
Abstract
Objective
To propose a modified technique of ossiculoplasty using an ossicle-cartilage composite graft (OCCG) and compare its hearing outcome and protrusion rate with those of a synthetic prosthesis.
Methods
Autologous tragal or homologous septal cartilage was combined with an ossicle to create an umbrella shape OCCG. A total of 302 ossiculoplasty surgeries performed in a single university hospital between 1997 and 2006 were retrospectively reviewed based on the prosthesis type—OCCG or polymaleinate ionomeric prosthesis (IONOS®). Data includes demographic profiles, audiometric outcomes, intraoperative findings, and post-operative complications and was categorized by the follow-up periods.
Results
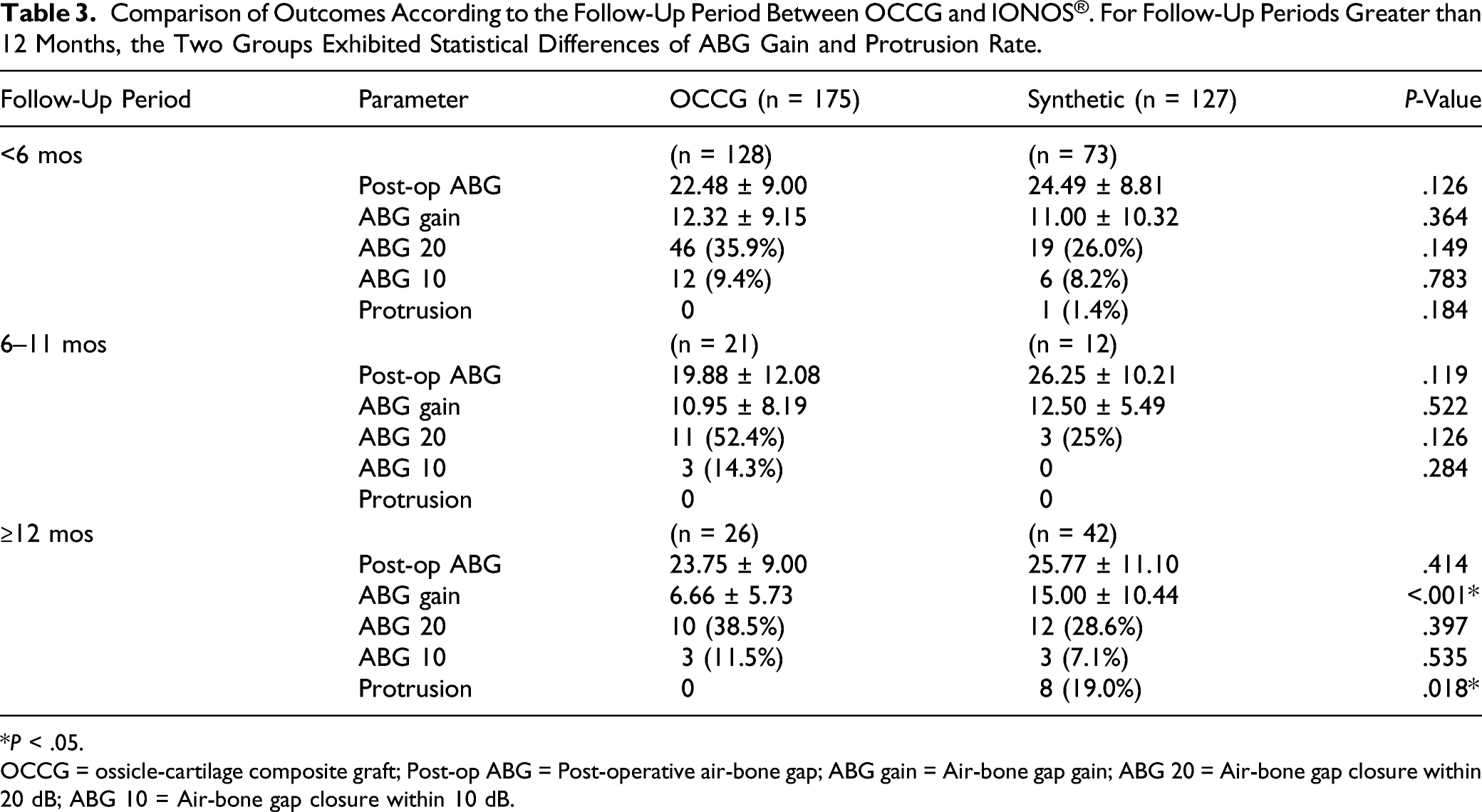
Ossicle-cartilage composite graft was used for 175 patients and IONOS® for 127 patients. The mean post-operative air-bone gap (ABG) of the OCCG group was 22.36 dB, which was better than the IONOS® group of 25.08 dB (P = .015). The successful ABG closure rate of less than 20 dB was also higher in the OCCG group compared to the IONOS® group (38.3% vs 26.8%, P = .036). The ABG between the pre- and post-operative conditions exhibited a significant difference between the 2 groups (P = .006). In the data divided into 3 groups according to the follow-up period, the OCCG group showed a better outcome in the long-term follow-up with 0 cases of protrusion during the follow-up period in the OCCG group compared to 8 cases of the IONOS® group (P = .018).
Conclusion
Ossiculoplasty with OCCG exhibited satisfactory audiometric outcomes and low complication rates. Ossicle-cartilage composite graft can be a good option with sufficient informed consent and preliminary screening of transmitted diseases.
Introduction
Most chronic middle ear diseases involve the ossicular chain, requiring ossicular reconstruction as well as the removal of inflammatory tissue during surgery. 1 Various materials such as autologous ossicles, autologous and homologous cartilage, autologous bone chips, and many synthetic materials are used for ossiculoplasty. 2 Ideal conditions for ossiculoplasty materials include biocompatibility, safety, ease of handling, ease of implantation, and stability for long periods of time.3-5
Ossicular reconstruction using a combination of 2 materials, rather than using ossicle or cartilage alone, has been reported. Malhotra announced an “umbrella” graft for total ossicular replacement prosthesis (TORP) and Kong et al. described a “bone-cartilage composite graft” for total or partial ossicular replacement prosthesis (PORP).6,7 Both groups reported that ossiculoplasty with these composite materials showed satisfactory hearing outcomes and low complication rates.
In this study, we proposed a modified technique of ossiculoplasty using a composite graft of ossicle and the cartilage of nasal septum or tragus, and compare its hearing outcome and protrusion rate with those of a synthetic prosthesis.
Material and Methods
Subjects
Ossiculoplasty surgeries performed in a single university hospital between January 1997 and December 2006 were retrospectively reviewed. All the surgical procedures were performed by one experienced surgeon. Patients diagnosed with chronic otitis media and underwent ossiculoplasty were included in this study. Patients with sensorineural hearing loss, children under 5 years of age, and cases of otosclerosis were excluded. The absence of hearing test after more than a month of surgery was also excluded from this study. Patient data including demographic profiles, pre- and post-operative audiometric results, intraoperative findings, and post-operative complications were collected and compared based on material types. This study was approved by the Institutional Review Board (IRB) of Bucheon St. Mary’s Hospital, the Catholic University of Korea (IRB approval no., HC20RASI0051).
Surgical Techniques
A routine post-auricular approach was used in all the cases. Ossiculoplasties were performed using either ossicle-cartilage composite grafts (OCCG) or synthetic materials. Ossiculoplasty using OCCG was performed in cases of available incus remained, and polymaleinate ionomeric prosthesis (IONOS®) was used if incus was not available due to necrosis or destruction.
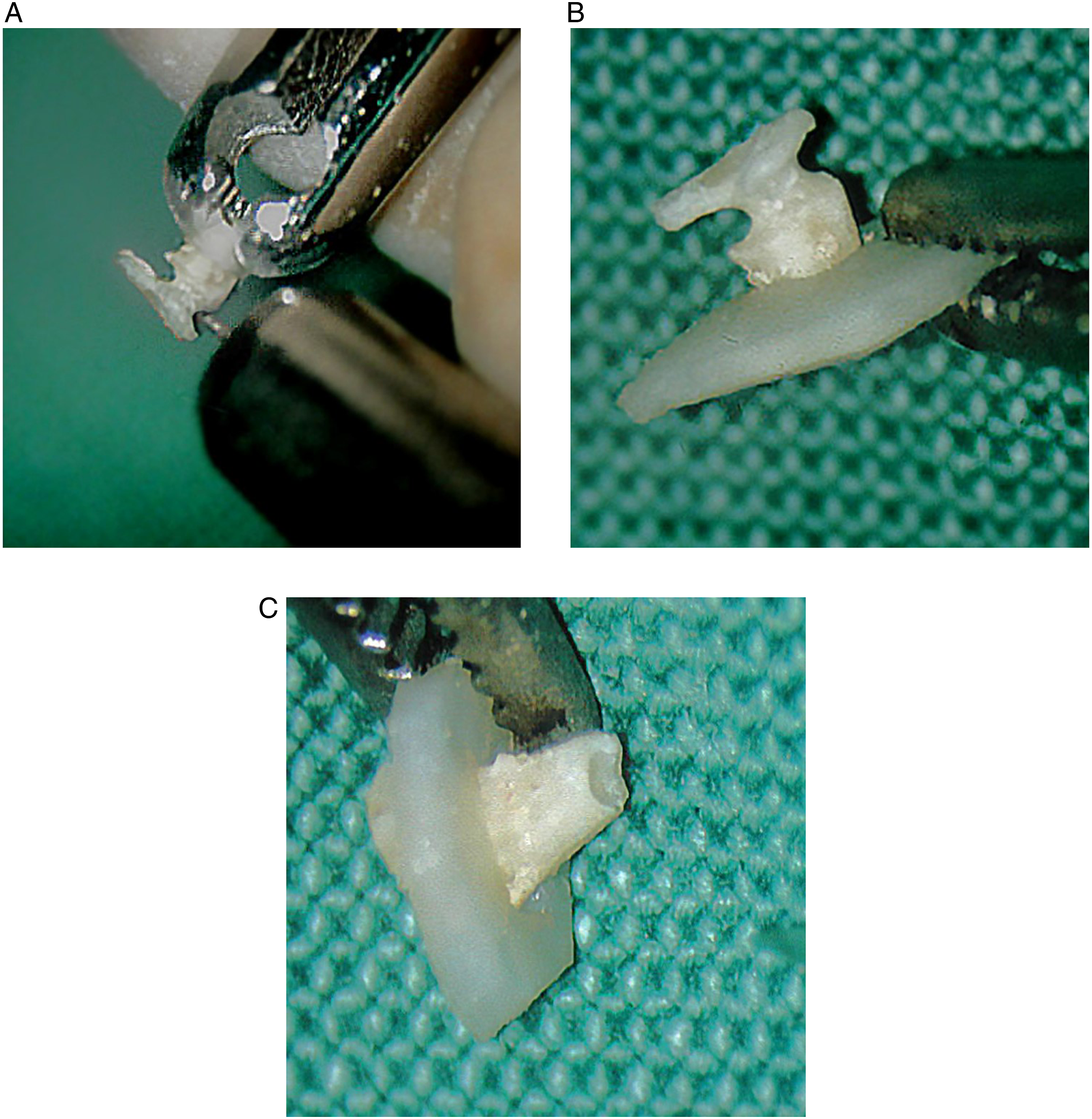
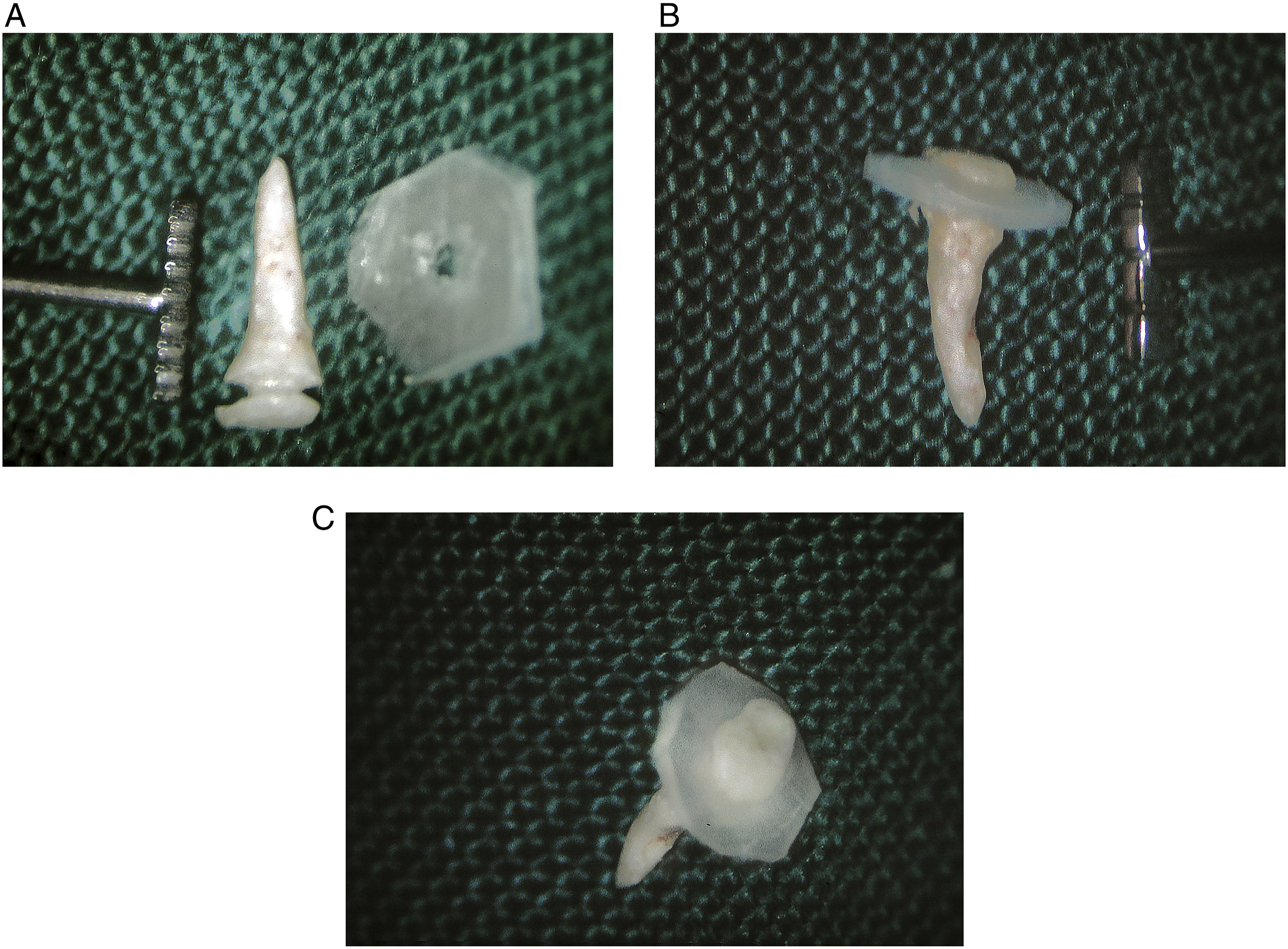
The surgical procedure of ossiculoplasty using OCCG was as follows (Figure 1). The pathologic incus was removed from the incudomalleolar joint. While the ossicle was held with microforceps, it was reshaped into the shaft using a drill with a 1-mm diamond burr. Using a #11 knife, autologous tragal or homologous septal cartilage was reshaped to the plate. A hole was drilled into the cartilage plate so that the reshaped ossicle fits inside the hole. By combining the shaft and the plate, an umbrella-shaped prosthesis was constructed. A small hole at the bottom for stable placement of BCCG as PORP over the stapes was made with a 1-mm diamond burr (Figure 2). The TORP procedure was identical to PORP, except for the length and the base part of the shaft, which was suitable for the footplate of the stapes (Figure 3). Diagrams of designing procedures for the ossicle-cartilage composite graft Ossicle-cartilage composite graft (OCCG) for partial ossicular replacement prosthesis (PORP). (A) Using diamond burr, the incus was drilled and reshaped to make a groove for cartilage. (B) The reshaped incus was connected to the cartilage. (C) A small hole at the bottom of reshaped incus was made to allow stable placement of OCCG over the head of stapes. Ossicle-cartilage composite graft (OCCG) for total ossicular replacement prosthesis (TORP). (A) The incus was carved to be a stalk and cartilage was shaped to be the cap of OCCG for TORP. (B and C) OCCG of TORP was the same with PORP except that the design of the stalk in TORP was longer and thinner than PORP and was flat in base.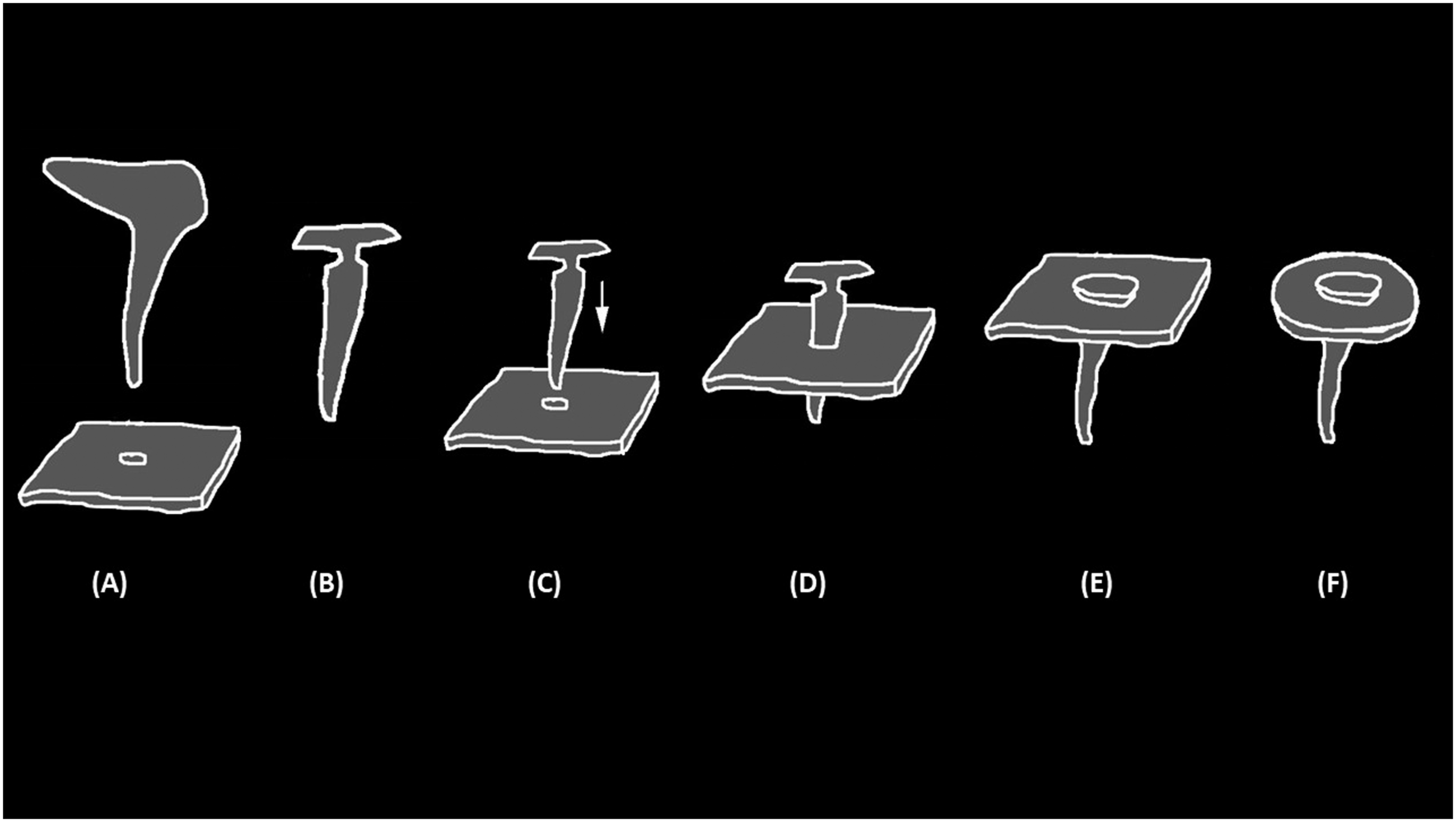
Same as above in the synthetic group, IONOS® PORP or TORP (Medizinische Produkte GmbH, Seefeld, Germany) was used for ossicular reconstruction. A piece of autologous conchal cartilage was placed over the prosthesis to prevent its extrusion, followed by temporalis fascia grafting.
Audiometric Outcome
All the patients underwent audiometry assessments before and after surgery. The average thresholds of pure tone at 500, 1000, 2000, and 4000 Hz were calculated for pre- and post-operative comparisons.
The assessment data also included post-operative air-bone gap (ABG), post-operative air-conduction (AC) threshold, and post-operative bone-conduction (BC) threshold. Post-operative ABG of 20 dB or less was considered a successful hearing result. Audiometry was reported according to the American Academy of Otolaryngology-Head and Neck Surgery guidelines, except for the thresholds at 3 kHz, which were substituted in all the cases with thresholds at 4 kHz.
Statistical Analysis
Baseline variables were expressed as mean ± standard deviation for continuous variables and number including percentage for categorical variables. Demographic details and post-operative hearing results between the 2 groups were compared using Student’s t test for continuous variables and Pearson χ2-test for categorical variables. All data were analyzed using SPSS statistics (IBM, version 21.0). A two-tailed P-value less than .05 was considered significant.
Results
Demographic Details of the OCCG and IONOS® Ossiculoplasty Groups.
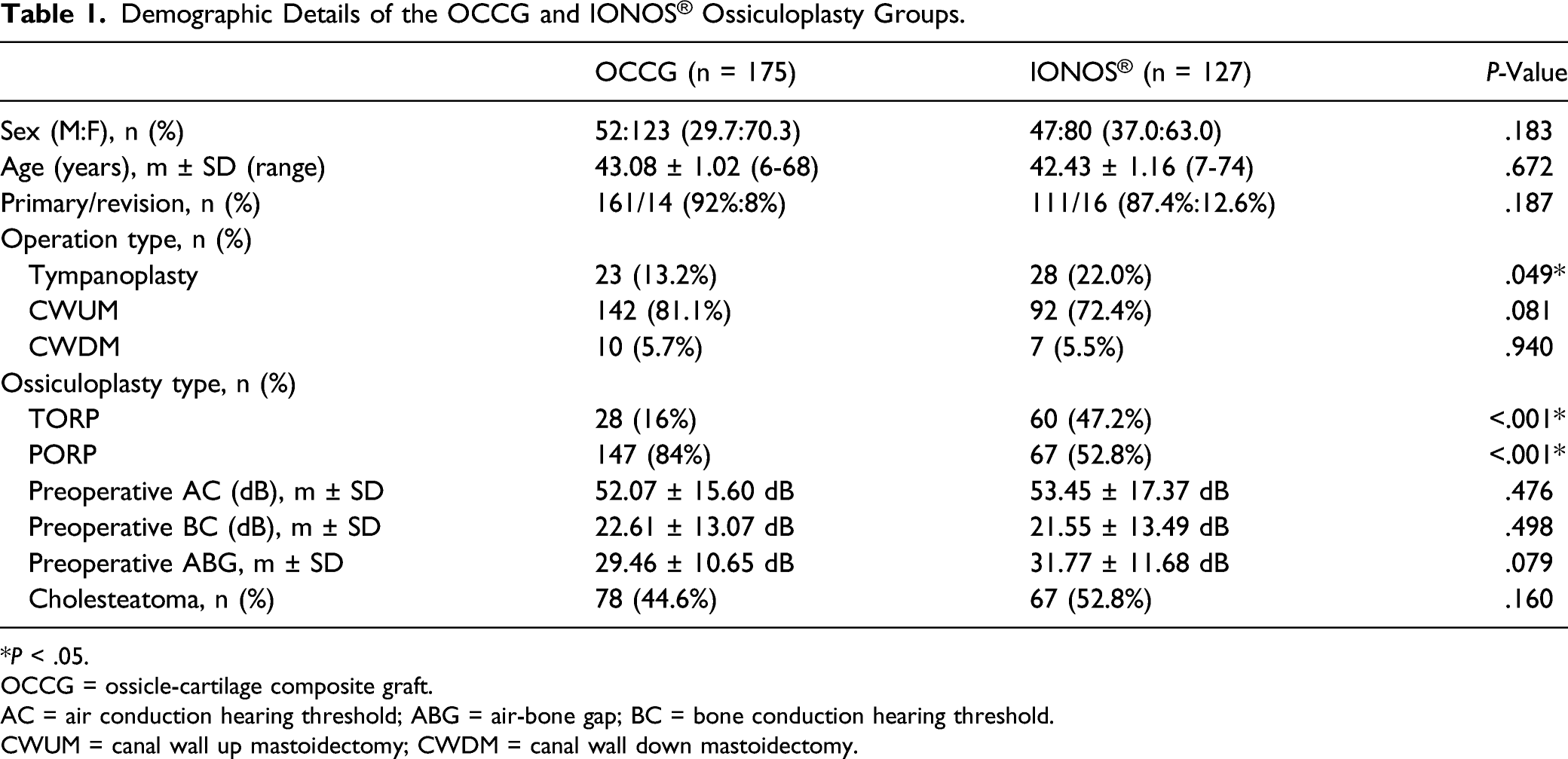
*P < .05.
OCCG = ossicle-cartilage composite graft.
AC = air conduction hearing threshold; ABG = air-bone gap; BC = bone conduction hearing threshold.
CWUM = canal wall up mastoidectomy; CWDM = canal wall down mastoidectomy.
Comparison of Post-Operative Hearing Results With OCCG and IONOS®.

*P < .05.
OCCG = ossicle-cartilage composite graft; Post-op AC = Post-operative air conduction hearing threshold.
Post-op BC = Post-operative bone conduction hearing threshold; Post-op ABG = Post-operative air-bone gap; ABG 20 = Air-bone gap closure within 20 dB; ABG 10 = Air-bone gap closure within 10 dB.
ABG gain = Air-bone gap gain; ACG = Air conduction gain.
Comparison of Outcomes According to the Follow-Up Period Between OCCG and IONOS®. For Follow-Up Periods Greater than 12 Months, the Two Groups Exhibited Statistical Differences of ABG Gain and Protrusion Rate.
*P < .05.
OCCG = ossicle-cartilage composite graft; Post-op ABG = Post-operative air-bone gap; ABG gain = Air-bone gap gain; ABG 20 = Air-bone gap closure within 20 dB; ABG 10 = Air-bone gap closure within 10 dB.
Discussion
The purpose of chronic otitis media surgery is to completely eliminate inflammation, prevent recurrence, and improve hearing. Most chronic middle ear diseases invade the ossicles, requiring reconstruction of the affected ossicles. 8 Many factors such as the presence of stapes superstructures, implantation material, condition of middle ear mucosa, E-tube function, reconstruction type, and methods affect the outcomes. 2 Since 1950, various surgical techniques and materials have been used for ossicular chain reconstruction, but there are still no standardized techniques or ideal materials that are accepted worldwide. Three general classes of prosthesis are used today: autograft, homograft, and allograft. The autograft prosthesis is a procedure that uses ossicles, cartilage, cortical bones, etc. This method has high biocompatibility, can be implemented immediately, and exhibits low extrusion rates and infection frequencies. 9
Hall and Rytzner introduced autologous ossicular graft incus in 1957, 10 followed by the introduction of ossicular reconstruction using cortical bone by Hough in 1959 11 and Zollner in 1960. 12 Autologous incus grafts are currently the most commonly used technique in the world, and many good results have been reported for ossiculoplasty using autologous ossicles. However, this technique is limited in cases of cholesteatoma or severe inflammation. 13 Therefore, several methods have been introduced to complement single autograft and these methods have shown comparable results. Malhotra introduced an umbrella-shaped graft that combined autologous malleus-conchal cartilage, and demonstrated hearing gain of 77.3% in 22 patients. 6 Kong et al. used mushroom-shaped autologous bone-cartilage composite graft (BCCG) for ossicular reconstruction, and compared the results to those of synthetic prosthesis. The hearing results were not statistically different from those of synthetic prosthesis, and the complication rate, including dislocation, was found to be lower. 7
The use of autologous cartilage requires additional incisions and surgical procedures, which lead to prolonged operation times. Therefore, this study also introduced an OCCG using homologous septal cartilage, which was previously stored in a cartilage bank. We compared this prosthesis with IONOS, the synthetic material. IONOS, a polymaleinate ionomer developed in 1969, has been used as a filling material in dentistry for over 15 years. It can endure large forces such as those of drilling without breaking and is sufficiently malleable to be shaped into any desired form. 2 In a study of ossiculoplasty using IONOS, the proportion of successful hearing gain (ABG closure of less than 20 dB) was 59% for the PORP group and 58% for the TORP group with a protrusion rate of 2.5%. 14
We analyzed the anatomical and functional results and found that hearing improvement and graft take-up rate were significantly better in the OCCG group. An average post-operative ABG closure of less than 20 dB was considered successful hearing gain and was seen in 67 cases (38.3%) of OCCG and 34 cases (26.8%) of IONOS prosthesis. Post-operative ABG exhibited hearing gain of 22.36 ± 9.41 dB in the OCCG group, which is statistically lower than the 25.08 ± 9.70 dB of the synthetic group.
The protrusion rate was also very low in the OCCG group. We categorized these 2 groups by follow-up periods into 3 categories: under 6 months, 6–12 months, and 12 months or longer, and compared the hearing results and protrusion rates among these periods. For most of the follow-up periods, the 2 groups did not exhibit significant statistical differences in audiologic outcomes or protrusion. However, for the follow-up periods of more than 12 months, the 2 groups showed statistical differences in ABG gain and protrusion rate. The total protrusion rate was 12.3% in the synthetic group, which is significantly higher than the OCCG group. This is because the reconstruction of autologous ossicles is well tolerated because it is more physiological and biocompatible, thereby resulting in better hearing results and reducing graft extrusion rates. In addition, the use of septal cartilage may provide additional stability to OCCG. Septal cartilage exhibits stiffness that is significantly higher than those of other cartilage. In a study comparing the structure and mechanical characteristics of ear, alar, and septal cartilage, septal cartilage exhibited stiffness significantly higher than those of alar cartilage and conchal cartilage. 15 Because of this characteristic, septal cartilage is sometimes used for other types of reconstruction, such as orbital walls in blowout fractures. In a study of orbital wall reconstruction surgeries using septal cartilage and conchal cartilage, the group using septal cartilage had better outcomes in both enophthalmos correction and residual enophthalmos, especially for long-term follow-up. 16 Considering these biochemical features, ossicle reconstructions using septal cartilage may have more structural advantages in maintaining long-term hearing.
This study is the first large-scale study to compare OCCGs with synthetic materials, and the grafts exhibited sufficient biocompatibility, stability, and good hearing gain. Since all the procedures were performed by a single surgeon at a single hospital, bias related to the surgeon ability can be excluded, resulting in very high reliability.
One of the limitations of this study can be heterogeneity of each subgroup. Because we reviewed the cases performed by a single surgeon in a single institution retrospectively, each surgery type or material choice was not identical. However, if multiple surgeons participate to match the homogeneity, it can also be a bias. Safety problem about homologous materials also can be an issue. However, in a comparative study of ossiculoplasty using homologous septal cartilage and autologous conchal cartilage, homologous cartilage showed similar results for both hearing and complication rates. 17 With sufficient informed consent and preliminary screening to eliminate the possibility of transmitted diseases, homologous cartilage-autologous ossicle grafts can be a good option for ossicular reconstructions. The surgical technique is delicate and needs practice; however, it took less time than acquiring additional autologous cartilage, and was less complicated than incus interposition.
Conclusion
Ossicle-cartilage composite graft is a biocompatible, easily harvested material that has very few side effects. Reconstruction using OCCG resulted in better hearing outcomes compared to when synthetic materials were used. Ossicle-cartilage composite graft also exhibited no protrusion in this study. With sufficient informed consent and preliminary screening to eliminate the possibility of transmitted diseases, OCCG can be a good option for ossicular reconstructions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (2020R1F1A107220911).