
Abstract
Accidental swallowing of fish bone is one of the most common emergencies in the otolaryngology department. The impacted fish bones are usually found in the palatine tonsil, base of the tongue, valleculae, pyriform sinus, and esophagus, which can be successfully removed after a thorough examination. However, in some cases, the fish bone may penetrate into the neck soft tissue and migrate to extraluminal organs, causing infection, abscess formation, or rupture of vessels. In such cases, prompt recognition and immediate removal of the impacted fish bone are necessary. Herein, we report a rare case of a 60-year-old woman who had accidently swallowed a fish bone 10 days prior to visiting the outpatient department. The fiberoptic scope and head and neck computed tomography scans were obtained from the outpatient department. The fish bone was found to migrate from the upper esophagus to the left thyroid gland. First, a rigid esophageal endoscopy was performed in the operating room, but no obvious fish bone was noted over the esophagus. Finally, the fish bone was removed via exploratory cervicotomy with left-sided total lobectomy of the thyroid. The patient recovered after the operation, and there were no further complications during the 3 years of follow-up.
Introduction
Accidental swallowing of fish bone is a common emergency referral or otolaryngology outpatient department visit condition. The fish bones discovered in the upper digestive tract are usually located in the palatine tonsils, base of the tongue, valleculae, pyriform sinus, and esophagus.1,2 Migration of the impacted fish bone into extraluminal soft tissues or organs could cause significant complications; thus, immediate surgical intervention for removal of the impacted fish bone is essential to reduce morbidity and mortality. Herein, we report a case of fish bone migration from the upper esophagus to the left thyroid gland. The fish bone was successfully removed via exploratory cervicotomy with left-sided total lobectomy of the thyroid.
Case Report
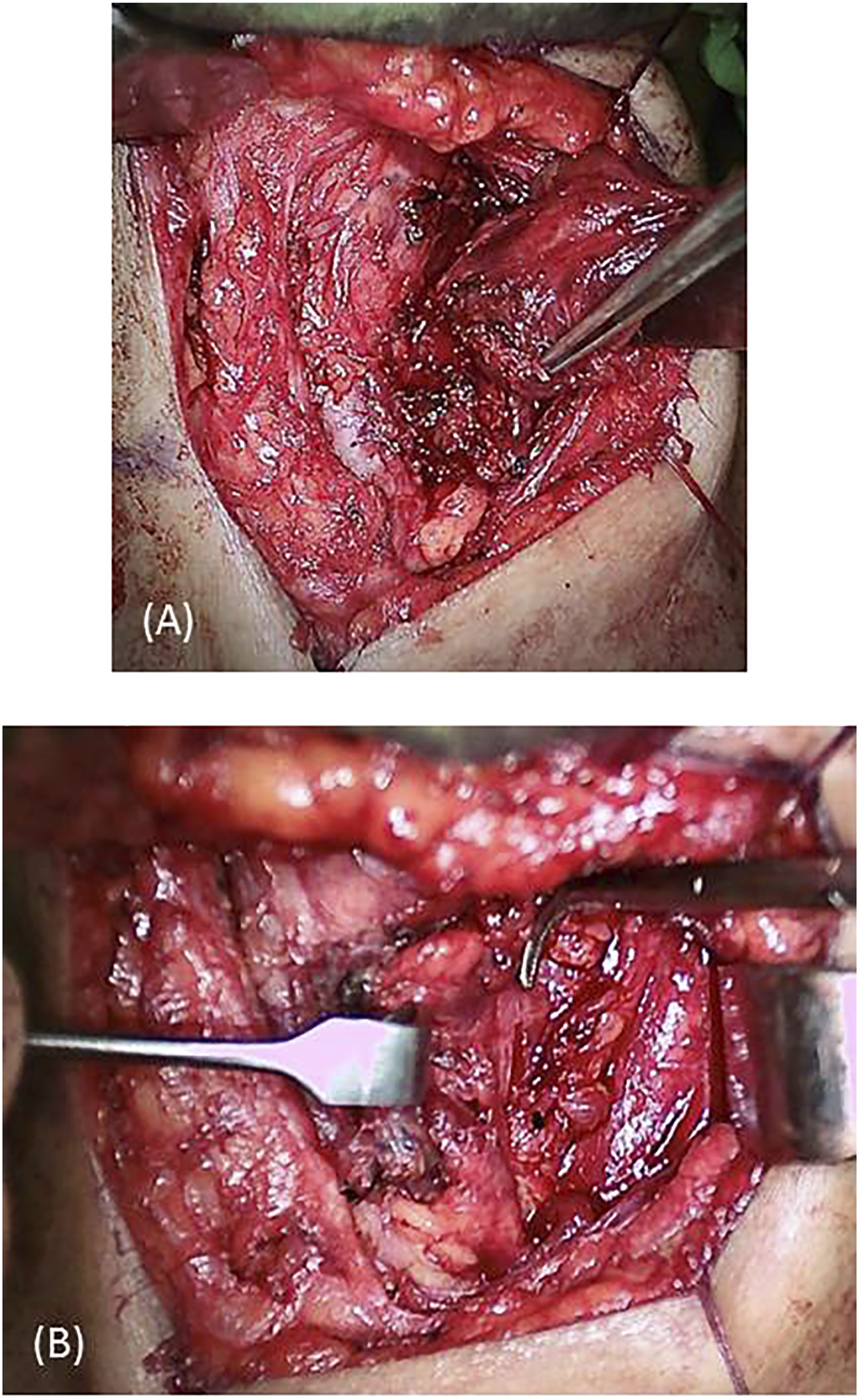
A 60-year-old woman visited our outpatient department with the chief complaint of a lumping throat and odynophagia for 10 days after accidently swallowing a fish bone. She had previously visited otolaryngology clinics, but no fish bone was found. Her throat pain during swallowing worsened daily. On physical examination, the patient’s neck was supple without swelling, but there was obvious tenderness and tingling sensation over her left lower paramedian neck. No fish bone was visible over the oropharynx or hypopharynx under flexible fiberoptic nasopharyngoscopy. Laboratory data revealed normal white blood cell count and slightly elevated levels of C-reactive protein (6.2 mg/dL). Due to a high suspicion of esophageal foreign body impaction, cervical computed tomography (CT) was performed, which showed a linear hyperdense lesion penetrating the upper esophagus into the left side of the thyroid gland (Figure 1). We first attempted the emergent operation of rigid esophageal endoscopy. However, no fish bone was visible in the esophagus. We then performed an exploratory cervicotomy with a lateral and inferior approach to the thyroid gland. After dissecting the left thyroid gland almost free from the trachea and esophagus while preserving the left recurrent laryngeal nerve, we found that the fish bone was almost embedded in the left thyroid gland. A hematoma and goiter were also observed within the left thyroid gland (Figure 2). Eventually, we performed a left total lobectomy of the thyroid, removing the 2.3-cm long fish bone (Figure 3). The patient’s postoperative recovery was uneventful, and she was free of preoperative symptoms during the postoperative follow-up for 3 years. Her thyroid function was also normal during the follow-up. Computed tomography showing (A and B) a linear hyperdense fish bone (red arrow) in the axial view and (C and D) the fish bone embedded in the left thyroid gland in the coronal view. (A) Left fish bone tip embedded in the left thyroid gland (the forceps). (B) Left recurrent laryngeal nerve preserved after left thyroid lobectomy (the right angle forceps). Left thyroid gland and the 2.3-cm long fish bone.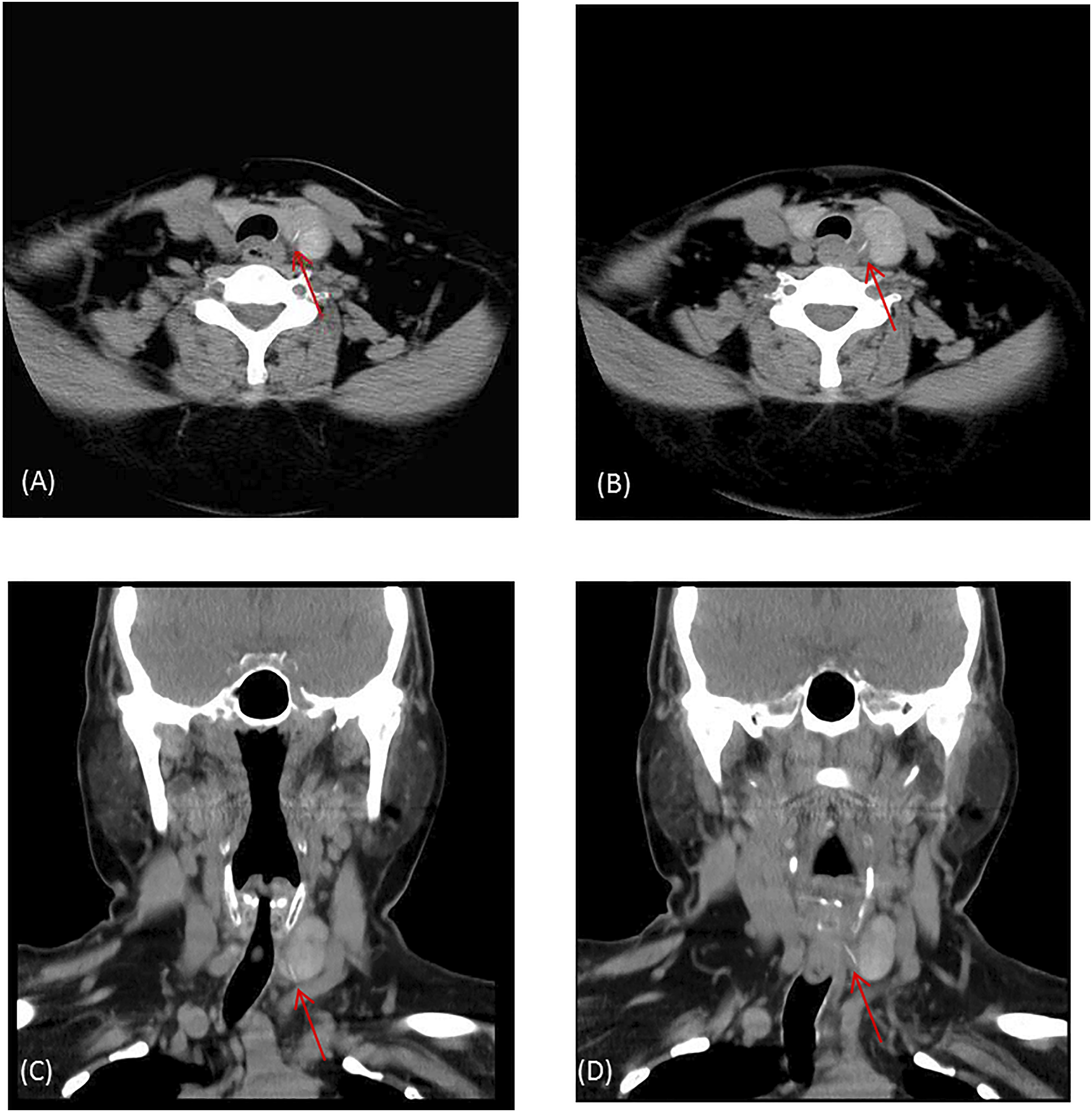

Discussion
Accidental swallowing of a foreign body is a common emergency in the otolaryngology department, and the fish bone is the most common foreign body (60%) that is accidentally ingested. 3 The cervical esophagus at the level of the cricopharyngeal muscle is the most frequent site of foreign body impaction in the esophagus (67%), and the symptoms include retrosternal pain (78%), dysphagia (48%), and odynophagia (43.4%).4,5 We must watch out for the major complications of penetrating foreign bodies in the esophagus, such as esophageal perforation with peri-esophagitis, para-esophageal abscess, mediastinitis, or vascular complications such as aortoesophageal fistula, innominate esophageal fistula, and carotid rupture. 6 Loh et al. reported 273 foreign bodies in the esophagus, with a major complication rate of 7.3% and a mortality rate of 0.73%. 7 Immediate localization and early retrieval of ingested foreign body impaction play an important role in reducing the morbidity and mortality rates.
If a patient with a clear history of accidental swallowing of a foreign body presents with obvious symptoms indicating foreign body impaction but the foreign body cannot be seen by detailed fiberoptic nasopharyngoscopy, foreign body impaction over the esophagus should be highly suspected. When there is a suspicion of foreign body impaction, we must arrive at a diagnosis as quickly as possible. The fastest approach is to use a lateral neck radiograph. However, the diagnosis can be challenging because ingested foreign bodies can be easily mistaken for calcified normal structures in the neck. 8 Cervical CT can provide more information, such as a diagnosis and whether tissue injury or abscess formation is present, and is useful for planning a surgical route. In a previous study, the initial CT interpretation demonstrated a sensitivity of 75% and specificity of 100%. 9 Another study reported that plain radiography detected 35.9% of the simple fish bones and 54.5% of the fish bones detected by CT in the esophagus. Therefore, CT should be considered the first-choice technique for the diagnosis of esophageal fish bone foreign bodies. 10 In patients > 40 years of age with suspected fish bone impaction, non-contrast CT is recommended and should be urgently performed, even in the presence of ambiguous symptoms such as the absence of localized pain. 11 In our case, we performed CT to identify the esophageal fish bone because the symptoms related to foreign body impaction persisted even after 10 days of observation and fiberoptic nasopharyngoscopy revealed saliva pooling over the hypopharynx but no foreign body impaction over the oropharynx and hypopharynx.
Extraluminal migration of an esophageal foreign body is rare, but it can occur in the lungs, liver, subcutaneous tissues of the neck, thyroid gland, major blood vessels, and pericardium.12-18 If extraluminal migration occurs, the procedure for removing the foreign body becomes more complicated, as in our case. Endoscopy should remain a part of the initial evaluation in order to evaluate soft-tissue injury that would not be evident in radiographic studies. 18 Initially, we performed rigid esophageal endoscopy to locate the fish bone tip and evaluate the esophageal mucosal injury. No visible fish bone or esophageal perforation was observed. A previous study reported an endoscopic approach of removing an esophageal foreign body with thyroid abscess drainage in order to avoid hemithyroidectomy and potential injury of the recurrent laryngeal nerve. 19 However, an endoscopic approach cannot be used in cases where the foreign body is almost totally imbedded into the thyroid gland. In our case, we chose to perform an exploratory cervicotomy with a left total lobectomy of the thyroid because (1) the fish bone was almost imbedded into the left thyroid gland, (2) hematoma formation and goiter was noted within the left thyroid gland, and (3) the left thyroid gland was almost free from the trachea and esophagus after dissection to preserve the left recurrent laryngeal nerve.
Fish bone migration from the esophagus to the thyroid gland is rare and difficult to diagnose based on common symptoms or with a fiberoptic scope. Prolonged fish bone impaction at the cervical esophagus may increase the possibility of perforation or migration, inducing major complications. CT scan can aid in the early detection and precise localization of foreign bodies. When an esophageal fish bone is diagnosed, esophagoscopy is always performed first. If the esophageal fish bone is found to have completely migrated into the thyroid gland, surgical intervention with exploratory cervicotomy and unilateral total lobectomy of the thyroid is a feasible option for removing the migratory fish bone.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.