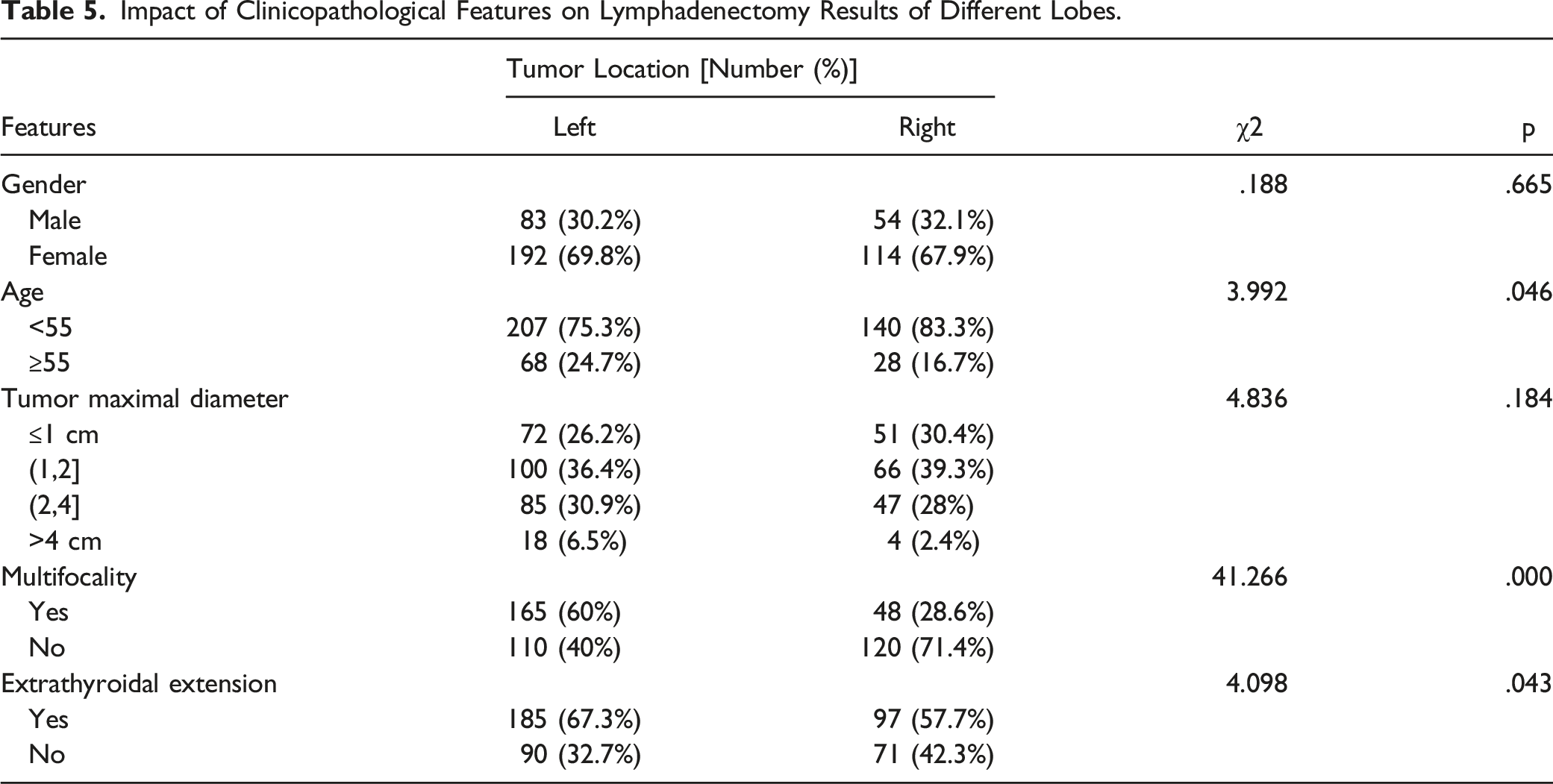
Impact of Clinicopathological Features on Lymphadenectomy Results of Different Lobes.
Discussion
Active surveillance has been applied to low-risk papillary thyroid microcarcinoma patients and proved to have low rates of size enlargement and appearance of nodal metastasis; over 70% of these cases did not progress with up to 10 years of follow-up. 9 However , even though the majority of early-staged patients followed our advice for active surveillance rather than surgery, and despite prophylactic lymph node dissection being performed on noninvasive, cN0 stage T1 or T2 PTC was not recommended according to ATA guidelines, 10 and patients with smaller tumors accounted for the majority of patients in this study (≤1 cm: 27.8%; 1–2 cm: 37.5%). We surmise that this may reflect the concern patients have with “watchful waiting” of a cancer, even if they are given reassurance about the relative innocence of very small PTCs and the excellent survival if subsequent surgery were to become necessary.1,11,12
Thyroidectomy with central compartment lymph node dissection for advanced and high-risk early-stage PTC is recommended by ATA guidelines. 10 Then, what extent of lymphadenectomy should be considered standard and adequate? Our experience demonstrated a wide range in the number of lymph nodes dissected (1–28), yet 53.5% cases had only 6 or fewer DLN. Therefore, from these data, it is difficult to delineate an appropriate value as a “threshold” for the minimum number of dissected lymph nodes to be considered adequate. Although we found more DLN in the right level VI than the left, there was no significant difference in MLN between the two. While this resulted in a lower MR of right side, similar to previous publications,7,8,13 this ratio seems somewhat artificial and less meaningful in this circumstance. The presence of VIb lymph nodes deep to the right recurrent laryngeal nerve may be the reason, compared to the direct anatomic course of the left RLN along the posterolateral aspect of the trachea.
Statistical analysis showed both MLN and DLN were higher in patients <55 years old. Young age has been shown to be an independent risk factor for lymph node metastasis,14,15 but usually refers to teenage or patients in their twenties. TMD ≤1 cm cases had more frequent MLN than cases with TMD >2 cm is a somewhat “odd” result. Review of the pathological data, however, showed that ETE of larger tumors could sometimes cause malignant adherence of tumor, lymph nodes, and surrounding soft tissues as an aggregate “cancer focus” that could have affected the count of individual lymph nodes. In addition, the small number of cases of advanced tumors could also have affected the accuracy of statistical results. It seems counterintuitive as to why more lymph nodes were obtained in patients without multifocality or ETE, but the statistical analysis did show a higher chance of HMR in patients with features above. As one of the independent risk factors for PTC, men in the study also showed a higher rate of HMR. These results are consistent with other studies on risk factors of PTC.4-6,15-17 However, no differences in HMR rates were found between tumor sizes, suggesting that standardized lymph node dissection should be performed equally in N+ patients, regardless of tumor size.
Correlation analysis showed an inverse correlation between DLN and MR, and χ2-test indicated a higher LMR rate in LDLN, which suggested that lymph node number not only depends on tumor spread but could be influenced by other factors. Therefore, a “berry-picking” approach to lymph nodes is not advisable; thorough lymph node dissection can reduce the rate of overlooked positive lymph nodes.
With the quantification results and pattern we found in pN1a PTC patients, lymphadenectomy results were impacted by several factors, but precise, thorough, and careful central compartment dissection can ensure resection of metastatic nodes. Surgical complications are mostly temporary and can be minimized within acceptable limits.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Fujian Provincial Health Technology Project (Grant number: 2019-CXB-7) / (Grant number: 2019-ZQNB-4); Joint Funds for the innovation of science and Technology, Fujian province (Grant number: 2019Y9035); Natural Science Foundation of Fujian Province (Grant number: 2021J01446) / (Grant number: 2019J01190).
Ethical Statement
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Data Availability Statements
The data that support the findings of this study are available on request from the corresponding author.