
Abstract

Significance statement
We present a patient with a retropharyngeal ectopic parathyroid adenoma who underwent dissection of the retropharyngeal space with removal of the parathyroid adenoma. Retropharyngeal parathyroid adenomas are exceedingly rare. Familiarity with potential ectopic locations for parathyroid adenoma is important when routine first line radiographic studies are equivocal. Awareness of this entity will avoid failed neck explorations and prepares the surgeon for a minimally invasive approach to surgical resection.
Case history
A 48-year-old female presented with asymptomatic hypercalcemia noted on routine lab work. Serum calcium was 10.9 mg/dL and intact parathyroid hormone (PTH) was 116 pg/mL. A sestamibi scan demonstrated a focus of uptake near the base of tongue, suggestive of an ectopic parathyroid adenoma. A 4D CT confirmed an oval-shaped enhancing lesion measuring 1.7 × 1.5 × 2.5 cm and located posterior to the pharyngeal wall on the right, at the level of the infrahyoid epiglottis.
The patient underwent a dissection of the retropharyngeal space with removal of the parathyroid adenoma (Fig 1). Following removal, there was a precipitous decrease in intraoperative PTH from 188.60 to 31.32 pg/mL. On final pathological evaluation, the lesion measured 2.6 × 1.4 × 0.7 cm and weighed 1.9 grams. Histopathological analysis confirmed the diagnosis of parathyroid adenoma. The patient tolerated the procedure well with normalization of PTH and calcium at 6 months follow-up. An intraoperative view of a retropharyngeal parathyroid adenoma (*) is shown here, such that the great vessels and sternocleidomastoid muscle are retracted laterally. The sternohyoid muscle and larynx (**) are retracted medially.
Discussion
Approximately 85% of patients with primary hyperparathyroidism (PHPT) have a solitary parathyroid adenoma. 1 Parathyroid adenomas are most commonly found in close proximity to the posterior or inferior aspect of the thyroid gland. Ectopic parathyroid adenomas are defined by their location in sites other than the juxtathyroid position and have a reported incidence of 2–22%.2-6 Ectopic parathyroid adenomas can be located at any site along their embryologic pathway of descent. 4 The most common location for ectopic parathyroid adenoma is the thymus, followed by retro-esophageal, intrathyroidal, mediastinal, and within the carotid sheath. 3
The pharyngeal pouches are embryonic structures derived from the endoderm, which comprise the thymus, parathyroid glands, and ultimobranchial body. 7 Parathyroid glands are the most common endocrine gland with ectopic location due to abnormal descent at the time of embryogenesis. The superior and inferior parathyroid glands have separate embryologic origins. Specifically, the superior and inferior glands are derived from fourth and third pharyngeal pouches, respectively. 8
The retropharyngeal location of ectopic parathyroid glands is thought to be due to the common origin of the superior parathyroid gland and the apex of the piriform sinus from the fourth pharyngeal pouch.
7
(Fig 2) If the gland fails to separate from the piriform sinus, these structures may migrate together, thereby placing the ectopic gland in a retropharyngeal location.
9
Retropharyngeal parathyroid adenomas are typically found posterior to the piriform sinus, as is shown in our patient. (Fig 3) During the sixth week of gestation, the third pharyngeal pouch forms the inferior parathyroid, thymus and pyriform fossa. The fourth pouch yields the superior parathyroid gland and the apex of the pyriform sinus. A 4D-CT of the neck shows a right retropharyngeal mass. A. An arterial phase axial image of the neck at the level of the pyriform sinus demonstrates a hyperenhancing lesion (red arrow) in the right retropharyngeal space at the level of the upper pyriform sinus. This lesion has a Hounsfield unit (HU) of 255. B. A delayed image at the same level demonstrates rapid washout of contrast of the lesion (yellow arrow) with 112 HU. C.D. Reformatted coronal and right sagittal venous phase demonstrate the washout of the retropharyngeal soft tissue with a polar vessel (green arrow) noted above the upper pole of the right lobe of the thyroid gland.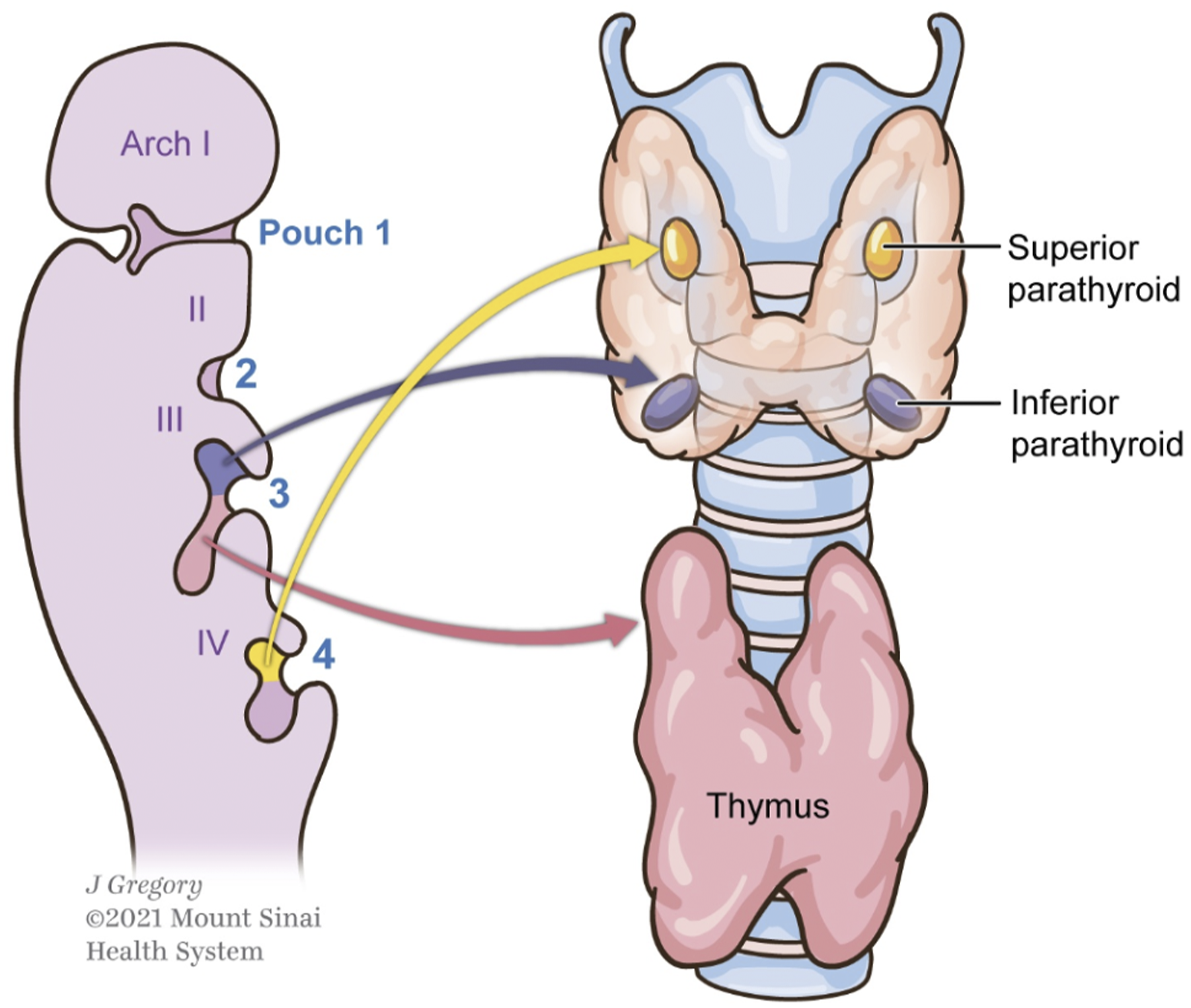

Tc-99 Sestamibi single photon emission computed tomography (SPECT) is a commonly utilized imaging modality for parathyroid adenoma localization. If this examination is negative in the setting of PHPT, then 4D-CT or MRI are often employed. In our case, the retropharyngeal adenoma demonstrated uptake on a Tc-99 Sestamibi scan. However, because the precise location of the adenoma was not confirmed, 4D-CT was utilized and identified as the retropharyngeal parathyroid adenoma. (Fig 3)
4D-CT includes images in 3 planes. The fourth dimension is the perfusion information derived from non-contrast, arterial and delayed venous phase. 10 Parathyroid adenomas are typically hyperenhancing tumors in the arterial phase with rapid washout of contrast on the delayed, venous phase.
At our institution, sonography and sestamibi scintigraphy are commonly used for localization of parathyroid adenomas. In addition to parathyroid detection, ultrasound can also inform the clinician regarding coexisting thyroid abnormalities. This method is preferred for initial work up to avoid the additional radiation dose and cost incurred by utilizing a 4D-CT. If the lesion cannot be localized by the 2 modalities, then a 4D-CT is used for localization. In some institutions, MRI is used as an imaging option for parathyroid localization.11,12 This alternative modality avoids radiation exposure and has a similar sensitivity as sonography and sestamibi. 11 On MRI imaging, parathyroid adenomas can have variable T1 and T2 signals with post-contrast enhancement which can increase the sensitivity of detection of a parathyroid adenoma. 11 However, cervical lymph nodes can have a similar signal characteristic and pattern of enhancement. In addition, respiratory motion can further limit confident detection of these lesions on MRI imaging.
In the past decade, less invasive surgical methods have been used for resection of parathyroid adenomas. This is mostly due to improved preoperative localization by newer and complementary imaging techniques. Minimally invasive parathyroidectomy (MIP) is performed through a small midline incision and is used for small, well-localized tumors. MIP is specifically used for treatment of single-gland disease and has largely replaced standard cervical 4 gland exploration. 11 In addition, superior imaging localization has permitted transoral robotic resection of retropharyngeal adenomas.13,14 Awareness of retropharyngeal ectopic parathyroid adenomas will help surgeons avoid failed neck explorations and prepares them for a minimally invasive approach to surgical resection.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.