
Abstract
Objective
Current management of fibrous dysplasia (FD) involving the paranasal sinuses and the adjacent skull base is currently controversial. This study aims to present our experience in the management strategy of FD that involves the paranasal sinuses and the adjacent skull base.
Methods
Twenty three patients from 2006 to 2019 with monostotic fibrous dysplasia (MFD), polyostotic fibrous dysplasia (PFD), or McCune-Albright syndrome (MAS) involving the paranasal sinuses and the adjacent skull base were retrospectively reviewed. This study series was divided into 3 groups based on management strategies: the observation group, the surgery group, and the optic nerve decompression group.
Results
The observation group included 9 patients with asymptomatic MFD with stable condition during the follow-up period of 15 to 164 months. The surgery group included 10 symptomatic patients with MFD who had personalized endoscopic endonasal surgery. The symptoms of the patients were relieved after surgery. The optic nerve decompression group included 4 patients with visual loss, who underwent endonasal endoscopic optic nerve decompression (EOND) with the aid of image-guided navigation. Their vision improved after surgery.
Conclusions
Clinical observation and periodic computed tomography (CT) scan are adopted for asymptomatic patients. Surgery is indicated in symptomatic patients. Optic nerve decompression is recommended as soon as possible if the patient has visual loss, whereas prophylactic decompression is not recommended if the optic nerve is encroached by FD without visual loss. Navigation plays an important role in endoscopic surgery involving the paranasal sinuses and the adjacent skull base, especially in FD resection and optic nerve decompression.
Keywords
Key Points
Clinical observation is adopted for asymptomatic patients. Surgery is indicated in symptomatic patients. Navigation plays an important role in endoscopic surgery in FD resection and decompression of the optic nerve.
Introduction
Fibrous dysplasia (FD) of bone, also known as fibrous hyperplasia of bone, is a group of non-neoplastic diseases with fibro-osseous bone lesions. Fibrous dysplasia is a developmental disorder induced by abnormal proliferation of fibroblasts resulting in the replacement of normal cancellous bone by structurally immature osseous tissue.1-3 Fibrous dysplasia can affect any bone of the body and affect one or more bones. It is divided into 3 types: monostotic FD (MFD), polyostotic FD (PFD), and McCune-Albright syndrome (MAS). When the lesion involves the craniofacial skeleton, the skull base is the most common site of involvement.1-3
Due to the low incidence rate, diverse natural history, and complicated surgical procedure, the management of FD involving the paranasal sinuses and the adjacent skull base is controversial. Therefore, many scholars have called for the development of a global consensus on improving patient management.4-7 In this study, we show our experience and treatment strategies for the management of 23 cases of FD that involved the paranasal sinuses and the adjacent skull base.
Patients and Methods
Subjects
Clinical Data of Patients in the Observation Group.
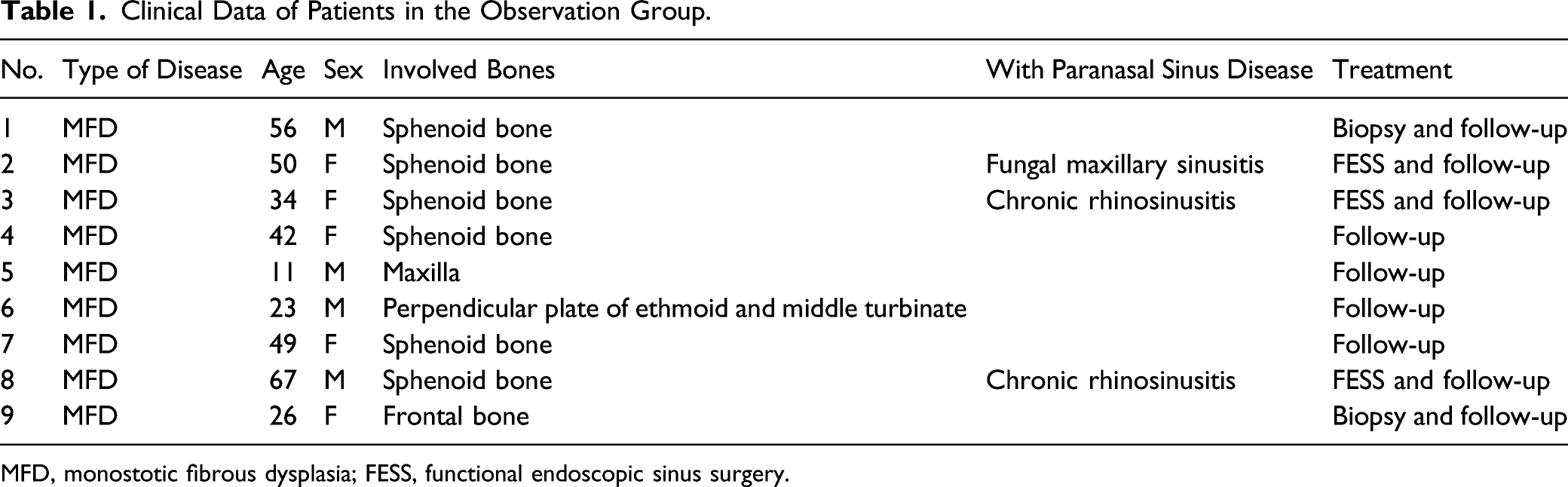
MFD, monostotic fibrous dysplasia; FESS, functional endoscopic sinus surgery.
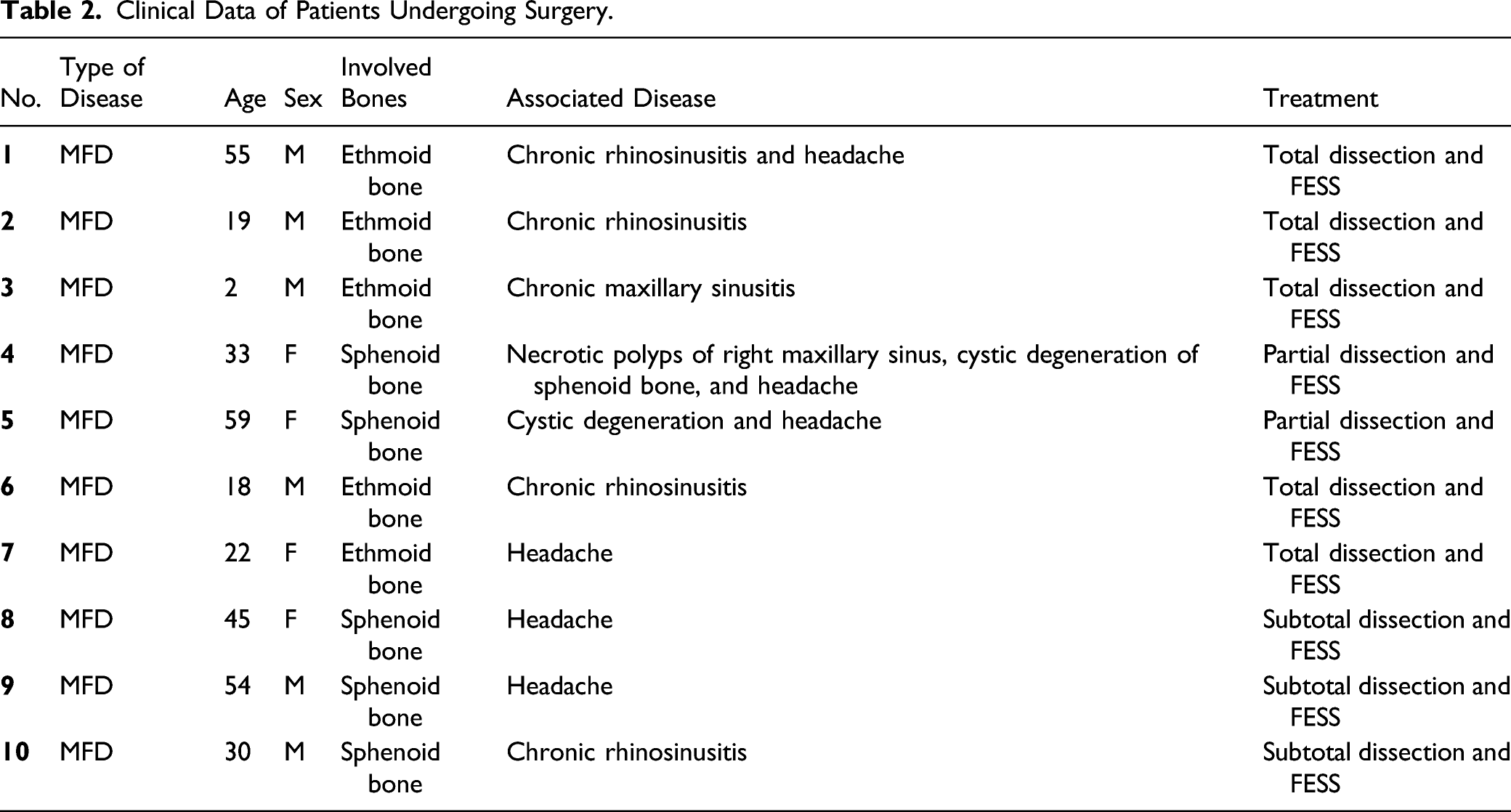
Clinical Data of Patients Undergoing Surgery.
Clinical data of Patients Receiving Endoscopic Optical Nerve Decompression.
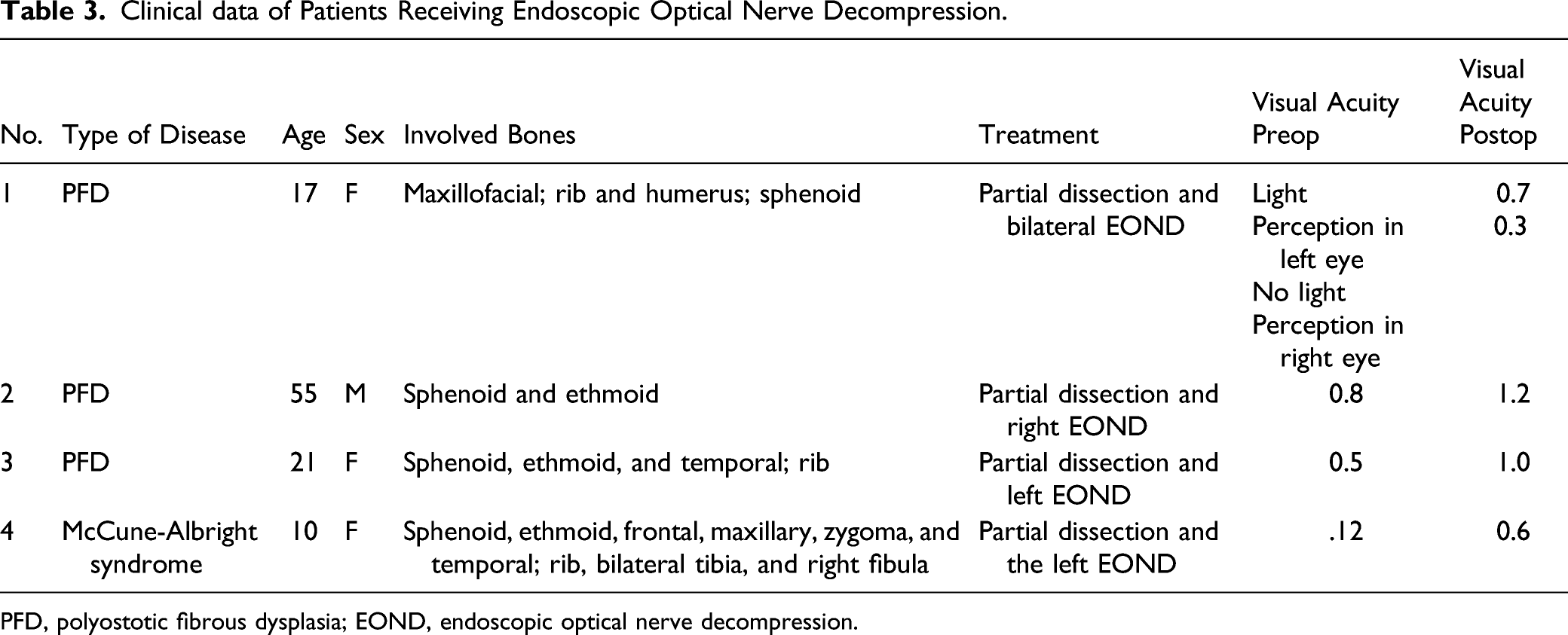
PFD, polyostotic fibrous dysplasia; EOND, endoscopic optical nerve decompression.
This study was approved by the Ethics Committee of our hospital and was conducted with written informed consent from the patient.
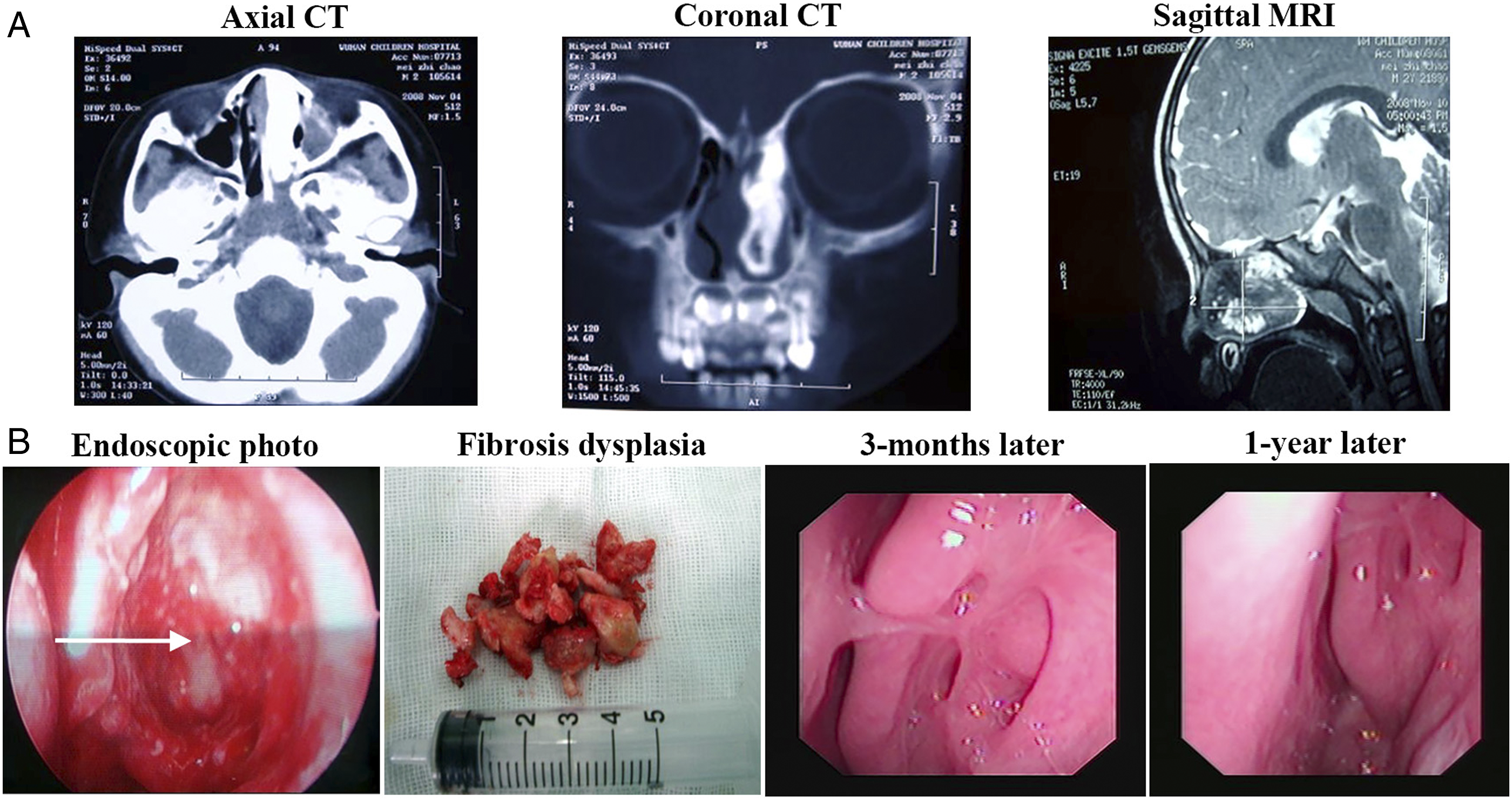
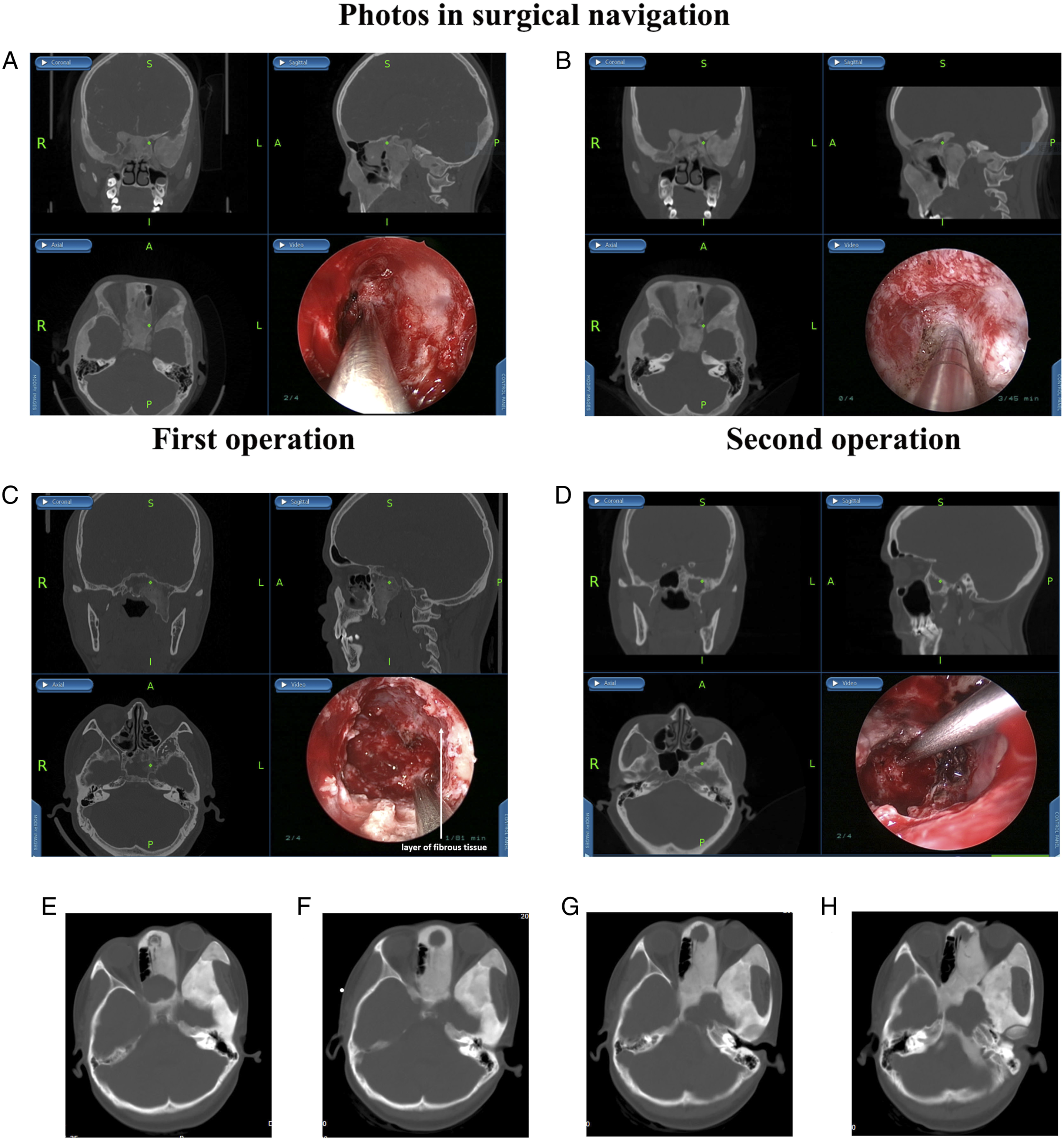
All patients received a thin-section computed tomography (CT) scan of the paranasal sinuses, including coronal and axial views. The CT revealed the location of the lesion and was helpful for diagnosis. The most common findings of FD in CT are an expanded bone with a ground glass appearance. The bone window showed that the image of a normal bone structure was replaced by the image of a high-density ivory pattern (Figure 1), a low-density pattern (Figure 2), or a frosted glass pattern (Figures 3A and 3B). Imaging features of fibrous dysplasia located in the sphenoid bone in a 56-year-old patient (patient 1 in Table 1) in different dimensional CT scans (A). Because of no symptoms, the patient accepted a biopsy, which was identified as fibrous dysplasia. The patient was followed up until now. The image shows the nasal cavity and sinus of the patient 8 years after the biopsy (B). (CT, computed tomography). Imaging features of a 2-years-old patient (patient 3 in Table 2). The images show the axial and coronal views of CT scans and the sagittal view of the MRI of the paranasal sinuses before the operation (A). The removal of a fibrosis dysplasia lesion in the ethmoid bone under FESS (B). The mass removed from the ethmoid bone in the operation was confirmed to be fibrosis dysplasia by pathological examination (B). The photos under nasal endoscopy showed the nasal cavity after the endonasal endoscopic operation 3 months later and 1 year later, respectively (B). The white arrow shows the place of the removed lesion in the ethmoid bone. (MFD, monostotic fibrous dysplasia; CT, computed tomography; MRI, magnetic resonance imaging; FESS, functional endoscopic sinus surgery). Imaging features of MAS in a 10-year-old patient (patient 4 in Table 3) (Figure 3A and 3B). Images used during the navigation-assisted operation: sagittal, coronal, and axial scans, and the video (The first and the second operation: 3A and 3B). The patient received left optic nerve decompression using an endoscopic endonasal approach. Then the patient received left optic nerve decompression again one and a half years later because of her left visual loss again. The green dot shows the left orbital apex region (A, B). Figure 3C showed the images used to aid image-guided navigation in MFD endoscopic sinus surgery (patient 9 in Table 2). The white arrow shows the thin layer of fibrous tissue between the fibrous dysplasia lesions and the sphenoid bone (C). Figure 3D showed the imaging features of fibrous dysplasia with degeneration changes (patient 5 in Table 2). The paranasal sinus CT of MFD showed frosted glass changes of the left sphenoid pterygoid process and the great wing, with a 2.3 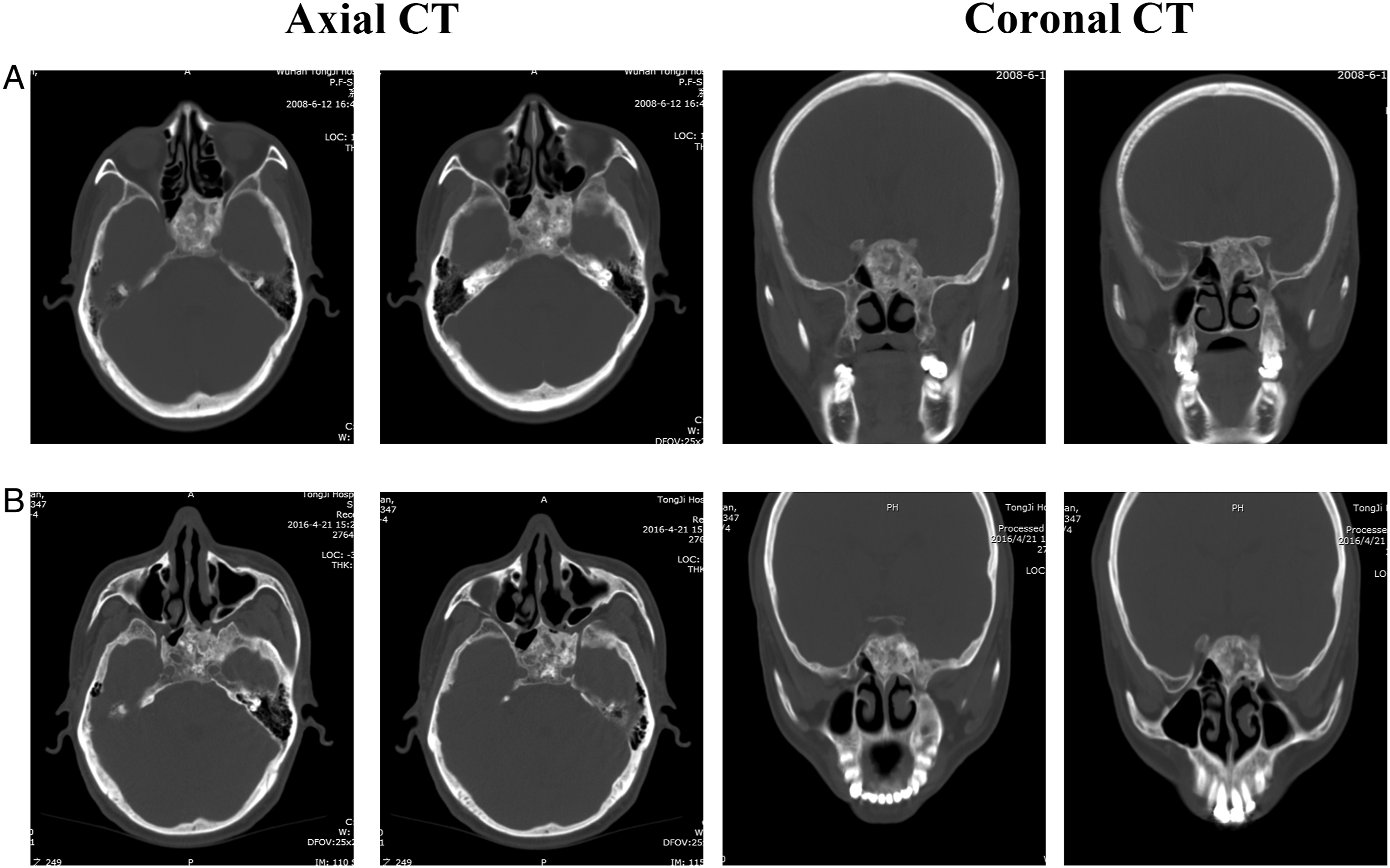
Management Strategies
This study series was divided into 3 groups based on management strategies, namely, the observation group, the surgery group, and the optic nerve decompression group.
The observation group included 9 patients with asymptomatic MFD and adopted the method of clinical observation and regular follow-up. Patients received a periodic paranasal sinus CT scan. The clinical data are shown in Table 1. Three of the 9 patients had chronic rhinosinusitis, who received functional endoscopic sinus surgery (FESS) only for their chronic rhinosinusitis. The other 6 patients with FD were found on physical examination. Two of them received a biopsy using an endoscopic endonasal approach.
The surgery group included 10 patients with symptomatic MFD. Clinical data are shown in Table 2. Five of the patients underwent FESS for chronic rhinosinusitis simultaneously. The FD was relatively hard and was removed by an electric drill (Medtronic IPC, USA) and Kerrison Rongeurs. Seven of the cases were excised with the aid of image-guided navigation (Fusion, Medtronic ENT, USA) (Figure 3C and 3D).
The optic nerve decompression group included 4 patients with vision loss, who underwent endonasal endoscopic optic nerve decompression (EOND) with the aid of image-guided navigation. Clinical data were shown in Table 3. One of the patients received bilateral endoscopic decompression of the optic nerve simultaneously. The MAS patient accepted the first surgery for left EOND in February 2016 and again in July 2017 (Figure 3A and 3B).
Results
The patients in the observation group were regularly followed. For example, in case 1 in Table 1, the paranasal sinus CT scan in June 2008 showed FD of ivory high-density sphenoid bone, then the patient received endonasal endoscopic biopsy and was diagnosed as FD by histopathological examination. He was asymptomatic and was followed up regularly. The paranasal sinus CT taken in 2008 was compared with the paranasal sinus CT reviewed in 2016, which revealed that the FD was in a static state (Figure 1).
In the surgery group, 5 patients with FD of the ethmoid bone underwent total resection, while 3 patients with FD of the sphenoid bone underwent subtotal resection and 2 patients underwent partial resection using an endonasal endoscopic approach. Five of the patients underwent FESS for chronic rhinosinusitis simultaneously. The symptoms of the patients were relieved after surgery and there were no intracranial or intraorbital complications. The patients in this group were followed for 1–13 years and there was no recurrence.
During the operation, we found that although some MFD lesions were large, neither the germinal center nor the pedicle was large. A thin layer of fibrous tissue separated FD from normal bone, and it was relatively safe to dissect along this layer of fibrous tissue. For example, case 3 in Table 2 is a two-year-old boy. The paranasal sinus CT scan of the patients showed that the left ethmoid sinus and nasal cavity were filled with a large (40.5 mm × 6.3 mm × 29.9 mm) and highly dense mass (Figure 2). The mass originated from the left cribriform plate, compressed the left papyracea lamina, and extended to the bottom of the nasal cavity. The frontal sinuses and sphenoid sinuses were not developed. The thin layer of fibrous tissue was found between the FD and the partial cribriform plate and the papyracea lamina during surgery (Figure 2). This phenomenon was also observed in the resection of FD of the sphenoid bone (Figure 3C).
In addition, MFD can have degenerative changes with age, as shown in case 4 and case 5 (Figure 3D) in Table 2. Paranasal sinus CT of case 5 revealed frosted glass changes of the left sphenoid pterygoid process and the great wing, with a 2.3
In the optic nerve decompression group, the effects of optic nerve decompression are shown in Table 3. The youngest patient in this group, a 10-year-old girl with MAS, showed left visual loss again one and half years after her first left optic nerve decompression. The patient received left optic nerve decompression again and the left visual acuity remained stable until now. However, CT showed that the right optic nerve was covered with FD, but the patient’s right eye vision remained stable all the time (Figure 3A and 3B). Case 1 in Table 3 underwent bilateral optic nerve decompression due to cystic degeneration of the FD (Figure 3E). The CT 2 years before surgery revealed that the left optic nerve was completely enclosed and the right optic nerve was partially enclosed by FD (Figure 3F, 3G, 3H), but vision was normal until 1 month before surgery.
During the follow-up period, the 9 patients with asymptomatic MFD included in the observation group are still in stable condition during the follow-up period of 15 to 164 months, including the boy of 11 years. He does not have a maxillofacial face deformity and is still followed. The paranasal sinus CT was taken at the local hospital. Patients with FD of the sphenoid bone in the observation group in this series did not progress to oppressive optic neuropathy, such that there has been no need for surgery during the follow-up period to date. The patient with frontal bone FD is still in stable condition and had no headache or other symptoms. The patient with FD of the perpendicular plate of the ethmoid and middle turbinate is still asymptomatic. The patients undergoing surgery did not have recurrence during follow-up. There was no further loss of vision for patients receiving EOND.
Discussion
In view of the rarity, complex, and varied natural history, and clinical manifestation of FD, it is difficult for clinicians to develop a standardized treatment plan. As a consequence, there are no treatment guidelines that currently exist. 1 Although there was no international guideline for the management of FD/MAS, an international workshop has been set up to focus on improving FD/MAS management and understanding the importance of a multidisciplinary team for the lifetime management of FD/MAS. 7
Fibrous dysplasia treatment includes clinical observation, medical therapy, and surgery. Medical treatment for FD is limited to relieving symptoms in a patient. One of these medications is bisphosphonate, which may help improve function, relieve pain, and reduce the risk of fracture. However, a recent randomized, double-blind, placebo-controlled trial disputed these effects.8,9 Radiation therapy is contraindicated due to the high prevalence of malignant transformation. Therefore, clinical observation and surgery are currently the main treatment strategies for FD.
Clinical observation is adopted for patients with asymptomatic FD, but patients should be required to have periodic radiological evaluations. As FD is a slow-growing lesion, tends to be stable after puberty, and has a low potential for malignancy, most specialists recommend clinical observation if there are no symptoms, but periodic imaging should be performed to confirm that there is no progression or regrowth in follow-up. 1 Comparing craniofacial FD management between 1980 and 2002 with management between 2003 and 2013 showed that observation has replaced surgery as the most widely used method. Watching carefully and attentively was indicated in cases of stable lesions and was the best therapeutic option, if possible. 4 In France, with the establishment of national reference centers, 57 specific recommendations have been provided for the diagnosis, prognosis, and follow-up of patients with FD/MAS. If the skull and/or facial bones are involved, a skull CT is recommended to accurately evaluate the risk of neurological compromise due to alterations in the foramina. Magnetic resonance imaging (MRI) should be viewed as a second-line imaging study. Radiographic monitoring is recommended every 2–3 years for follow-up patients. 10 It was shown that the characteristics of FD on CT and the natural radiographic progression can vary from a “ground glass” or homogeneous appearance to a mixed radio-dense/radio-lucent lesion as the patient ages. 2 According to preoperative radiology, the sensitivity and specificity to correctly detect FD were 54.6% and 96.9%, respectively.
Lesions with a classic pattern of ground glass or mixed CT pattern should not warrant diagnostic biopsy, especially in asymptomatic patients. However, if the radiological diagnosis is uncertain, biopsy may be warranted to arrive at the definitive diagnosis based on radiographic and histologic correlation. 11 Biopsy of a lesion does not specifically induce the growth of FD, but if the lesion is asymptomatic and/or at the cranial base, a biopsy may not be necessary. 2
Surgery is indicated in symptomatic patients. Although the application of surgical treatment for craniofacial FD is controversial, many publications have provided views on the surgical treatment of FD.12-14 Comparing craniofacial FD management between 1980 and 2002 with management between 2003 and 2013 revealed that radical resection (if possible) of FD was the only technique to obtain resolution of the disease. 4 The advantages of surgical treatment of FD should be adequately weighed against possible complications. 1 The purpose of surgical treatment for craniofacial FD is to remove the bulk of the lesion, preserve the compression of the cranial nerve, and resolve the esthetic problem. 6 The extent of the resection should be based on the location of the pathological bone and its proximity to important structures as radical or complete resection may not be necessary or possible. 5 Treatment protocols should be customized to the individual patient’s needs, with the aim of achieving the best possible esthetic and functional outcome with the least postoperative morbidity.12,15 Therefore, surgical treatment planning must take into account several factors (i.e., natural history of the disease, presence of symptoms, site of the lesion, and relationship with critical anatomic structures). 1
Early surgery is necessary for the patient with MFD when the lesion was limited to the ethmoid or sphenoid bone with obvious symptoms. It is because the growth and expansion of FD may lead to obstruction of the sinus ostia and result in rhinosinusitis and mucocele. Furthermore, the lesion has been reported to affect adjacent bone, such as the lamina papyracea and the anterior skull base, extend into the orbit and intracranial cavity, and ultimately lead to epiphora, diplopia, proptosis, impaired visual acuity, meningitis, leakage of cerebrospinal fluid leak, and so on. 16 Five patients with ethmoid bone FD and three with sphenoid bone FD in the surgery group of this study series underwent total resection or subtotal resection through an endonasal endoscopic approach, respectively. Only two patients with sphenoid bone FD underwent partial resection using an endonasal endoscopic approach. And five patients in the surgery group underwent FESS for their chronic rhinosinusitis simultaneously. Meanwhile, what we found in these procedures was that in the expansion process of FD toward the cavity of a paranasal sinus, the epithelial tissue in the sinus cavity can be compressed into a thin layer of fibrous tissue, which separates FD from normal bone, and it was relatively safe to dissect along this layer of fibrous tissue. Combined with the use of intraoperative image-guided navigation and advanced surgical instruments, these surgeries were successfully performed without intracranial or intraorbital complications.
For FD patients with impaired vision, it was recommended to have optical nerve decompression as soon as possible. However, if FD invaded the optic nerve without impaired vision, prophylactic decompression is not recommended. This is the current consensus.1,17–19 A retrospective analysis in 91 patients with craniofacial FD involving optic nerves showed that 17% of nerves were less than 50% encased, 22% were 50–99% encased, and 61% were 100% encased. However, optic nerve decompressions were performed in only 13 patients (6 prophylactic and 7 therapeutic) since the authors regarded that the majority of optic nerves encased with FD did not present symptoms of optic neuropathy and appeared to be stable over time. 17 Satoh K et al. held that current strategies should focus on esthetic improvement, with careful observation carried out to assess optic canal encroachment without prophylactic decompression. 18 In another study, in asymptomatic patients, stable vision occurred in 76% of patients who received decompression and 95% of patients who did not undergo surgery (P < .001). Vision impairment may be associated with the concomitant presence of cystic lesions (i.e., mucocele, hemorrhage, and aneurysmal bone cyst). 19 Holl et al. reported a case of FD in which the patient developed an aneurysmal bone cyst that led to compression of the left optic nerve with acute visual loss. An emergency optic nerve decompression resulted in complete restoration of vision. 20 In this study, a patient had acute bilateral visual loss due to cystic degeneration formation. Another patient with MAS underwent left optic nerve decompression twice, but in fact, although CT showed that the right optic nerve was encased by FD, the right eye vision of the patient remained stable all the time.
Navigation plays an important role in paranasal sinus and adjacent skull base FD resection, and in optic nerve decompression. Stereotactic navigation was recommended as the FD/MAS process often distorted the normal intranasal landmarks used in sinus surgery. 5 Navigation-assisted endonasal EOND was generally effective for the treatment of nontraumatic optic neuropathy. 21 Our study demonstrated that clinical observation is adopted for asymptomatic patients with FD, but patients should be required to undergo periodic radiological evaluations. Surgery is indicated in symptomatic patients. In FD patients with visual changes or vision loss, an optic nerve decompression was recommended as soon as possible; however, if FD is encroaching on the optic nerve without impaired vision, prophylactic decompression is not recommended. We believe that FD does not typically progress after puberty to the point where surgery is necessary, and the condition can thus be observed clinically. Navigation plays an important role in paranasal sinus and adjacent skull base FD resection and optic nerve decompression.
Footnotes
Authors’ Contributions
Shi LL and Zhen HT designed the study. Zhen HT performed the operations and collected the data. Xiong P and Shi LL prepared the manuscript and analyzed the data. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Consent to Participate
This study was approved by the Tongji Hospital Research Ethics Board.