
Abstract
After removal of a large frontal sinus osteoma in this case, the contralateral nasofrontal canal was opened to drain the intraoperative fluid and prevent infection, and the defect in the orbitofrontal area was restored using a titanium mesh designed with 3D printing technology.
Introduction
Most osteomas occur in the frontal sinus, one of the paranasal sinuses. 1 Giant frontal sinus osteomas are manifested by headache, local pain, facial deformity, nasal obstruction, epiphora, proptosis, decreased visual acuity, and diplopia.2,3 Current methods to remove osteomas include endoscopy, open surgery, and combination of both. However, the tumor has always a large volume and may puncture through the bone wall and into the orbit. In this condition, open surgery is recommended. 4 If drainage channels are not established after intraoperative removal of the osteoma, local effusion even intracranial infection may occur. In the present case, bilateral coronal incisions were made, and drainage was realized by opening up the contralateral nasofrontal canal through 3D printing technology. A titanium mesh was used to restore the fronto-orbital shape.
Case Report
Clinical Course
An 18-year-old man presented with a progressive frontal neoplasm for over 2 months. Physical examination showed no obvious abnormalities (Figure 1). (A) The patient exhibited bulging of the forehead. B.C CT showed the maximum diameter of the mass. (B) Maximum diameter measured in an axial position. (C) Maximum diameter measured in a coronal position. (D) 3D reconstruction showed that the lateral wall and supraorbital margin were destructed by the tumor.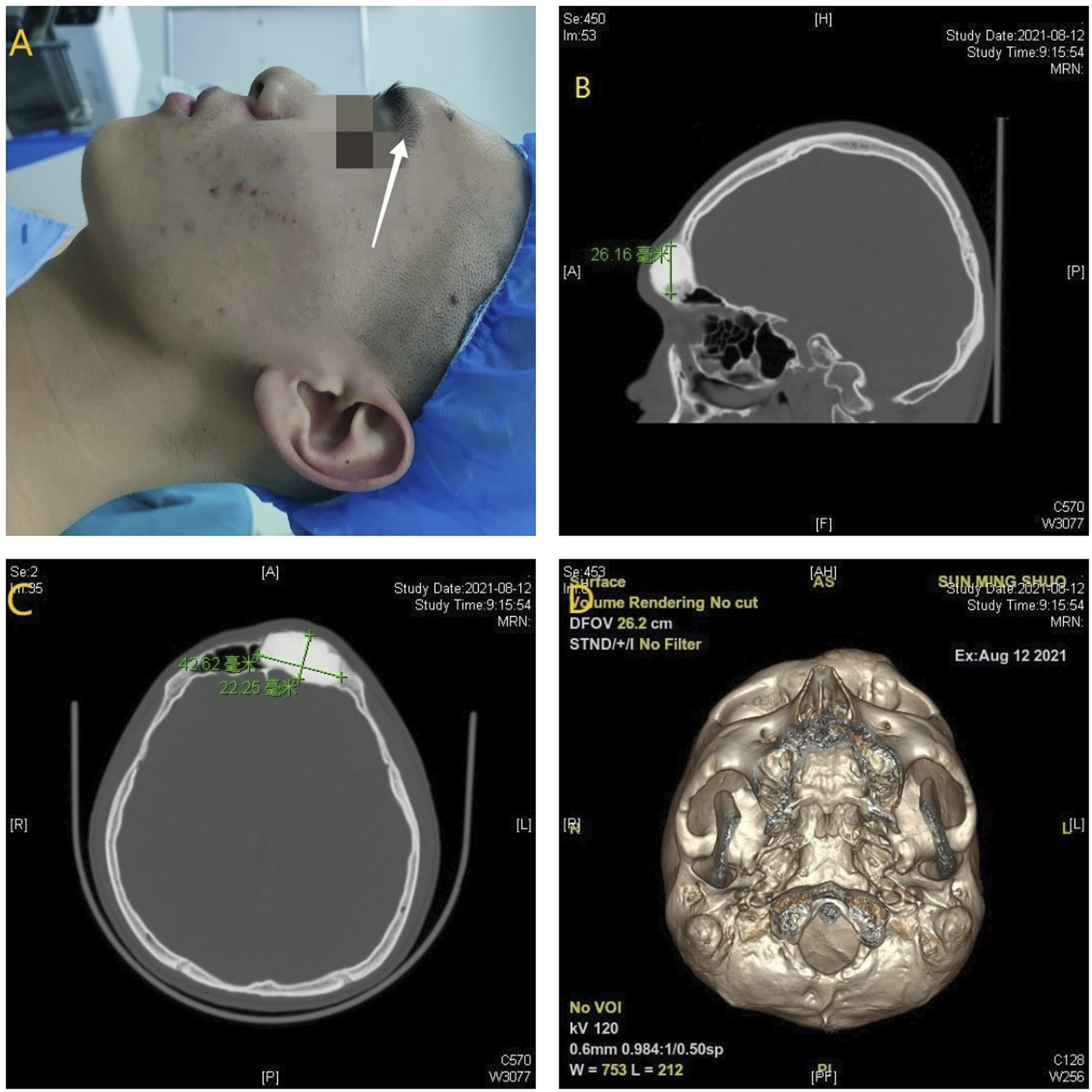
Head computed tomography (CT) displayed a well-defined high-density expansile lesion in the left frontal sinus, measuring 42.62 mm*22.25 mm*26.16 mm (Figure 1). The tumor had broken through the bony plate at the bottom of the frontal sinus and invaded the orbital roof (Figure 1).
The diagnosis of osteoma in the left frontal sinus was suspected based on imaging features.
Surgery
It is a great challenge to simultaneously reconstruct the fronto-orbital temporal framework and the drainage of the frontal sinus.
5
In this case, CT, mirror technology, and 3D printing technology were used to generate a model of the patient’s fronto-orbital temporal framework. A titanium mesh was designed to fit this model (Figure 2). The mirrored 3D model.
During the surgery, because the mass was large, a bilateral coronal incision was made to expose the fronto-orbital zone. The tumor was completely exposed. The facial nerves were protected. The tumor was encased by an intact capsule. The weak bone wall around the tumor and a circle around the tumor were cut, and the tumor was pried out intact eventually. The mass was white and dense, closely resembling bone cortex (Figure 3). Tumor tissue was sent for pathological analysis. The weak medial wall of the frontal sinus cavity was smooth and complete and did not break into the brain. The left cavity communicated with the contralateral frontal sinus. The contralateral nasofrontal canal was opened to drain the fluid and avoid postoperative infection or mucocele (Figure 3). Intraoperative imaging: (A) The tumor broke through the lateral wall of the frontal sinus, protruded on the frontal surface, breached the superior orbital margin, and entered the orbit. (B) After complete removal of the tumor, the frontal sinus communicated with the contralateral frontal sinus and the medial frontal sinus bone wall was intact, while the inferior bone wall was damaged and communicated with the orbit. (C) Pre-bent titanium mesh recreated the frontal shape. (D) The intact tumor was removed intraoperatively.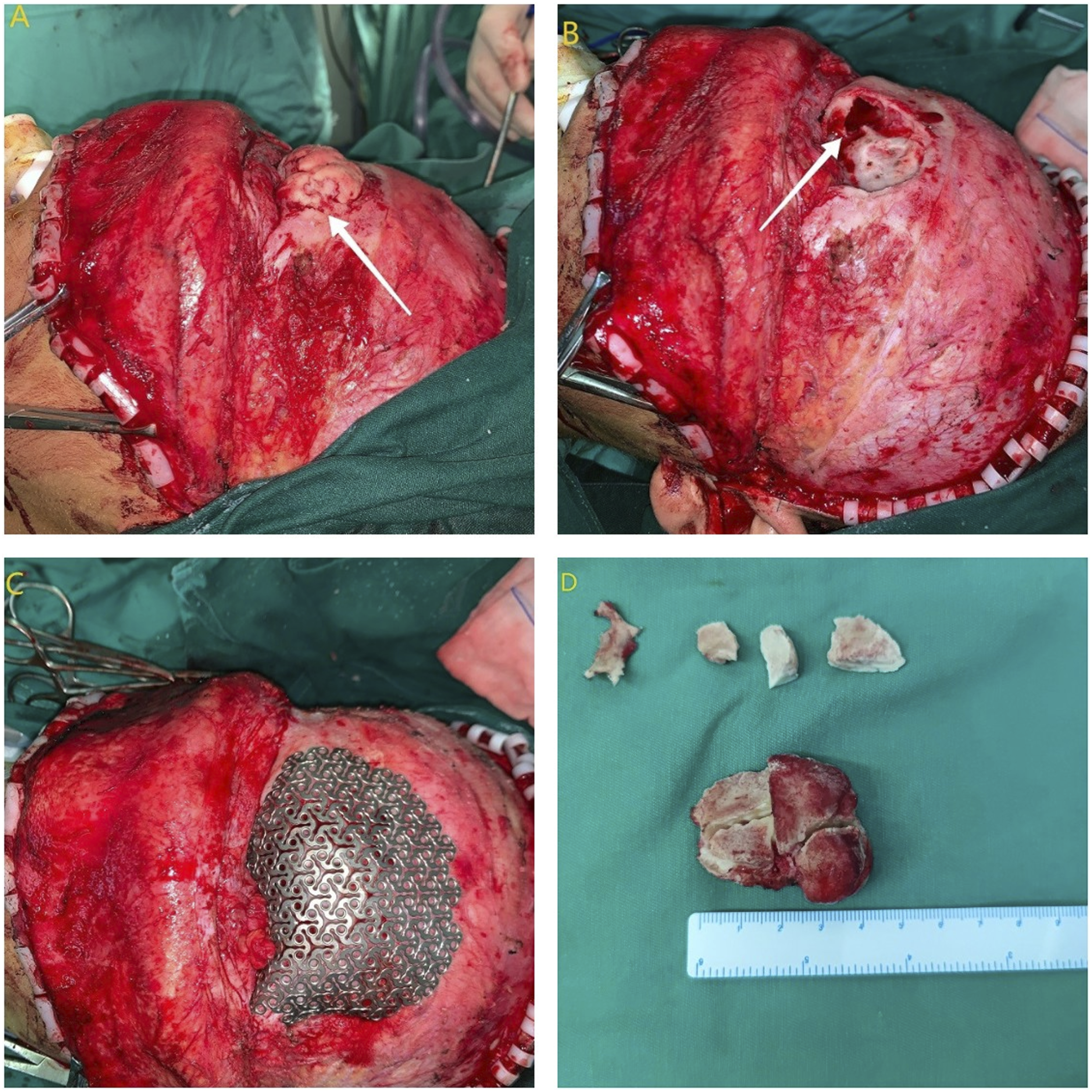
Using the model, the titanium mesh was pre-bent to fit the defect and make it symmetrical to the healthy side. A perfect frontal shape was obtained by adjusting the titanium mesh slightly to the defect.
Postoperative CT showed a perfect reconstruction of the fronto-orbital framework. At postoperative one month, sinus CT scan showed no effusion in the frontal sinus (Figure 4). (A) 3D reconstruction showed that the titanium mesh restored the shape of the frontal superior orbital margin. (B) Bilateral frontal sinuses were opened. (C) The contralateral nasofrontal canal was opened. (D) Facial appearance of the patient at 1 month after surgery.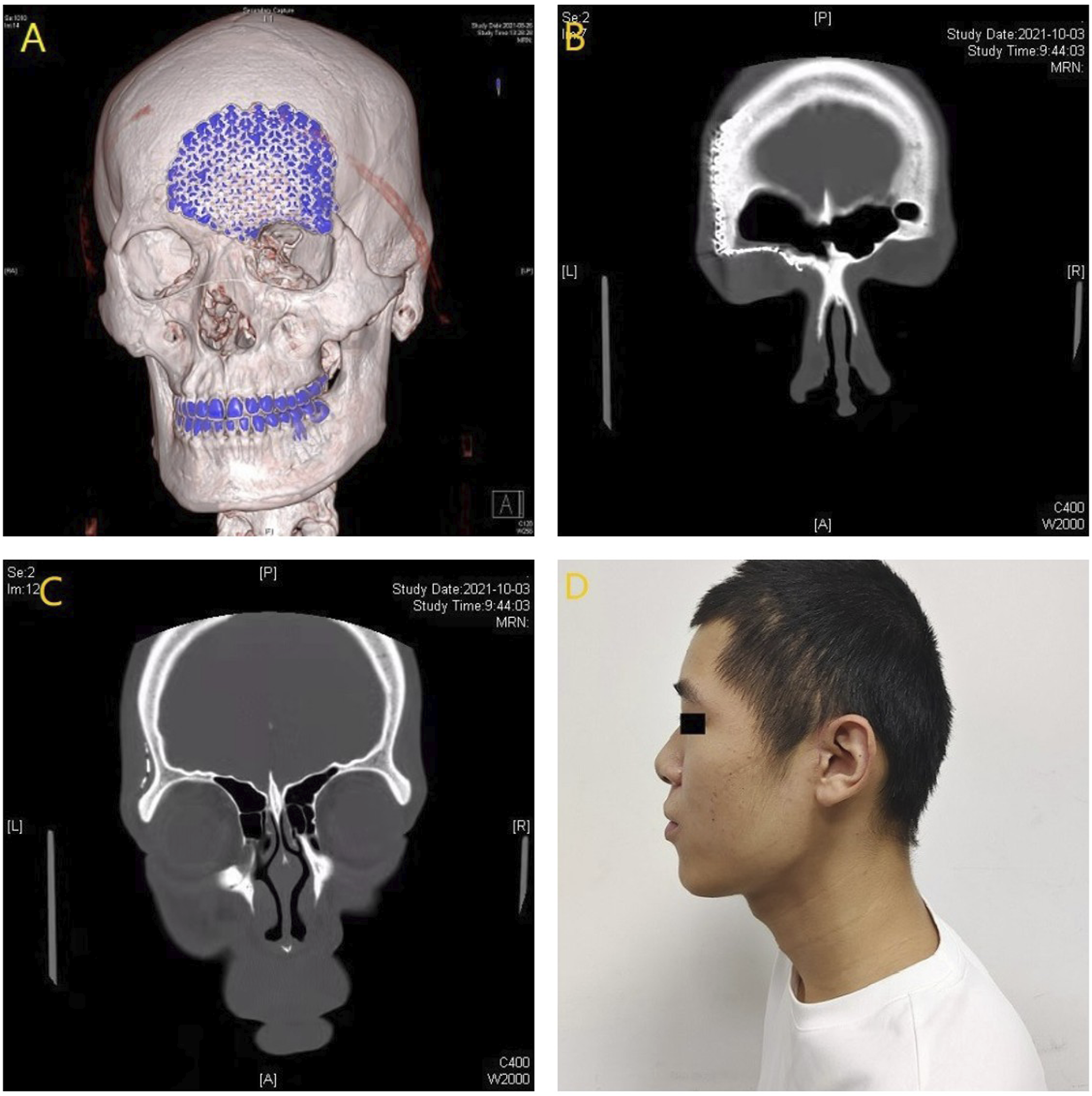
The anatomopathological study confirmed the diagnosis of osteoma.
Postoperative Outcomes
At postoperative two months, the frontal appearance was basically symmetrical without any complications. No infection occurred in the frontal sinus. Eye movement and vision were normal.
Discussion
In this case, the indications for osteoma resection were clear. Since this frontal sinus osteoma was large, open surgery was adopted, which is usually performed through bicoronal osteoplastic flap, lateral rhinotomy, and Lynch-Howarth approach. 4 In the present case, the deep orbital roof and the posterior wall of the frontal sinus were invaded; therefore, bilateral coronal incision was performed to expose the surgical field, hide surgical scars, and handle postoperative complications.
3D printing technology can bring with good functional and aesthetic effects in plastic surgery, 6 especially in repairing craniofacial curved bone defect. This technology has been used to treat frontal orbital defect after resection of frontal sinus osteoma. 5 In our case, CT, 3D printing and mirror technology were used to generate the fronto-orbital model, and then the model was used to pre-bend the titanium mesh to match the patient’s fronto-orbital framework, thus minimizing surgical damage.
Autologous bone transplantation is a standardized choice, but the implanted bone flap is difficult to survive and brings with much damage. Meanwhile, the rigidity of this material may increase the technical difficulty in creating a conformational reconstruction of the bone. 7 In comparison, alloplastic implants have emerged for reconstructing craniomaxillofacial bone defects. Hydroxyapatite and titanium mesh are often selected. Hydroxyapatite is biocompatible, osteoconductive, and osteoinductive in cranial and maxillofacial reconstruction. However, hydroxyapatite is brittle and prone to fluid leakage,8,9 thus increasing the risk of infection. Titanium is biocompatible and plastic. The porous surface of a titanium mesh facilitates tissue ingrowth,10,11 and drainage. In our case, the titanium mesh was used.
Frontal sinus infection is rare but serious, often (from 0.8 to 3%) accompanied by severe intraorbital or intracranial complications. 12 The frontal sinus outflow tract, with an hourglass shape, makes up the superior infundibulum and the inferior frontal recess, which is separated by the ostium or the narrowest portion (3–4 mm). 13 The location and anatomy of the frontal sinus are prone to serious complications. In order to prevent intrafrontal sinus infection or even intracranial infection caused by postoperative drainage obstruction, the frontal sinus should connect with the contralateral frontal sinus; meanwhile, the contralateral frontal sinus tube should be opened to facilitate fluid accumulation in the drainage area.
Conclusion
In this case, the giant osteoma was successfully removed. The fronto-orbital region was perfectly reconstructed by a titanium mesh designed according to 3D printing technology, and a nasofrontal drainage channel was dredged to avoid postoperative complications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
A statement of institutional review board
Patient involved in this study gave his informed consent. Institutional review board approval of our hospital was obtained for this study.