
Abstract
Introduction
According to the World Health Organization, more than 466 million people suffer from hearing loss, of which, 34 million are children and 10–19% of pediatric cases have cochlear nerve deficiency (CND). 1 CND refers to a small or absent cochlear nerve on high-resolution imaging, accompanied by normal or abnormal morphology of the inner ear and stenosis of the internal auditory canal or cochlear nerve canal with/without the electrophysiological characteristics of auditory neuropathy.2-4 In recent years, high-resolution magnetic resonance imaging (MRI) has been used to observe the neuromorphology and development of the internal auditory canal, showing that CND accounted for 6–28% of those with auditory neuropathy spectrum disorder. 5 It is believed that CND may be associated with the pathological site, acting as one of the causes of auditory neuropathy spectrum disorder (ANSD). 6 This study of 25 pediatric cases of CND involved a detailed medical history investigation, systematic audiology examination, and genetic testing to retrospectively analyze their audiological and imaging characteristics, as well as to explore appropriate early intervention measures.
Methods
Subjects
A total of 563 children with an unpassed automatic auditory brainstem response (AABR) were diagnosed with hearing loss in our department from December 2018 to December 2021. Among them, 25 children (25/563, 4.4%) aged from 2 months to 5 years (average age is 1.78 years) were diagnosed as CND, including 13 boys and 12 girls. None of the 25 children had a family history of hearing loss. The mother of one child with bilateral inner ear malformation and bilateral CND had an upper respiratory tract infection and fever in early pregnancy. Another case of bilateral CND with inner ear malformation was born with an intestinal obstruction and was physically retarded. Moreover, the mothers of four children with unilateral deafness had upper respiratory tract infection during pregnancy. This study was approved by the Ethics Committee of Children’s Hospital of Fudan University and conducted per ICH guidelines for Good Clinical Practice and the Declaration of Helsinki.
Computed tomography (CT) of the temporal bone and magnetic resonance (MRI) of the internal auditory canal
CT of the temporal bone and MRI of the internal auditory canal were performed in the 26 CND children, with children sedated with chloral hydrate half an hour before the examination if necessary. The CT was performed by a GE Light Speed VCT with the following scanning parameters: 120 kV, 120 mA, 5 mm spacing, 5 mm collimation, 512×512 matrix, 5 mm thick section, 0.625 increment, and the images of the coronal axis were rebuilt. The MRI was performed using the Siemens Magnetom Avanto 1.5 T MRI system with the following parameters of T2WI with fat suppression (axial and coronal): TR = 1200 ms, TE = 67 ms, FOV = 200 × 200 mm, Bandwidth = 41.6 Hz, turn Angle=150°, NEX = 2, layer thickness = 0.3 mm, and Matrix = 320 × 320. Sagittal T2FRFSE fat suppression scans were performed on both ears of each child and the parameters were set as follows: TR = 5000 ms, TE = 79.7 ms, FOV 200 × 200 mm, bandwidth 41.6 Hz, NEX = 2, layer number = 19, and layer thickness = 0.3 mm.
A CND diagnosis was made if one of the following criteria was met: 1) CT of the temporal bone showed that the diameter of the narrowest cross-section of the bony internal auditory canal was less than 2 mm, 7 2) CT of the temporal bone showed cochlear neural tube stenosis (cross-sectional diameter less than 1.5 mm) or undeveloped cochlear neural tube, 7 3) MRI at the midpoint of the internal auditory canal showed that the diameter of the cochlear nerve was smaller than that of the facial nerve, 4) MRI of the internal auditory canal showed no auditory nerve in any cross-section, 8 or 5) the diameter of the vestibular cochlear nerve at the cerebellar pontine angle was less than 1.5 mm or 1.5 times that of the facial nerve. 9
Audiological detection
The auditory brainstem response (ABR) and auditory steady-state response (ASSR) were measured with a GSI Audera Brain-stem Analyzer using a Modle TIP-50 earphone, with silver disc electrodes placed on the participants’ scalps in the following positions: nasion (ground electrode), forehead (active electrode), and mastoid (reference electrode). For ABR, the bandpass filter settings were 30 and 5000 Hz with a 10-msec window, and the average response was obtained twice by recording the response to two series of 2,006 clicks, as detailed previously. 10 The CM response appeared between the presence of a regular ABR waveform and the click stimulus and inverted with stimulus polarity reversal, whereas neural responses to clicks typically did not completely invert. 11 For ASSR, dichotic stimulation and multiple frequencies were used, and the following carrier frequencies were used: 500, 1000, 2000, and 4000 Hz.
Behavioral audiometry was measured by pure tone audiometry (PTA). Children aged >4 years wore headphones for PTA, with pure or warble stimulus sounds and frequencies of 0.5, 1, 2, and 4 kHz, as described previously. 12 Acoustic immittance was used to assess the middle ear function, and distortion product otoacoustic emission (DPOAE) was used to investigate cochlear mechanics.
Genetic testing
DNA was extracted from whole blood samples and purified using a commercially available extraction kit (Qiagen Inc. China). Genetic testing was performed in 8 patients via second-generation sequencing.
Results
Audiological features of CND
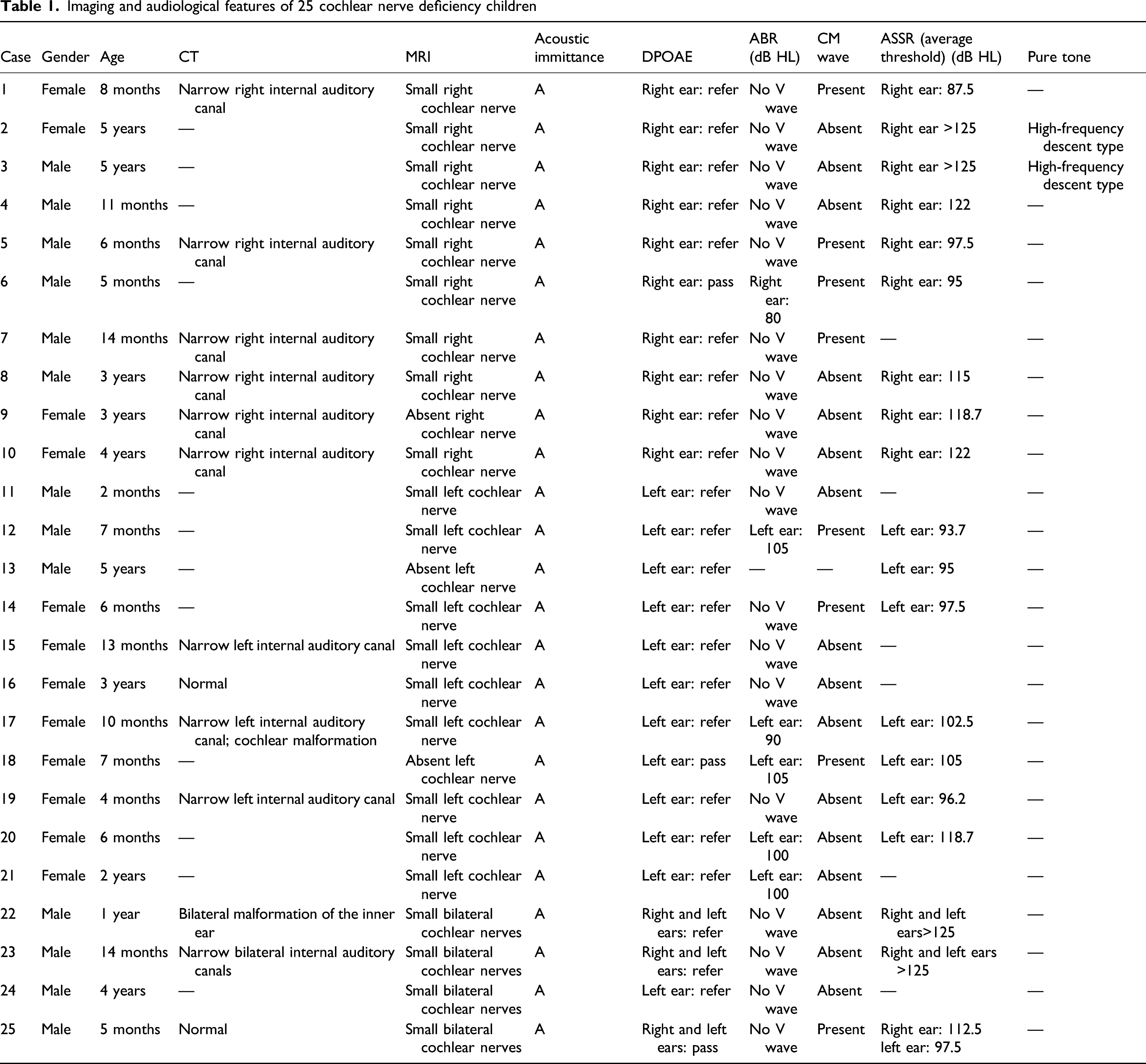
Three children passed the otoacoustic emission, and eight children had a cochlear microphonic (CM) wave Figure 1, suggesting audiological characteristics of ANSD. All ears had a type A tympanogram, and the ABR suggested that the auditory threshold of the deaf ears was greater than 100 dB HL. Pure tone audiometry was recorded in 2 cases, both of which were extremely severe sensorineural hearing loss. The multiple auditory steady-state responses showed that the average hearing threshold of deaf ears in children with CM waves was significantly higher (P < 0.001) than those in children without CM waves. Language development was normal in two older children with unilateral deafness, but the speech recognition rate of the deaf ear was poor. Children with (A) or without (B) CM waves.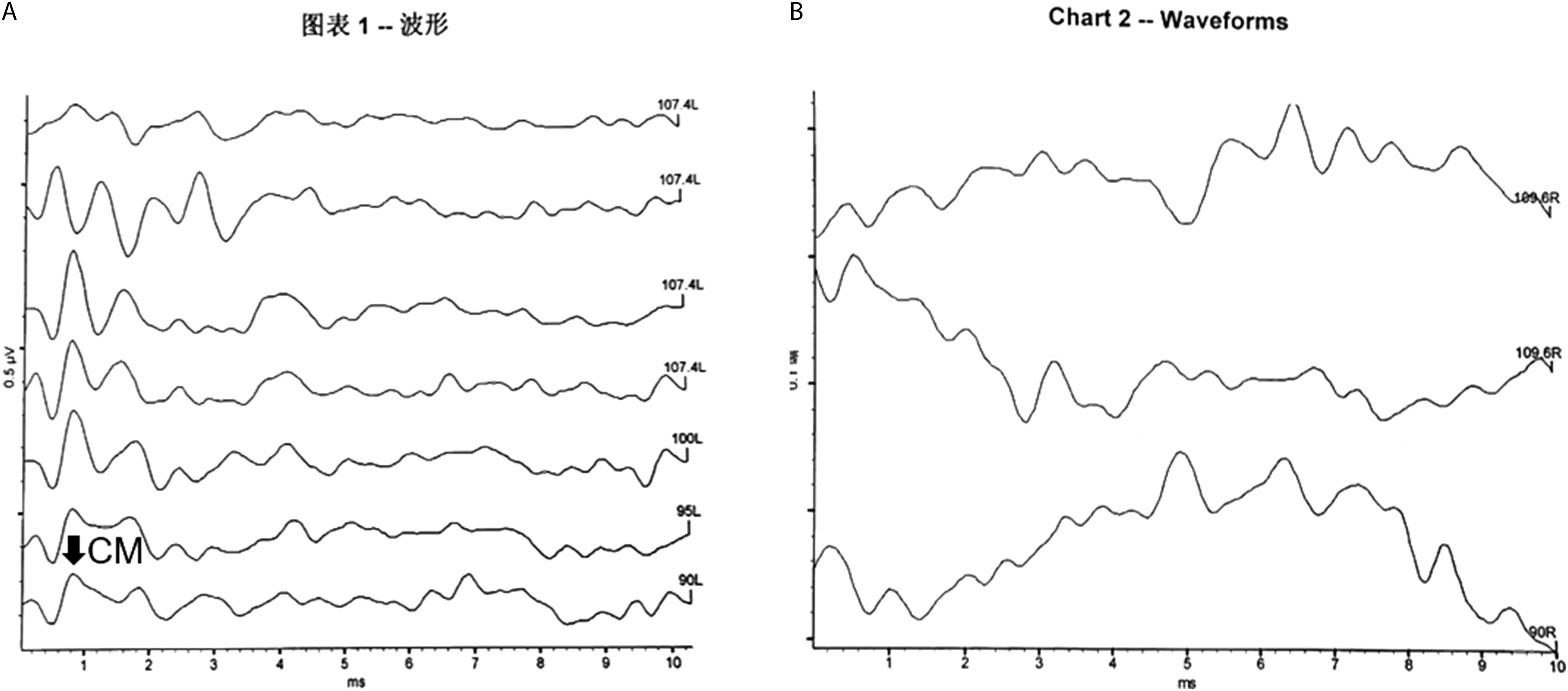
CT and MRI features of CND
CT abnormalities were found in 11 children (11/13, 84.6%), and since acoustic nerve abnormalities cannot be completely ruled out by CT, MRI was performed to better display the auditory nerve of the internal auditory canal. The typical MRI feature of CND is shown in Figure 2. Nineteen children (19/25, 76.0%) presented with unilateral CND (10 children with right CND and 11 children with left CND), and 4 children (4/25, 16.0%) presented with bilateral inner ear malformations and bilateral CND, indicating that most CND were unilateral (Table 1). MRI features of the cochlear nerve deficiency (A) and normal (B) internal auditory canal. (A) The facial nerve (Fn) and vestibular superior nerve (Vsn) can be seen in the inner auditory canal, but the cochlear nerve (Cn) and vestibular inferior nerve (Vin) are absent. (B) Normal MRI features of the internal auditory canal. The facial nerve (Fn), vestibular superior nerve (Vsn), cochlear never (Cn), and vestibular inferior nerve (Vin) can be seen in the internal auditory canal. Imaging and audiological features of 25 cochlear nerve deficiency children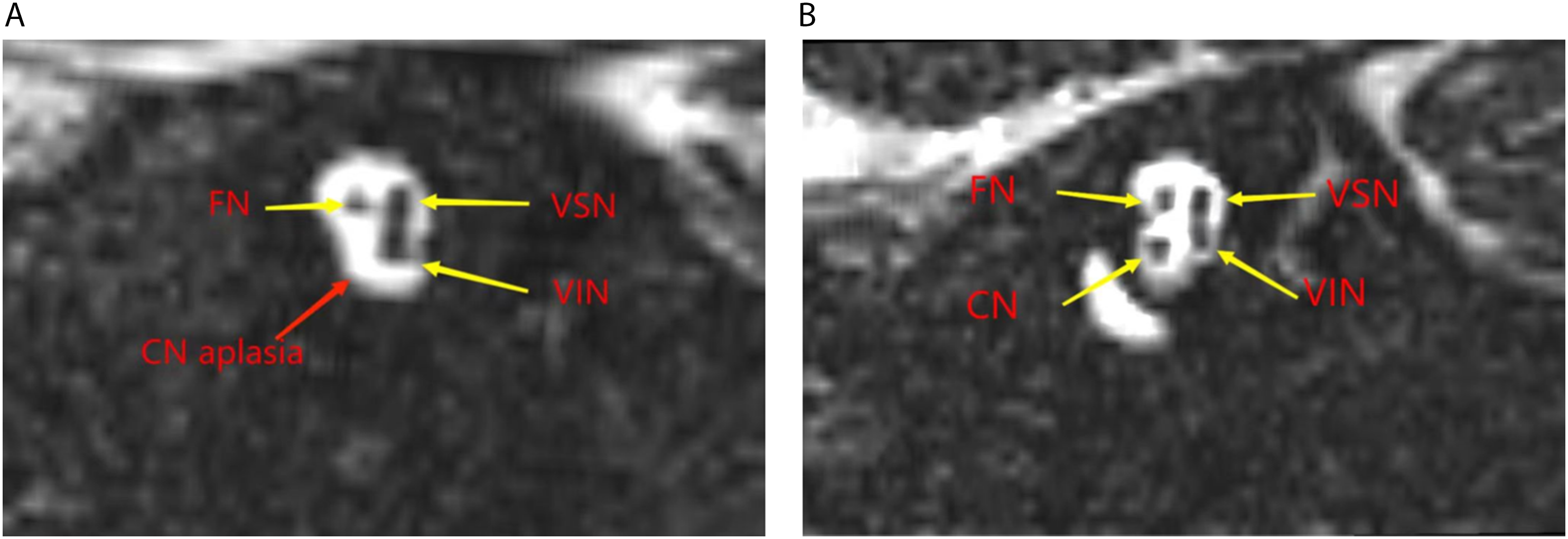
Genetic testing
No deafness-related mutations were detected via second-generation sequencing.
Discussion
During the first three weeks of embryonic development, a group of neural crest cells appears in the open dorsolateral area of the rhombencephalon and the rostral side of the otic placodes, giving rise to both the facial and cochlear nerves, known as the origin base or crest of the facial-acoustic nerve. One week later, the otic placodes gradually invaginate to finally form the otic vesicle of the membranous labyrinth of the inner ear, and the cochlear nerve arises from the origin base terminating on the wall of the otic vesicles. At the same time, the otic ganglion is divided into upper and lower parts, with the upper part developing into vestibular ganglion while the lower part further develops into the upper and lower branches, forming the inferior vestibular nerve and the cochlear spiral ganglion, respectively. During the 7th week, fibers from the spiral ganglion form the cochlear nerve, while the vestibular ganglion develops and forms the superior vestibular nerve. The concept of CND was first proposed by House in 1989, which refers to the absence of and/or small cochlear branch of the vestibulocochlear nerves (cranial nerve VIII), 13 including both cochlear nerve aplasia (CNA) and cochlear nerve hypoplasia (CNH). 14 Nowadays, the pathogenesis of CND remains unclear and can occur alone or in combination with other malformations of the inner ear. In this study, CND in most cases was unilateral (76%), especially in the right ear. There were also two bilateral CND cases accompanied by inner ear malformations, which may result from the arrested development during the early embryonic development in the synchronized growth of the cochlear structure and cochlear nerve. The children in this study were diagnosed early, once they failed hearing screening at birth, therefore all were considered as congenital CND. Except for a small or absent cochlear nerve, the development of the middle ear and inner ear was normal in the unilateral CND cases, with inner ear malformations in the bilateral CND cases. No other neurodevelopmental abnormalities were observed in these children in addition to CND.
CND was found in 10–19% of the patients with congenital sensorineural hearing loss, 1 and Valero et al. 5 reported that the incidence of CND in patients with ANSD was 6–28%. Therefore, routine MRI of the internal auditory canal is recommended for children with congenital unilateral hearing loss, as Clemments reported 26% cases in children with SNHL. In our study, CT abnormalities were found in 11 children (11/13, 84.6%); however, acoustic nerve abnormalities cannot be completely ruled out by CT, so an MRI examination was performed to better display the auditory nerve of the internal auditory canal.
CND can be seen in children with normal external hair cells and is regarded as the pathological site and one cause of ANSD. Patients may show the characteristics of auditory neuropathy, that is, seriously abnormal ABR with CM present or DPOAE pass. In our study, a CM wave or DPOAE pass was recorded in 11 of the 25 CND cases by auditory brainstem response testing, suggesting 44% (11/25) of the CND cases presented with audiological characteristics of ANSD. In addition, dysfunction of cochlear outer hair cells was found in most CND cases, with only a few with normal cochlear inner hair cells.
Audiological examination showed extremely bad differentiation of ABR waveforms of all ears, with no obvious wave Ⅲ and wave V. A CM wave was recorded in eight ears presenting the audiological features of ANSD. Notably, multi-frequency steady-state response test revealed that the average hearing threshold of the ears with a CM wave was significantly higher than that of the other ears (P < 0.001), indicating that the function of cochlea inner hair cells in these ears was normal and their cochlear nerve still had residual function, which, unfortunately, cannot be verified in unilateral CND as most of these children were too young to cooperate with subjective tests. Besides, extremely severe sensorineural hearing loss was found in two older children by pure tone audiometry, with a declining trend at high frequency in the audiometric curve. Based on their condition of unilateral CND, no special intervention was taken as their functions of speech and language were normal, with only poor speech recognition in the ear with CND.
According to the MRI and CT results, the anatomical characteristics of the auditory nerve in children with CND can be largely understood, but the functions of the auditory nerve in these children remain unclear. Theoretically, the auditory nerve encodes the electrical stimulation delivered by the cochlear implants, which is then transmitted to and processed by more developed neural structures. The electrical stimulation with cochlear implants (CI) electrode in the cochlea may not reach the brainstem and auditory cortex in patients with cochlear nerve aplasia 15 ; therefore, patients with auditory nerve loss may not benefit from cochlear implantation. However, studies have demonstrated that CND is not an absolute contraindication to CI due to the limitations surrounding the resolution of MRI and the detection threshold in CND, and the response of the auditory cortex to acoustic stimulation was identified even though the cochlear nerve was absent on MR images. 16 This study found residual hearing in some children with CND, especially those presenting with CM waves in ABR.
In conclusion, CND can be accompanied by other inner ear malformations. MRI should be performed in children with unilateral deafness to exclude CND, and CND should be considered in children with no abnormal CT results; the CM wave or DPOAE pass should be recorded in CND children presenting with the characteristics of auditory neuropathy. The postoperative effect of cochlear implantation is not dependent on the absence of the cochlear nerve in preoperative imaging examinations, with residual hearing found in some children with CND. Some children with unilateral deafness may have normal functions of speech and language even no special intervention was taken due to the normal hearing of the contralateral ear.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Young Clinical Scientist Project (2022LCKXJ03).