
Abstract

More than a third of adults in the US aged 40 years and older experience vestibular dysfunction. This number will rise—the worldwide population of those aged 65 years and older is estimated to reach 1.6 billion in 2050. 1 Here, we present our experience with age-related changes in vestibular function, known as presbyvestibulopathy (PVP). PVP, which gained formal diagnostic criteria in 2019, causes significantly decreased quality of life across multiple domains of health resulting in limited mobility and social isolation. 1
We have found that discussing the pathophysiology of PVP and imbalance with patients in the clinic can significantly ease anxiety and demystify their condition. The sense of balance is the result of complex neurological integration of multiple sensory systems, primarily vision, proprioception, and the peripheral vestibular organs of the ear. In peripheral vestibular deficiency, these other systems help functionally compensate for loss of function. 1 In an aging individual, however, reduced somatosensory function, decreased visual acuity, peripheral neuropathy, and decreased strength all contribute to diminished signal integration and diminished ability to correct for vestibular loss. Furthermore, many of these sensory and mechanical deficits progress slowly and may not be consciously recognized by the patient as a decline in function. As a patient ages, loss of balance and fear of falling result from this multisensory decline, in turn contributing to anxiety and avoidant behaviors that further reduce strength and mobility.
We approach these patients in the clinic with a careful history to eliminate other common conditions in the dizzy patient, including benign paroxysmal positional vertigo (BPPV), vestibular migraine, Meniere’s disease, and vestibular neuritis. In a 60+-year old individual experiencing gradual-onset disequilibrium with or without vertigo, PVP should also be strongly considered. The presence or absence of vertigo, hearing loss, and the temporality of symptoms (duration and frequency) can differentiate common peripheral causes of vertigo. Inciting events, substance use, and medication history should also be discussed. Asking questions regarding the patient’s daily functioning can also be revealing as to their degree of impairment. For example, asking about: falls and the falls’ circumstances, difficulty navigating in the dark or on uneven surfaces, and difficulty reading words while moving, are all helpful in discerning hypofunction. Asking about the patient’s experiences behind the wheel is also helpful—if the patient can drive without difficulty but has dizziness as a passenger in a car, this suggests vestibular migraine vs PVP. Though no PVP-specific screening tools have been tested, we routinely perform fall risk screening to efficiently identify high-risk patients with a simple 3-question inventory from the CDC’s STEADI algorithm. 2
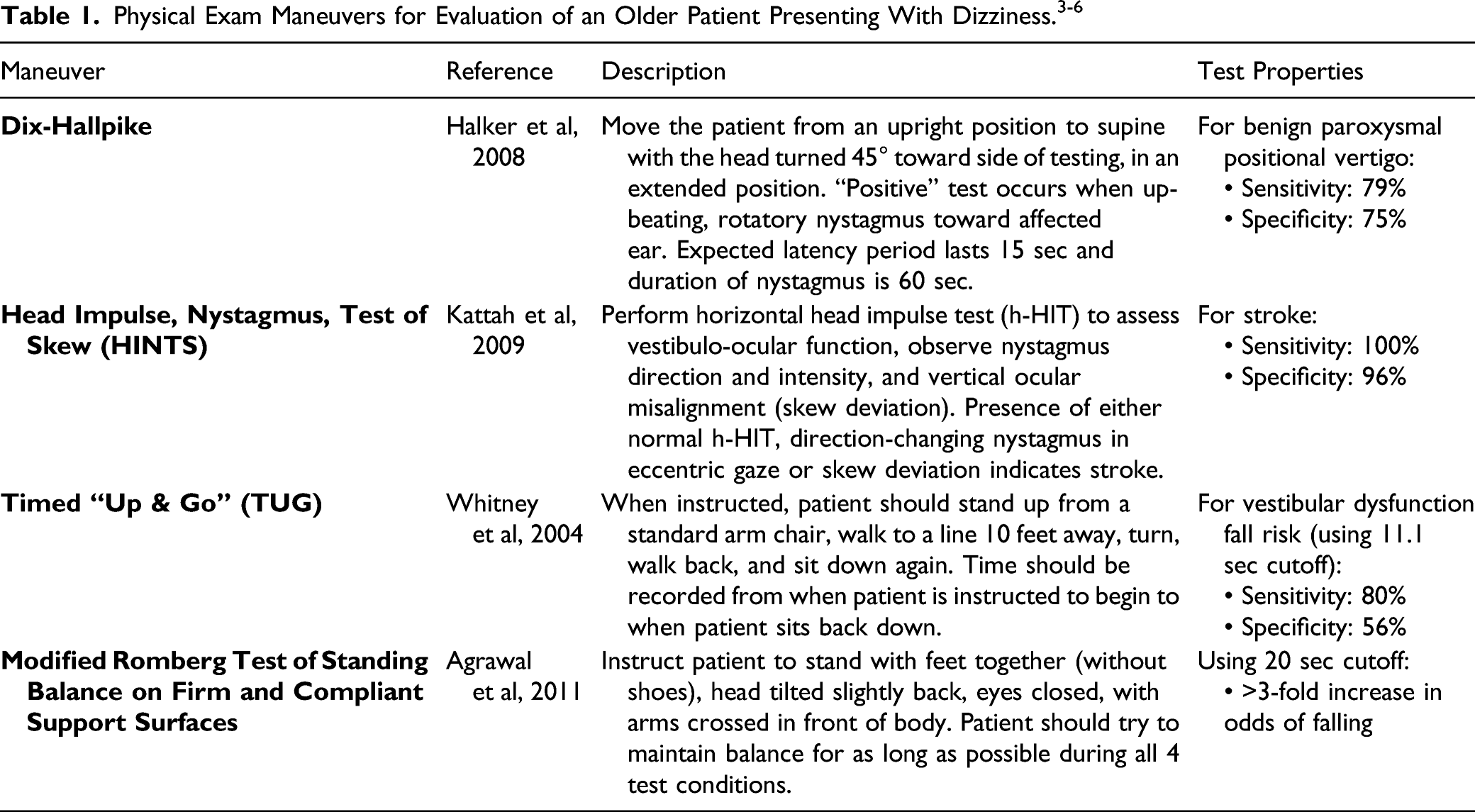
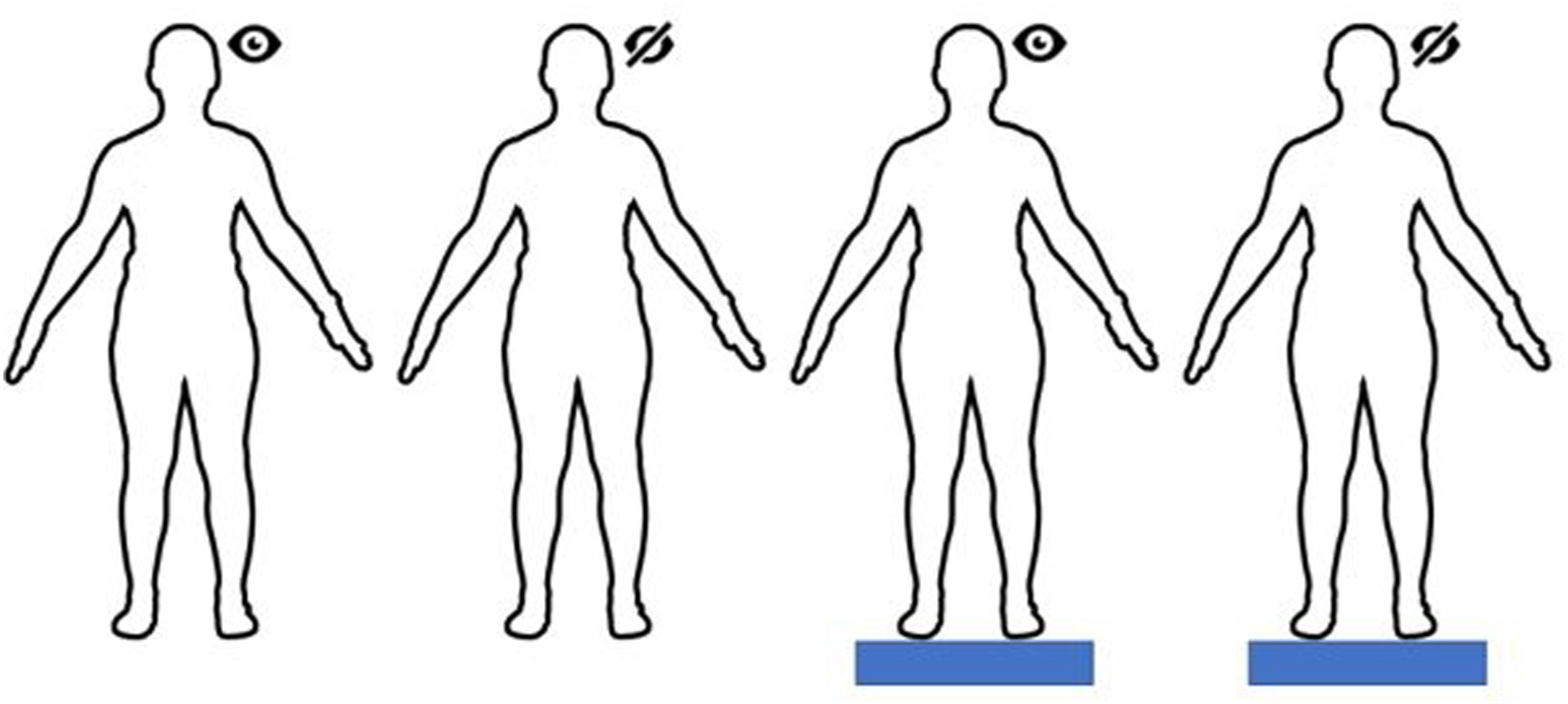
Modified Romberg Test of Standing Balance on Firm and Compliant Support Surfaces. 4 Patient spends 30 seconds in each condition. Condition parameters are as follows: 1) Eyes open, on firm surface (testing visual, proprioceptive, and vestibular inputs); 2) eyes closed, on firm surface (testing proprioceptive and vestibular inputs); 3) eyes open, on compliant surface (testing visual and vestibular inputs); 4) eyes closed, on compliant surface (testing vestibular inputs). Failure is defined as opening eyes, moving limbs to gain stability, fall, or requiring tester intervention.
We find vestibular testing to be less helpful than history and the physical exam in the diagnosis of these patients. In contrast to audiometry, a direct quantitative evaluation of hearing, tests to measure vestibular function are indirect, time-consuming, and difficult to perform accurately. Current vestibular physiologic testing assesses the vestibulo-ocular (VOR) and vestibular spinal reflexes and does not provide a single quantifiable measurement of vestibular function. These tests also require specialized equipment and a trained professional to perform, thereby limiting access for much of the population. Most vestibular disorders may be diagnosed on history and physical exam; vestibular neurodiagnostic testing should only be used in specific scenarios, in which case a referral to a neurotologist or neurologist may be helpful.
Once diagnosed, PVP must be approached in a multipartite fashion. Vestibular physical therapy and rehabilitation is a promising therapeutic management technique and the primary modality of treatment. 7 Ophthalmology screening can address visuospatial issues. Coordination with the patient’s primary care physician or a psychiatric/geriatrics referral can address avoidant behaviors and anxiety. Fall prevention education such as appropriate shoes, removing hazards in the home, and using assistive devices are all in order.
On the horizon, there are ongoing clinical feasibility trials for a multichannel vestibular implant system providing continuous, long-term, motion-modulated stimulation in the semicircular canals and address widespread loss of vestibular hair cell function. 8 This implant has already been shown to improve posture, gait, and quality of life in patients with bilateral vestibular hypofunction with unilateral implantation. 9 Apart from these options, there are no existing approaches to bypass loss of function that are analogous to hearing aids and cochlear implants.
Dizziness in the geriatric population is a complex and often nebulous phenomenon. With upcoming demographic shifts, it is imperative that otolaryngologists play a role in addressing such challenges facing our patient community.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is funded in-part by the American Otological Society (Fellowship Grant, PSK).
Ethics and Consent Statement
No Institutional Review Board was consulted for this project as this is a “Perspectives” piece that did not involve data collection or ethical approval.
Data Availability Statement
Data was not collected for this project; therefore, there is no data available to be shared.