
Abstract

Keywords
Significance Statement
Neuroglial heterotopia or glial choristoma (GCH) of the middle ear and the mastoid cavity is an uncommon diagnosis with only 34 cases been reported as of today in the current literature. We present 2 clinical reports of GCH diagnosed in patients who underwent a mastoidectomy. In the first one, the patient’s GCH was located at the epitympanum, and in the second one, in the middle ear.
Clinical Report 1
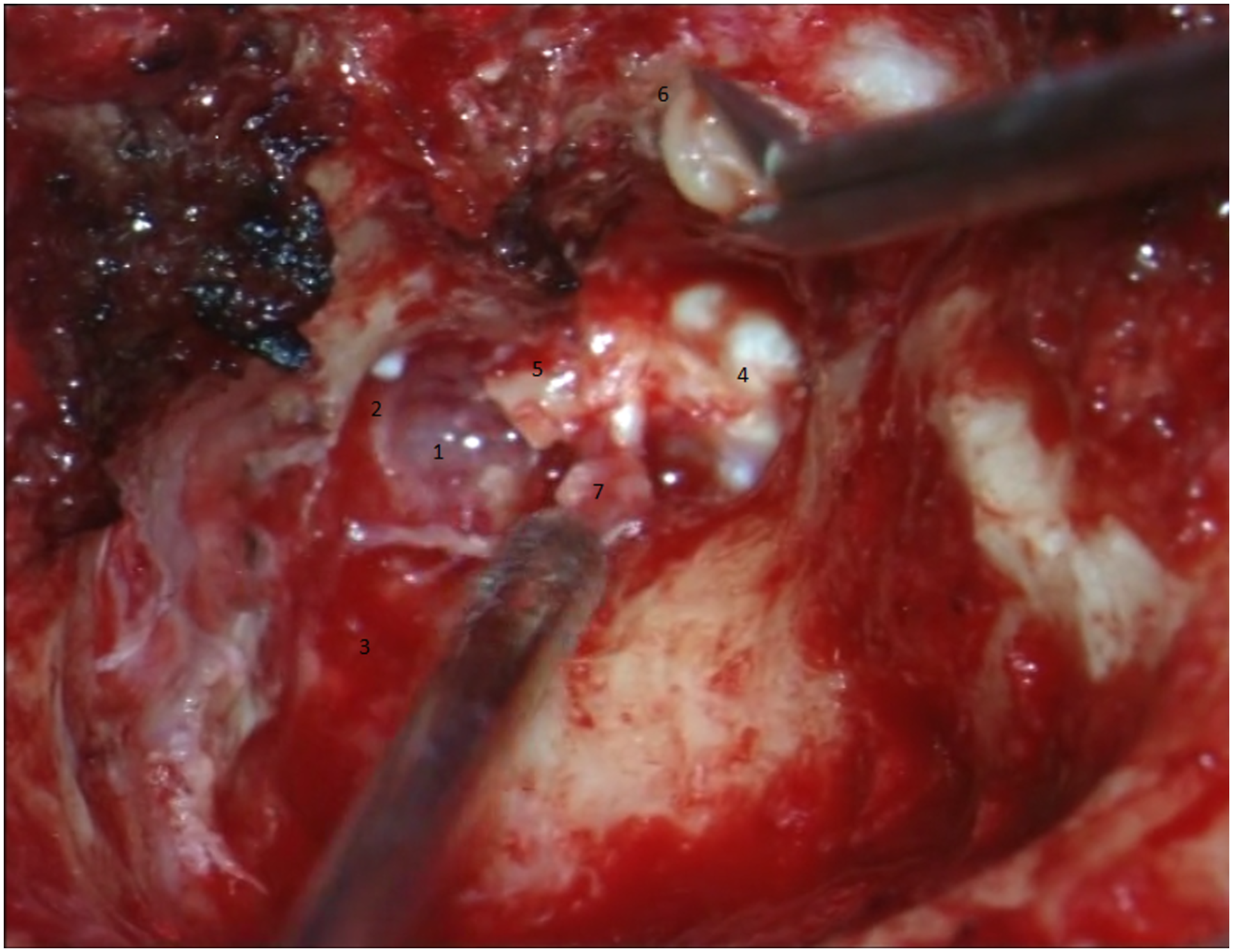
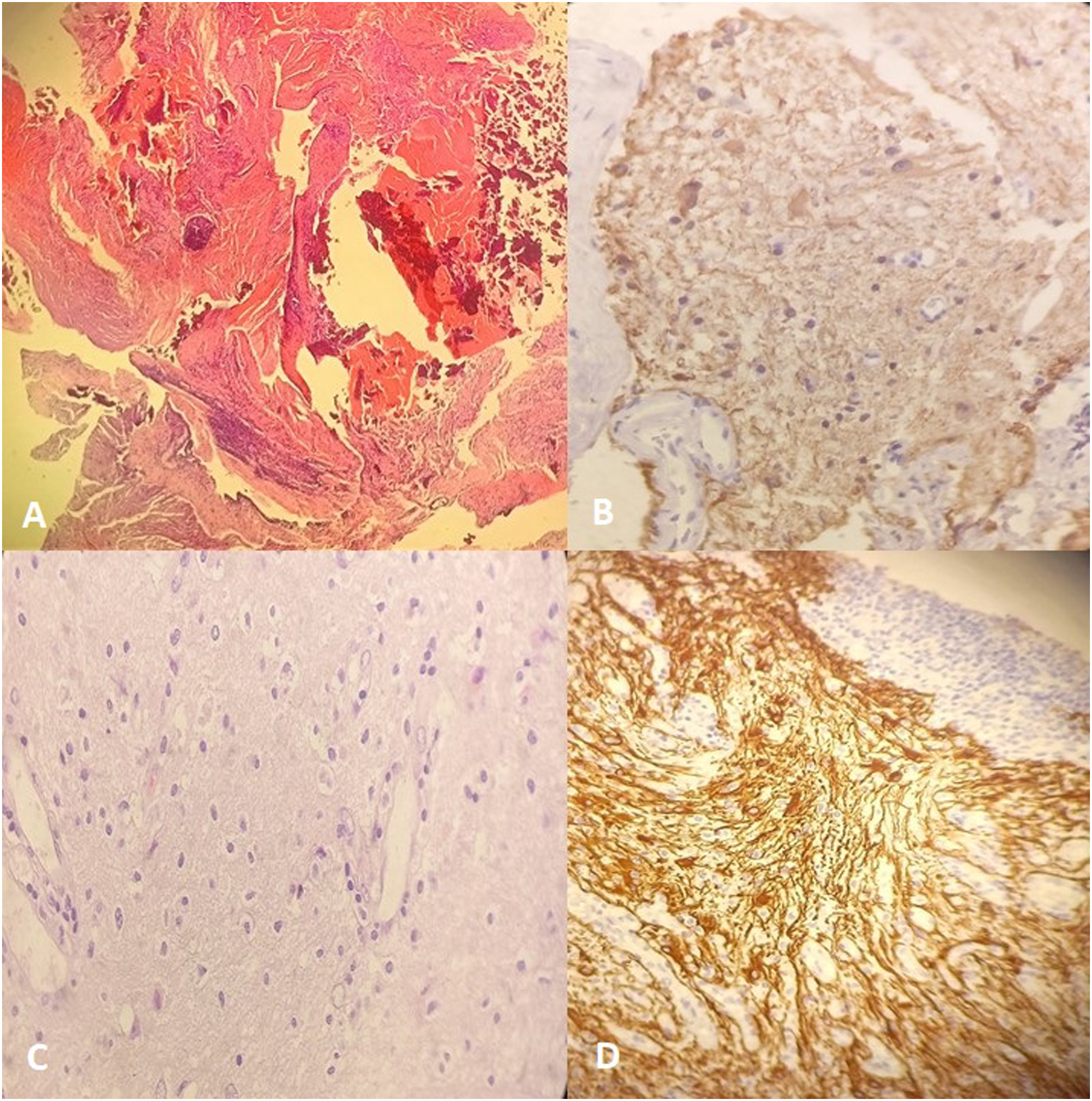
A 65-year-old male patient was referred to our ear, nose and throat department, with 1 year history of right-sided ear fullness and recurrent episodes of vertigo. The patient had a history of chronic otitis media with cholesteatoma treated with mastoidectomy and tympanoplasty approximately 35 years ago. Otoscopic examination was normal. Pure-tone audiometry showed conductive mild hearing loss on the right ear. Computed tomography (CT) showed soft-tissue density present inside the middle ear and mastoid cavity (Figure 1A). The patient was scheduled for a revision mastoidectomy. During the operation, granulomatous tissue was recognized inside the mastoid cavity, while the epitympanic space was occupied by a soft-tissue and gelatin-like consistency mass (Figure 2). Histopathological and immunohistochemical examination revealed a GCH (Figure 3A and 3B). The patient was discharged after 5 days and remains symptom-free 2 years later. Coronal computed tomography (CT) images of (A) the right temporal bone (clinical report 1) and (B) facial bones (clinical report 2), showing pathologic tissue of the middle ear and mastoid cavity. Yellow arrows show the place where the glial choristoma was found. Intraoperative image of revision mastoidectomy (clinical report 1) showing (1) the mass (glial choristoma), (2) the epitympanic space opened, (3) that the scutum was removed, (4) the antrum, (5) the tympanic membrane, (6) the rest of the malleus (the head was removed), (6) the head of the malleus, and (7) the head of the stapes. Histopathological and immunohistochemical examination showing (A and C) glial masses composed of astrocytic cells with large amounts of glial fibrils (H&E, Ax4, Cx10); (B and D) GFAP +. H&E indicates hematoxylin and eosin, GFAP indicates anti-glial fibrillary acidic protein, (A and B) concern the clinical report 1, and (C and D) concern the clinical report 2.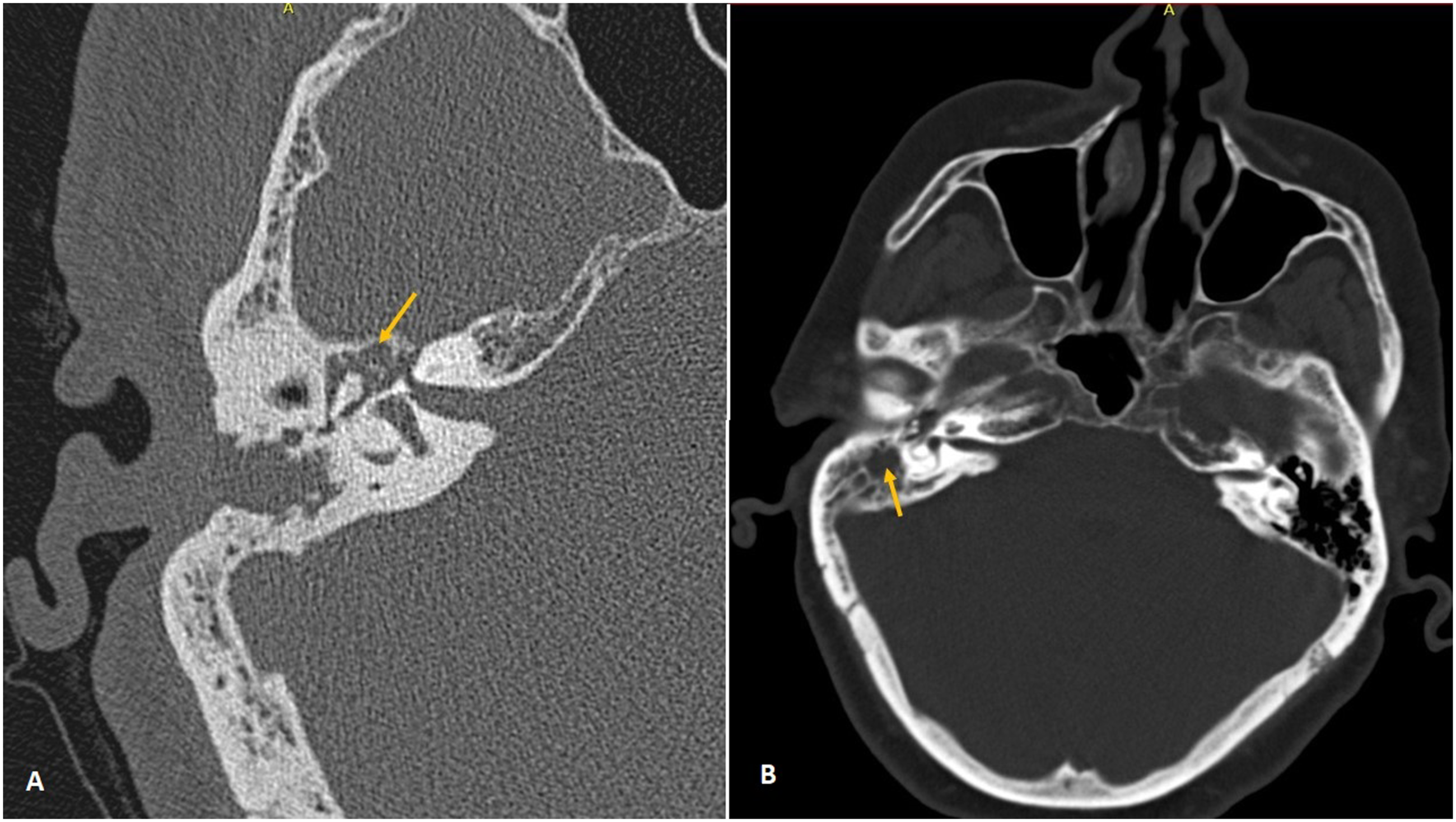
Clinical Report 2
A 68-year-old female presented to the emergency department of our hospital with a 4-day history of fever, vomiting, right-sided otalgia, and drowsiness the last 1 day. The patient was febrile (39.5oC), with signs of hypovolemia and a disturbed level of consciousness upon arrival. A brain CT scan was performed and revealed otitis media and mastoiditis of the right ear without signs of cerebral ischemia or abscess (Figure 1B). Clinical examination concurred with the diagnosis of otitis media, and thus, a myringotomy was performed, and an ear ventilation tube was placed. A magnetic resonance imaging (MRI) scan that followed 2 days later showed cerebral edema of the right temporal lobe and meningitis. Due to these new findings, the patient underwent a mastoidectomy. During the surgery, puss from mastoid cavity was drained, and inflammatory tissue was removed and sent for histological examination. The patient was admitted to the intensive care unit (ICU) for further treatment. Histopathological and immunohistochemical examination revealed a GCH (Figure 3C and 3D). After 1 week, the patient was discharged from the ICU in excellent condition and remained uncomplicated during the follow-up visits.
A neuroglial heterotopia or GCH is defined as the presence of normal mature glial tissue extracranially or outside the spinal cord. It is a rare finding, with only 34 cases being reported in the current literature after 1950.1,2 It can appear as a midline lesion, especially in the nasal cavity and nasopharynx, or more rarely in non-midline structures, such as the mastoid cavity, the middle ear, the eye and orbit, the skin, as well as other neck structures.2-4 The differentiation between a GCH of the middle ear and an encephalocele is the presence of a connection with the central nervous system, which can be discovered radiologically or intraoperatively.5-7 Out of the 34 case reports of GCH, 24 were located in the middle ear, and only 3 out of them had a mass present in the epitympanum. Furthermore, 6 cases describe a GCH in the mastoid cavity and 4 in both mastoid cavity and middle ear.1-3
The pathophysiologic mechanism is not yet completely understood, and a history of infection, inflammation, or trauma seems to contribute to its appearance. However, an anomaly during embryological development cannot be excluded.2,4-6
Middle-ear heterotopias are usually diagnosed in adulthood. Symptoms include otorrhea, episodes of otitis media, tinnitus, dizziness, and ear-fullness sensation. Otoscopic examination may not reveal any pathology and hearing loss of different degrees can be found with pure-tone audiometry. 6
Imaging studies are very helpful in order to detect the presence of pathologic tissue inside the middle ear and/or the mastoid cavity. CT scanning can reveal a soft-tissue lesion in the middle ear cavity or/and the mastoid cavity, with or without tegmen tympani dehiscence, a close relationship with the facial nerve and the ossicular chain.2,6,8 An MRI scan can be of assistance, firstly, to determine central nervous system involvement, and secondly, with the differential diagnosis, which includes cholesteatoma, paraganglioma, adenoma, meningioma, retrotympanic vascular tumor, endolymphatic sac tumor, and carcinoma.1,2
Histopathological examination of the mass after its removal confirms diagnosis, with normal glial tissue, or rarely, ependymal or choroid plexus present. Immunohistochemical markers that are usually examined include antibodies such as anti-glial fibrillary acidic protein (GFAP), anti-cytokeratin, anti-NEU N, as well as CD34 and CD68.1,4
Treatment includes surgical removal of the ectopic tissue, and intraoperative examination is important to determine the exact location and the relationship of the mass with the middle-ear structures. Some authors suggest partial removal of the lesion, if it is adhered to the facial recess or the ossicular chain, because a malignant transformation has not yet been described.1,8
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
We declare that written informed consent for patient information and images to be published was provided by the patient.