
Abstract
Laryngeal carcinoma represents one-third of all head and neck cancers and is burdened by significant morbidity and mortality for advanced-stage disease. Surgical treatments, including Open Partial Horizontal Laryngectomy (OPHL), are often followed by long-lasting swallowing rehabilitation and more rarely, persistent dysphagia. Some authors reported single cases, successfully treated with fat injection of the base of tongue, but nowadays, a standardized technique has never been described so far. We provide a step-by-step technique description of the trans-cervical lipofilling of the base of the tongue (BOT) under local anaesthesia in a case series of three patients. The functional results have been evaluated with a videofluoroscopic study of deglutition and Penetration-Aspiration Score. The procedure was well tolerated; all patients were discharged after 24 hours without any majorcomplications. After six months, all patients had a steady improvement in swallowing. During follow-up, the videofluoroscopic study of deglutition confirmed a sensitive amelioration of the Penetration-Aspiration Score and an empowered base of tongue retropulsion. Finally, the lipofilling of the BOT under local anaesthesia showed to be a feasible, and reproducible procedure, for dysphagia after OPHLs.
Keywords
Introduction
Laryngeal squamous cell cancer (LSCC) represents one-third of all head and neck cancers. About 200 000 new cases of laryngeal cancer were diagnosed in 2017 worldwide and recent studies show that the incidence and prevalence have both increased by 12.0% and 23.8%, respectively, during the past three decades. 1 Surgical function sparing strategies include both Transoral Laser Microsurgery (TLM) and Open Partial Horizontal Laryngectomy (OPHL), but dysphagia is a common complication after conservative treatments. 2 Most patients will experience dysphagia during the first 3 months and will undergo long extensive rehabilitation, or eventually in a minority of cases, they will depend on a fully nasogastric tube nutrition because of persistent aspiration or even treated with total laryngectomy. 3 Reaching a good compromise between oncologic radicality and good functional outcomes is not easy, especially in the case of postoperative radiation. Most patients will benefit from at least three months of postoperative rehabilitation for speech and deglutition. The incidence of late functional complications (more than 3 months after surgery) is esteemed to be low, with about 1.3% of patients referred to total laryngectomy because of persistent aspiration pneumonia. 3 The mechanisms underlying persistent dysphagia may be several, including incomplete neoglottis closure, delayed opening of the upper oesophagal sphincter or impaired retraction of the base of the tongue (BOT). 2 Some authors have successfully reported about the fat injection or polydimethylsiloxane of the BOT in treating chronic dysphagia, speculating about how this procedure might improve the protection of the airway and reduce the oropharyngeal pooling due to tissue loss.4-7 This work describes a modified technique of transcervical lipofilling of the BOT under local anaesthesia, providing a high-quality pictorial step-by-step description of the technique and the promising preliminary outcomes in three consecutive cases affected by persistent dysphagia after OPHLs and residual impaired BOT retraction.
Case reports
Patients’ clinical characteristics.
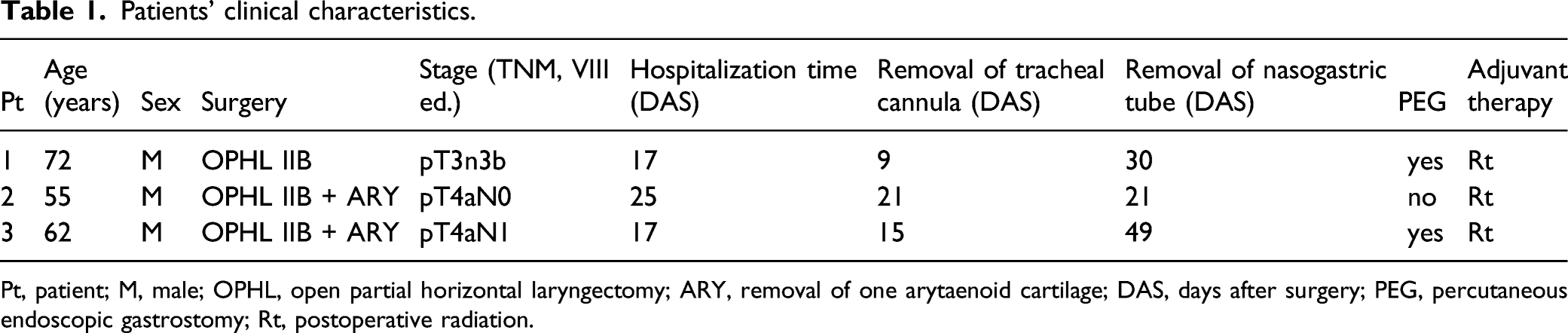
Pt, patient; M, male; OPHL, open partial horizontal laryngectomy; ARY, removal of one arytaenoid cartilage; DAS, days after surgery; PEG, percutaneous endoscopic gastrostomy; Rt, postoperative radiation.
Surgical technique
Step 1
The patient is put supine under local anaesthesia. Klein’s solution is prepared to be injected into the abdominal donor site before start the procedure. The abdominal region is injected with about 200 ml of Mepivacaine enriched solution about 15 minutes before the fat harvesting. Fat harvesting is performed according to the well-known technique by Coleman et al.
9
After a small skin incision, a blunt tip harvesting cannula (3 mm in diameter) is inserted while exercising a low negative pressure. The cannula is attached to a 10 cc Luer-Lock syringe. The very purified fat is obtained through an automated centrifugation, washing and decantation processing system that permits to separate the pure fat from the cell debris, the oily fraction, the remnant watery fraction consisting of blood and residual Klein’s solution (Figure 1A and B). (A) and (B) The patient is put supine under local anaesthesia, fat harvesting with blunt tip cannula attached to a 10 cc Luer-Lock syringe.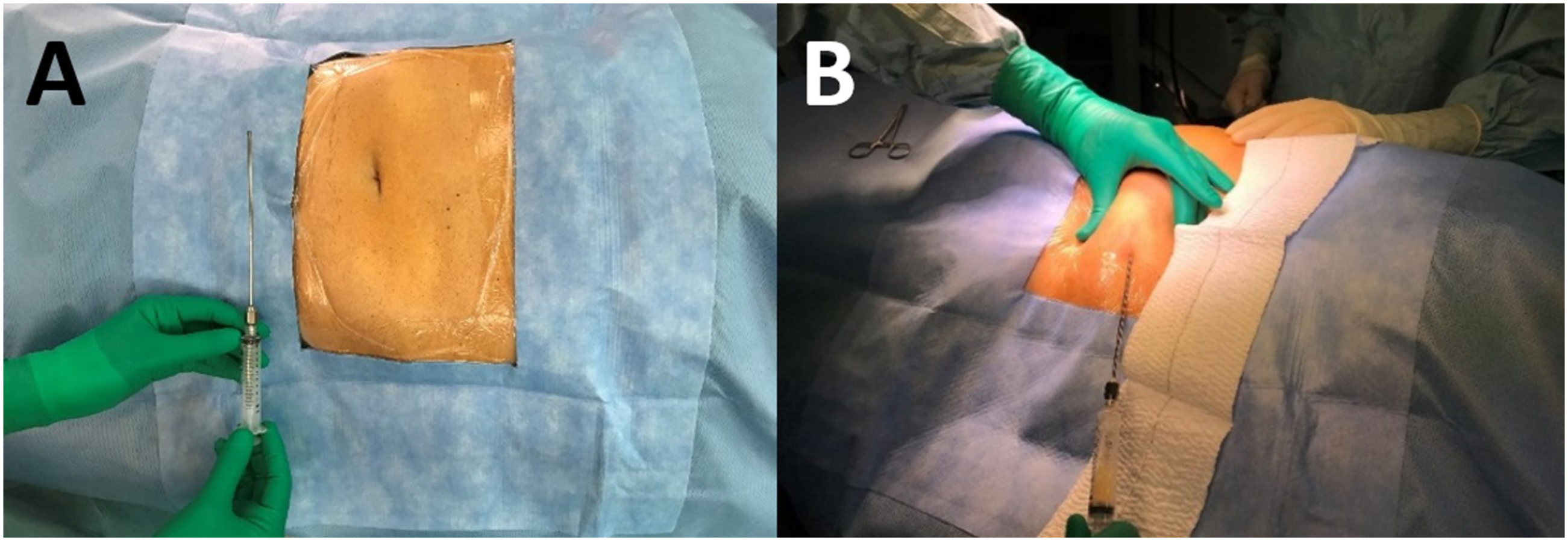
Step 2
The target region for fat infiltration is set preoperatively on the base of the preoperative CT scan. On the sagittal reconstruction images, the surgeon identifies three pointers defined as follows: the mandible symphysis (A), the hyoid bone (B), the middle distance between ‘A’ and ‘B’ (C). The region for fat infiltration is identified between an ideal perpendicular line conducted from ‘C’ to the submucosal layer of the BOT and a second line that runs from ‘C’ to the superior border of the hyoid bone. The angle between these two lines is patient-specific and corresponds to the portion of the tongue which actively contributes to the arytaenoid-BOT contact (Figure 2). The patient is put in a 45° angled position, the surgeon identifies on the preoperative CT scan and in vivo the three pointers: (A) the mandible symphysis; (B) the hyoid bone; (C) the middle point between ‘A’ and ‘B’.
Step 3
The patient is placed in a 45° angled position, and the submental region is injected with a 2% Lidocaine solution for local anaesthesia. After about 10 minutes, the surgeon proceeds to fat transfer at the level of the median lingual raphae, using a 20-Gauge needle. Meantime the bedside assistant performs a fiberoptic examination of the upper aerodigestive tract for intraoperative visual control of the BOT augmentation. The fat is injected until allowing full contact between the tongue and the residual arytaenoid cartilage during the deglutition, always preserving the patency of the upper airways. In the case of patients with one residual arytaenoid and an asymmetric arytaenoid-BOT closure, about 30% of the fat can be injected with a lateral angle of infiltration, which is patient-specific and set at the preoperative CT scan axial reconstructions (Figure 3). Intraoperative view. The fat is injected at the level of ‘C’, the bedside assistant performs a fiberoptic examination of the upper aerodigestive tract, for intraoperative visual control of base of the tongue augmentation.
Results
Patients’ Penetration-Aspiration Scale Score. Comparison between preoperative data, with postoperative results about 1 month after the procedure. Such results were thus confirmed at the 1-year follow visit.
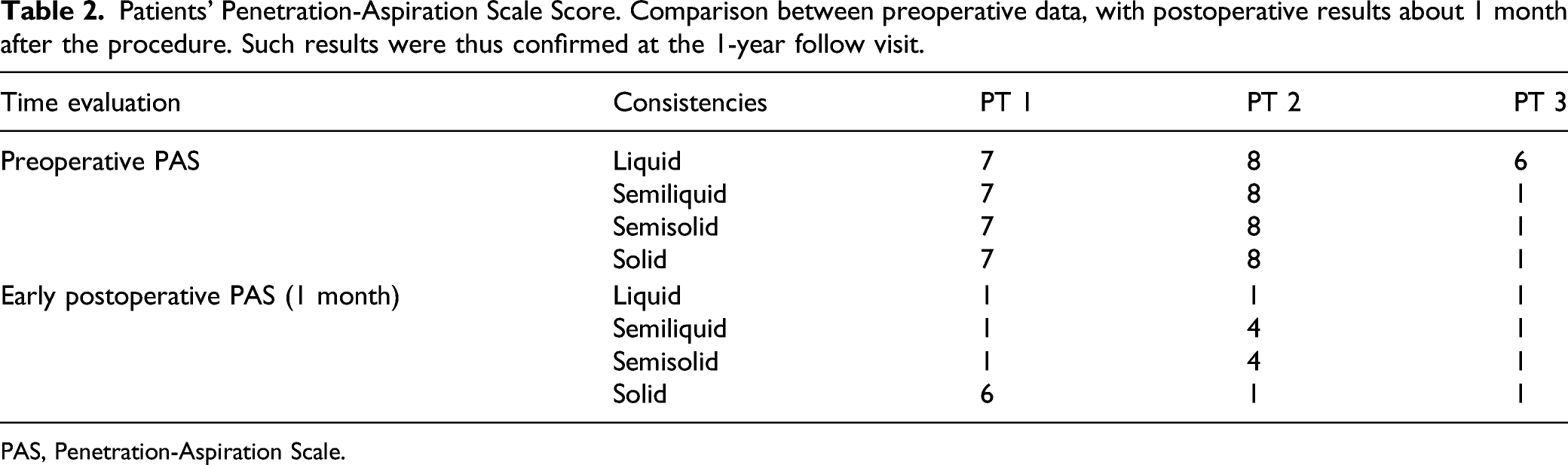
PAS, Penetration-Aspiration Scale.
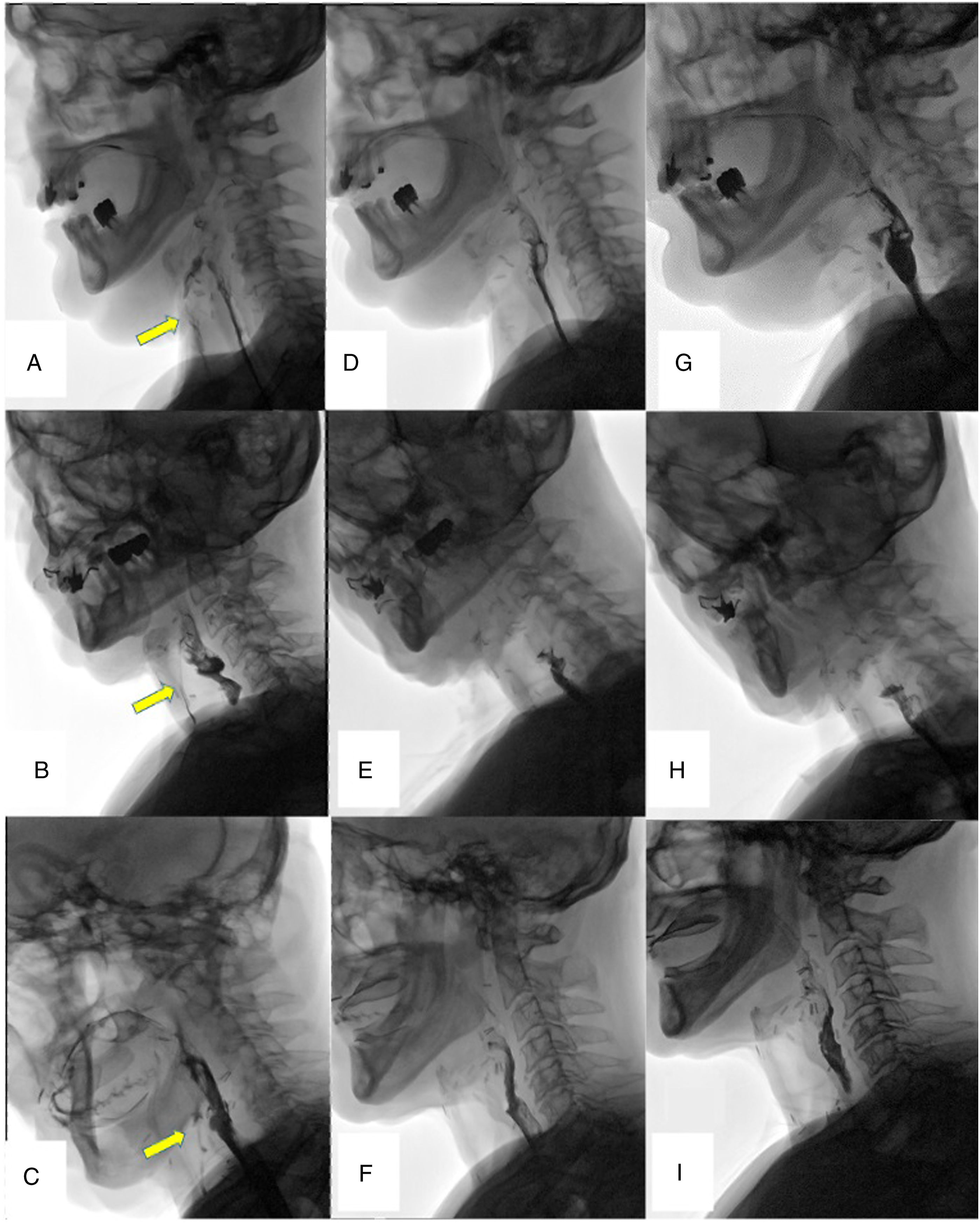
(A)-(I) Videofluoroscopic evaluation of swallowing with barium liquid bolus. At the preoperative images (A)-(C), the yellow arrow points to the radiological signs of tracheal inhalation. At early postoperative images after 1 month (D)-(F) and follow-up evaluation after 1 year (G)-(I), the barium liquid bolus flows into the pharynx and oesophagus without any sign of inhalation.
Interestingly, all patients benefitted from a subjective improvement in phonation, which was confirmed at the vocal analysis, thus resulting from an augmented maximum phonation time. Further data about quality of voice should be evaluated in a future prospective cohort study.
Discussion
Recently, Literature evidence shows that dysphagia is a common complication after OPHLs, depending on a wide range of factors which include the type of reconstruction, training by swallow therapist, radiation, arytaenoid resection, extended procedures and age. 2 Most patients will experience dysphagia during the first 3 months and will benefit from long extensive rehabilitation, while in a minority of cases, late dysphagia (more than three months after surgery) will restrain patients to fully tube-dependent nutrition or even total laryngectomy because of persistent aspiration. 2 Pre- and postoperative swallow rehabilitation aim at achieving compensatory postural changes of the head, increasing the sensory stimuli with the cold bolus, and finally, strengthening the musculature of the BOT. 10 Specifically for those selected patients with posttreatment dysphagia due to an impaired function of the base of the tongue, Kraaijenga et al reported their promising experience with BOT lipofilling in six patients affected by head and neck cancer and with chronic dysphagia secondary to surgery and/or chemoradiotherapy. 5 In 2011, we reported our experience about a patient treated with curative radiation for nasopharyngeal carcinoma and iatrogenic lack of lingual movements. 6 The patient was put under general anaesthesia, and the fat injection was performed transorally along the median lingual raphae under direct endonasal fibre-optic visualization of the base of the tongue. 6 More recently, Ottaviani et al. reported the benefit of BOT lipofilling under local anaesthesia with the patient awake and able to swallow, thus allowing to monitor the effect of surgery in real-time. In their experience, the flexible endoscope was inserted trans-nasally while the functional fat injection was performed using a transcervical thyrohyoid approach. The volume and area were not decided a priori but were related to the desired patient-specific functional loss and intraoperative endoscopic examination. 7 According to our experience, the lipofilling of the BOT under local anaesthesia shows significant advantages, in terms of monitoring the effect of the procedure in real-time with an intraoperative fiberoptic examination of the upper aerodigestive tract and avoiding the effect of gravity on the back fall of the BOT during the procedure. This surgical procedure has proved to be effective and safe; thus, it fulfils to authors’ concern about an augmented intubation risk under general anaesthesia due to the anatomical alteration of the natural airway or oedema from chemo-radiation, and the necessity of a protective tracheotomy or nasotracheal intubation. Moreover we can assume that, avoiding the transoral approach and the potential translocation of bacterial flora from the oral cavity, the transcervical approach reduces the possibility of surgical site’s infection. We didn’t record any major postoperative complication. We used a median avascular plane at the level of the lingual raphae, thus avoiding trauma to the lingual artery. In the case reported by Ottaviani et al., the injection point was at the level of the thyrohyoid juncture in a patient treated with a horizontal supraglottic laryngectomy. 7 In our experience, the submental area provides a wider range of inclinations, thus permitting to reach more sites of the base of the tongue with a homogeneous distribution of the injected fat. Furthermore, this is a repeatable technique that might be used for all type of open partial laryngectomies, including type IIa and IIb, where the thyroid-hyoid space has been removed. 7 To note, this is the first paper that describe a step-by-step injection’s method in three patients for whom the area and angles of injection were patient-tailored on the base of the anatomical characteristics at the preoperative CT scan. One of the main limits of this technique and others reported in Literature is the unpredictable rate of fat reabsorption, which has been reported to range from 20 to 90%. 11 In our experience, the minimum volume of injection for an effective volumetric gain was about 24 ml. We do not advocate for a smaller amount of fat, but this datum will be verified in further comparative clinical studies on a larger cohort of patients.
The submental lipofilling of the BOT showed to be feasible and reproducible in all three cases. The study of the preoperative CT scan allows to define standard anatomical landmarks that help the surgeon to perform an homogeneous injection of the fat empowered by the visual endoscopic control of the base of the tongue in real-time.
This study offers a potentially reproducible technique based on the evaluation of patients’ specific anatomical landmarks. Further prospective studies on a larger cohort of patients will follow in order to highlight the potential limits, drawbacks and field of application of this technique and eventually standardize the procedure.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by the Italian Ministry of Health with Ricerca Corrente and 5x1000 funds.