
Abstract

Significance Statement
This case report demonstrates the first case of a hypoglossal nerve stimulator (HGNS) system’s implantable pulse generator (IPG) experiencing electromagnetic field (EMF) interference from a distal spinal cord stimulator (SCS), which resulted in device failure. The effects of EMF interference on HGNS systems are currently not well understood. Given that the patient had a previously implanted, contralateral, non-functional HGNS system, this was successfully treated with a contralateral stimulation lead crossover.
Special Topics Clinic
A 44-year-old male with a history of lumbosacral radiculopathy and obstructive sleep apnea (OSA) presented to clinic with CPAP failure. His recent home sleep study demonstrated an apnea-hypopnea index (AHI) of 34.8 events/hour. Drug-induced sleep endoscopy (DISE) revealed soft palate anterior-posterior (A-P) collapse and limited lateral oropharyngeal wall collapse. Notably, the patient had been expecting to undergo SCS placement (Medtronic, Minneapolis, MN) for radiculopathy. Right-sided HGNS implant (Inspire Medical Systems, Golden Valley, MN, USA) with the three-incision approach was offered and performed after case discussion with the HGNS manufacturer regarding possible HGNS-SCS interference. Intraoperatively, he had good tongue protrusion with no retrusor branches on nerve monitoring and expected tongue movement on neurostimulator analysis postoperatively. Five weeks after right HGNS placement, he underwent implantation of a two-lead lumbar SCS and an associated left flank IPG. During SCS implantation, potential HGNS interference was not evaluated. Only until after SCS surgery did he undergo activation and titration of the right HGNS. Subsequent polysomnography (PSG) HGNS titration study demonstrated rapid succession obstruction of nearly once per minute, no improvement at higher stimulation, and a worsened AHI to 103.9 events/hour. This worsening was thought to be likely secondary to inadvertent inclusion of retrusor branches. Repeat DISE was performed to clarify this supposition, and this demonstrated A-P collapse of retropalatal and retrolingual airways worsened by right HGNS-induced elevation of the right tongue base against the palate.
Per HGNS manufacturer, stimulator cuff repositioning would unlikely be successful due to scarring, and it was recommended that a new, left-sided HGNS implant system, including a left-sided respiratory sensor, IPG, and stimulator cuff, or, alternatively, to implant a new left-sided stimulator cuff routed to the right-sided IPG. Six months later, a left HGNS system was implanted with the two-incision approach and the IPG in standard bipolar configuration, leaving the right HGNS system intact, inactive. On postoperative day one, the patient reported uncontrolled tongue and jaw protrusion upon SCS activation, with the left HGNS device off, which persisted after SCS stimulation adjustments. Despite the positioning of the implants, in which the right HGNS, left HGNS, SCS, and their subcomponents were at least six inches distant from each other per manufacturer recommendations, there was concern of left-sided HGNS IPG and SCS IPG proximity-related cross-communication, leading to uncontrolled left HGNS activation. After discussions with the HGNS and SCS manufacturer representatives, the decision was made to remove the left HGNS IPG and respiratory sensor lead and reroute the left HGNS stimulator to the right HGNS IPG over the sternum from the left to the right chest incisions, see Figures 1 and 2. After completion, both the HGNS and SCS systems were interrogated by manufacturer representatives, and visible tongue movement was observed without concurrent SCS interference. The left HGNS and left SCS were working appropriately after surgery with no interference. PSG six months after surgery demonstrated surgical success, with an all-night AHI of 10.2 events/hour. X-ray Device Configuration. A. is an x-ray taken after patient’s first surgery demonstrating a right-sided INSPIRE system with a right-sided respiratory cycle sensing lead (black arrow), and the implantable pulse generator (IPG). B. is an x-ray taken after patient’s second surgery demonstrating the new left-sided INSPIRE system with left-sided respiratory cycle sensing lead (black arrow). The right-sided INSPIRE system is inactive at this time. The new spinal cord stimulator leads can now be seen along the vertebrae (black arrow heads). C. is an x-ray taken after patient’s third surgery demonstrating the final postoperative configuration of the bilateral INPSIRE system. The left IPG is removed, as is the left-sided respiratory cycle sensing lead. The active circuit starts with the sensing lead from the right side transmitting to the right sided IPG, which is then transmitted to the left hypoglossal nerve via the stimulation lead traveling across the chest and then up the left neck. Device Crossover Diagram. A. demonstrates the preoperative configuration of bilateral hypoglossal nerve stimulators. The right INSPIRE system shows a right-sided respiratory cycle sensing lead, which transmits a signal to the right-sided implantable pulse generator (IPG), which is then transmitting to the right hypoglossal nerve. The stimulation lead then carries the signal to the right electrode to the right hypoglossal nerve. The left INSPIRE system shows left-sided sensing lead transmitting to the left-sided IPG which is then transmitting to the left hypoglossal nerve. The spinal cord stimulator is located along patient’s left side. B. demonstrates the final postoperative configuration of the bilateral hypoglossal nerve stimulators following stimulator lead crossover. The left IPG is removed, as is the left-sided respiratory cycle sensing lead. The active circuit starts with sensed respirations from the right side, which then transmits a signal to the right-sided IPG. The signal is then transmitted via the right stimulation lead across the chest to the left hypoglossal nerve electrode.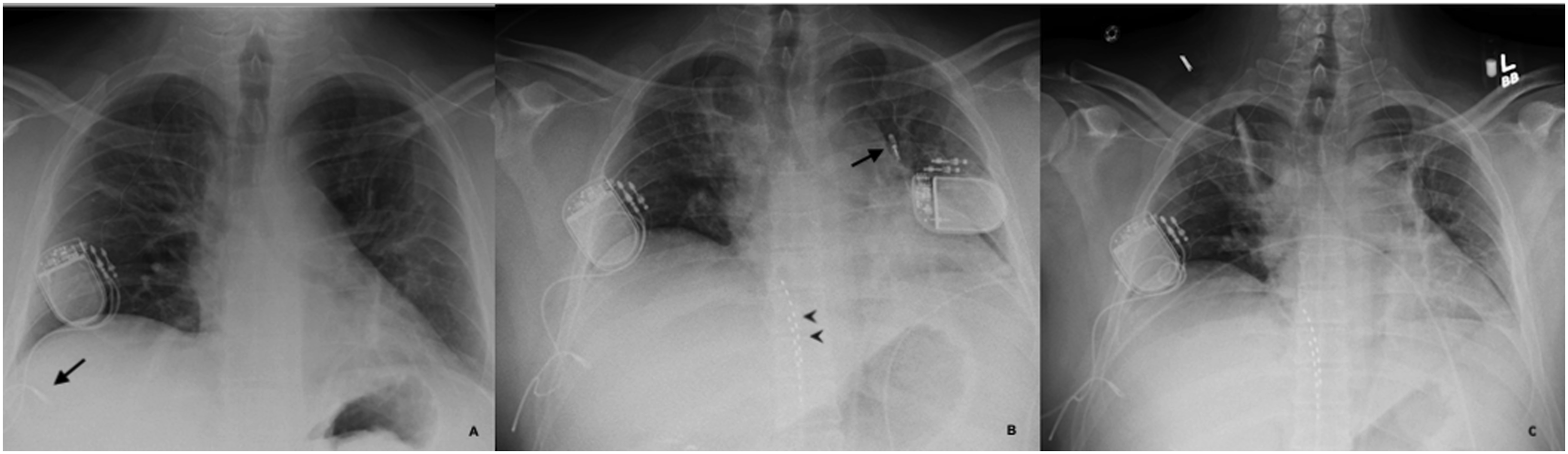

Discussion
Hypoglossal nerve stimulator effectively treats OSA patients with CPAP intolerance.1,2 Surgical challenges encountered during the standard unilateral implant have prompted attempts to re-route the stimulator and/or sense leads to the contralateral side from the IPG.3,4 This case is unique since device rerouting was due to EMF. It is unclear why the first (right-sided) HGNS worsened the patient’s OSA. One explanation is electrode malfunction and stimulation of the tongue’s retractor muscles. The second (left-sided) HGNS IPG may have experienced proximity-related EMF interference with the SCS IPG, even with the left HGNS turned off.1,5 The second (left-sided) HGNS implant was performed with the two-incision approach with slightly differing positioning of the respiratory sensing lead. 6 However, per the HGNS device manufacturer, the primary concern was over IPG interference, which may be undetectable intraoperatively. When the SCS was maximally activated at both the beginning and end of the final case, no tongue movement was detected, and we were unsure the interaction was eliminated until the patient awakened. Stimulator lead crossover from the left chest incision across the sternum to the right chest IPG was feasible with the standard stimulation lead length and successfully solved the interference problem.
Footnotes
Acknowledgments
We would like to acknowledge the West Virginia University Department of Otolaryngology-Head and Neck Surgery for its insights and support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was determined to be exempt and approved by the West Virginia University Institutional Review Board.