
Abstract
Complete laryngotracheal separation is a rare life-threatening trauma that may occur due to road traffic accidents. Unfortunately, this injury may be missed if emergency physicians were not aware of its possibility. We present a pediatric patient who had complete laryngotracheal separation and esophageal injury caused by strangulation with a headscarf while riding a four-wheeled motorcycle. The neck on external examination showed only a ligature mark without open wounds. The injury was identified while attempting tracheostomy as the patient had a decreased oxygen saturation and was aphonic. The patient underwent complete airway reconstruction and stenting as well as low tracheostomy with complete reconstruction and anastomosis of the esophagus. The patient was decannulated after a few weeks with the vocal cords in paramedian position and no aspiration. This case demonstrates that early prompt treatment can save the patient’s life and result in good functional outcomes.
Introduction
Laryngeal trauma is an uncommon, life-threatening condition. 1 Complete laryngotracheal separation (LTS) is the most severe form of laryngeal trauma and corresponds to the fifth group in the Schaefer–Fuhrman classification. 2 Early proper airway management within the first few hours following trauma is crucial in such cases for the patient’s survival. As laryngeal trauma accounts for less than 1% of all traumas admitted to the emergency department, 3 some physician might not be familiar with its diagnosis and management. This exposes the patients to delayed diagnosis and inappropriate management with poor outcomes. 4 The diagnosis of LTS requires a high index of suspicion to identify the condition in an apparently normal-looking neck of a trauma victim. We present a case of a pediatric patient who sustained LTS in a road traffic accident after strangulation with her headscarf.
Case Report
A 12-year-old-girl presented to the emergency room (ER) with the help of a driver who saw her at the site of a road accident after she was strangulated with her headscarf while riding a four-wheeled motorcycle. The girl was medically free before the presentation to our ER. On primary assessment, she was alert, conscious, oriented, and aphonic. She was having a mild supra-sternal retraction and soft biphasic stridor. A clear demarcated strangulation line was detected on her neck, with no other external wounds. The oxygen saturation was 90–92% on 15 L non-rebreather face mask.
Rapid fiber-optic assessment showed the vocal cords fixed in a paramedian position bilaterally, with a strip of mucosa going up and down from the subglottic to the glottic area with inspiration and expiration, with neither cartilage exposure nor bleeding. A laryngotracheal injury was suspected.
The patient was admitted into the operating room where one trial of intubation under sedation was attempted but failed. A clear cuff leak with air bubbles was noticed. As oxygen saturation was declining, emergency tracheostomy was attempted. After a quick vertical anterior neck incision, the trachea was seen just above the sternal notch completely separated from the larynx. A 6.5-F cuffed endotracheal tube was inserted into the separated trachea and fixed with two stay sutures to the skin to prevent slippage of the trachea to the mediastinum. The examination revealed complete separation of the cricoid and thyroid cartilages from the trachea, complete laceration of the thyro-cricoid membrane and the esophagus (except for a small part of the posterior esophageal wall), and significant pharyngeal injury. Bleeding was controlled, and the patient’s vital signs were stabilized (Figure 1). Lacerated anterior esophageal wall (the rigid esophagoscope can be seen peaking through the perforation).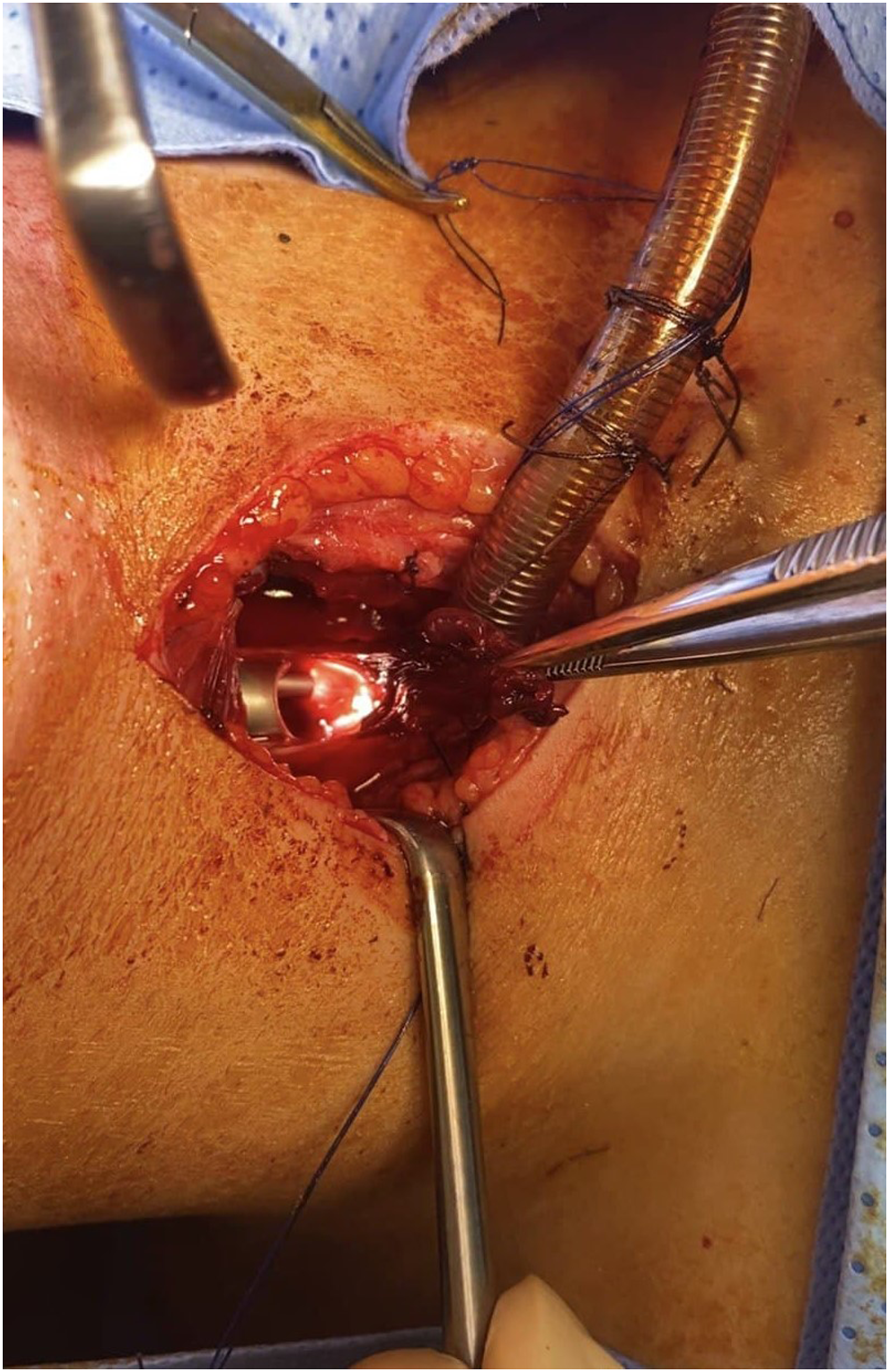
Neurosurgical consultation excluded cervical injury after undergoing a computed tomography (CT) of the neck with intravenous contrast. Chest radiography revealed massive surgical neck emphysema with right pneumothorax. The cardiothoracic consultant inserted a right-sided chest tube. After completion of primary and secondary survey, the airway surgeon performed esophageal repair under esophagoscopy guidance followed by nasogastric tube (NGT) insertion. Airway reconstruction was then performed by releasing and approximating the trachea with laryngotracheal anastomosis by multiple simple interrupted vicryl sutures and stenting with a 6-F endotracheal tube (ETT) to ease lacerated mucosa healing without eventual scarring. Stent was fixed by proline suture and knotted superficially under the skin. Low tracheostomy was performed away from the anastomosis site with a 6.5 cuffed non-fenestrated tube. Care was taken to provide good hemostasis and restore the lacerated mucosa and thyroid tissue (Figure 2). Intraoperative assessment of the patient: (A) Insertion of the tube into the trachea and (B) approximation of the two separated parts of the airway. Note the mark of strangulation on the skin above the surgical wound.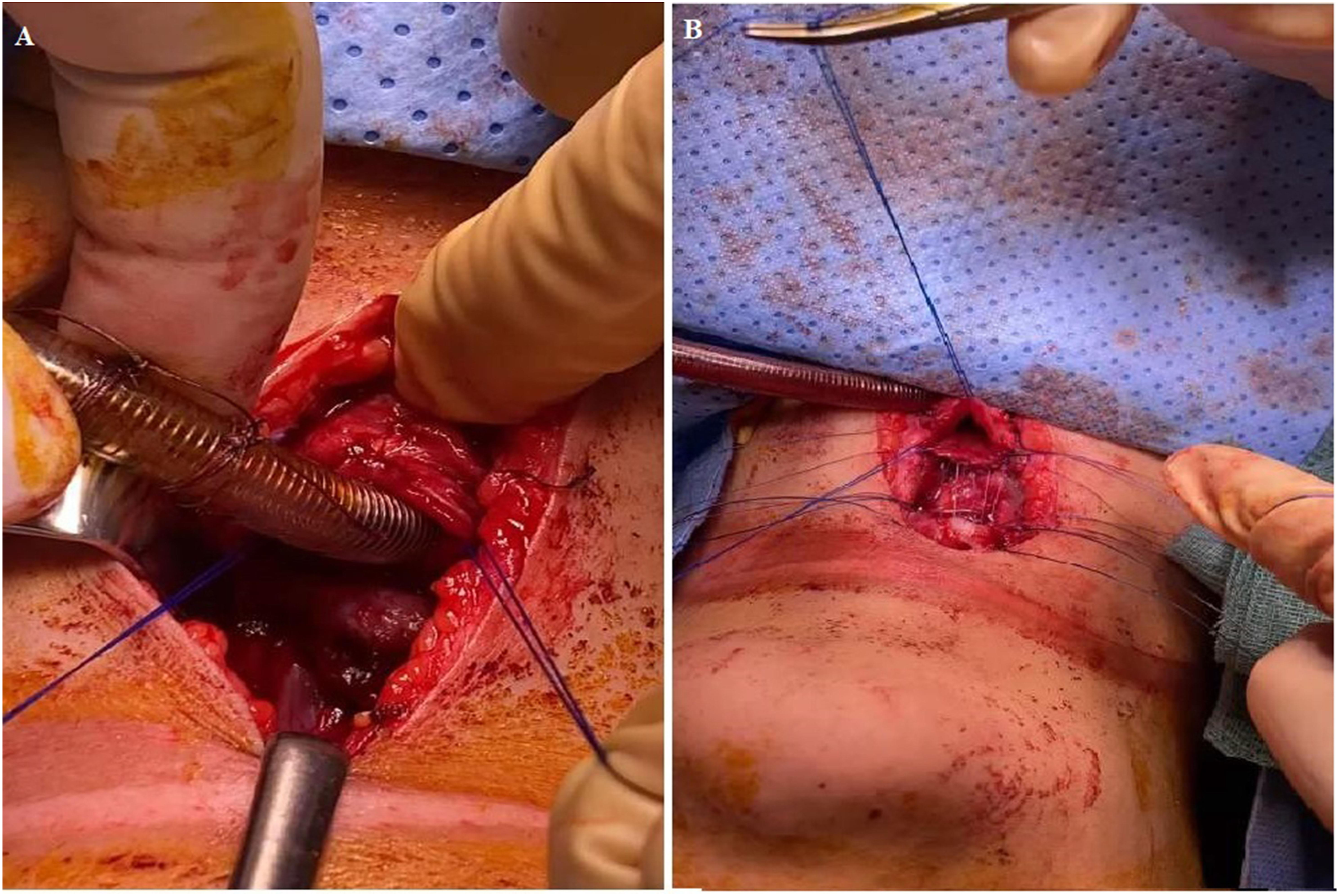
Postoperatively, the patient was sent to the intensive care unit on mechanical ventilation. The patient was weaned from the ventilator on second postoperative day. On the 10th postoperative day, the tracheostomy tube was changed to a smaller size (6 non cuffed, fenestrated tube), and modified-Gastrografin swallow studies were performed and showed no extra esophageal leak with minimal aspiration through the airway stent.
Three weeks postoperative, the patient underwent a second-look surgery of direct laryngoscopy and bronchoscopy and stent removal. Minimal aspiration was detected by modified-barium swallow fluoroscopy with thin consistency. Oral feeding started with thickened formula, and the NGT was kept for fluids. After 3 weeks, the fiber-optic assessment showed paramedian vocal cord position and no aspiration. The patient underwent NGT removal and tracheostomy tube decannulation, and she was discharged home after a few days and the follow-up was uneventful with a good voice and airway outcomes.
Written informed consent for the patient information and images to be published was provided by the patient’s guardian.
Discussion
Laryngotracheal separation is a rare life-threatening trauma. The low incidence of LTS is attributed to the protection of the larynx and trachea by the mandible and sternum. 5 The occurrence of esophageal injury in association with LTS, as in the present case, is even rarer, with approximately less than 30 cases reported in the literature. 6
Complete LTS is encountered mainly in road accidents but may be caused in some cases by strangulation or hanging. 7 Several mechanisms may cause LTS, including a direct anterior neck impact, sudden deceleration with neck flexion-extension causing shearing at the relatively fixed points of the cricoid and carina, compression of the sternum, or rupture due to closure of the glottis while the intrathoracic pressure increases. 8 In our patient, LTS occurred presumably due to strangulation by her headscarf during the accident.
The risk of LTS is higher in the pediatric population sustaining blunt neck trauma than in adults due to the less developed ligaments and membranes holding the trachea. 9
In some cases, the transected trachea may be pulled into the thoracic cavity, adding to the difficulty of managing the injury.8,10 In our patient, the trachea was seen just above the sternal notch, and the use of stay sutures prevented its slippage downward.
Patients with LTS usually present with neck wounds, surgical emphysema, dysphonia or hoarseness, stridor, dyspnea, and respiratory distress. 11 Chest imaging reveals pneumomediastinum or pneumothorax in most patients. 12 Unfortunately, the non-specific manifestations of LTS and the presence of other serious injuries in other body regions contribute to delaying the diagnosis in several cases.
The diagnosis can be easily missed if no open neck injury is observed, as in our patient, but holding a high index of suspicion when examining victims of neck trauma helps to identify such cases. The presence of subcutaneous emphysema should direct the attention to airway injury as it is the commonest reported sign.13,14 Another important rule for clinicians to remember is that the severity of symptoms does not always correlate with the degree of injury. 2 This may be partly explained by the formation of an intact sheath of soft tissues and fascia of the neck in many patients, allowing for breathing and ventilation. 15
Early proper management of LTS patients reduces the risk of subglottic stenosis and results in better voice outcomes and airway restoration. Stabilization of the airway represents the priority in suspected cases, with emergency tracheostomy in most cases. 1 Cricothyroidotomy is not preferred as separation is usually below its level and it may cause more damage. 16
Assessment using flexible fiber-optic laryngoscopy and bronchoscopy is crucial for the direct visualization of airway injury 15 and insertion of ETT. Care should be taken to avoid further injury that may convert a partial separation into a complete LTS. 10
A complete trauma assessment is warranted in LTS victims as other associated injuries may occur, including injuries to the cervical spine, intracranial structures, carotid artery, 6 esophagus, thyroid gland, and the recurrent laryngeal nerve. Therefore, a CT scan of the neck and chest is required in such cases to exclude associated injuries. Suspicion of esophageal injury warrants performing esophagoscopy and swallow studies. 1
Treatment of LTS with esophageal injury entails a primary repair of the esophagus and trachea. Reanastomosis of an injured recurrent laryngeal nerve needs to be considered to prevent atrophy of the laryngeal muscles and enhance voice outcomes. 17 Insertion of airway stents can help prevent mucosal adhesions and laryngeal stenosis. 11 However, stents may cause some complications such as infection, scarring, and pressure necrosis, particularly with too large stents. Scarring can cause laryngeal stenosis and hinder the mobility of vocal cords. Stents are usually placed for 2 weeks and then removed by bronchoscopy. 2
Cases with LTS may suffer some long-term complications, including aspiration, subglottic stenosis, dyspnea on exertion, and poor voice quality. 11
Our case featured several interesting aspects, including the mechanism of injury by strangulation during a road accident, complete laryngotracheal separation, the associated esophageal injury, and the subtle, non-specific clinical manifestations that did not correlate with the severity of injuries. We attribute the good outcome achieved in our case to the early diagnosis and management by an expert in airway injuries within a few hours after the trauma. The importance of maintaining suspicion of LTS in blunt neck trauma and prompt management cannot be overemphasized.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval to report this case was obtained from Asir Institutional Review Board, Ministry of Health, Saudi Arabia (approval number: REC-09-01-2022).
Statement of Informed Consent
Written informed consent for the patient information and images to be published was provided by the patient’s guardian.
Statement of Human Rights
All procedures in this study were conducted in accordance with the approved protocols of Asir Institutional Review Board, Ministry of Health, Saudi Arabia (approval number: REC-09-01-2022).