
Abstract
Trigeminal schwannomas are rare tumours comprising 0.2% of all intracranial tumours and 0.5% of all head and neck tumours. Patients with trigeminal schwannomas presented with facial hypoesthesia and pain. We presented a case with left bulging oropharynx. The CT scan showed a 3.8x2.6x4.9cm left parapharyngeal tumour compressed to the oropharynx and middle cranial fossa. We performed 3 ways in two times of operation to excise the whole tumour. We chose the transoral approach for parapharyngeal space, trans-parotid approach for deep parotid part and the endoscopic endonasal trans-pterygoid approach and trans-maxillary with Canine fossa trephination for intracranial lesions. The pathology showed schwannoma. A huge schwannoma extended from intracranial to several spaces is difficult to resect just by one approach. We should separate the tumour to several parts by clinical image before the operation and design a plan to remove the whole tumour in different approach. The different space of tumour involvement had several ways to access. We needed to choose the less harm but with better surgical field.
Introduction
A schwannoma is a nerve sheath tumour arising from the perineural Schwann cells. Such tumours are solitary and slow-growing. 1 Approximately 20%–45% of all schwannomas are located in the head and neck region. 2 The vagus nerve and cervical sympathetic chain are the most common sites for schwannomas. 3 The most common type of intracranial schwannomas is vestibular schwannoma development. Trigeminal schwannomas are rare tumours accounting for approximately 0.2% of all intracranial tumours and 0.5% of all head and neck tumours.4-9 Patients with trigeminal schwannomas commonly present with facial hypoesthesia, pain and paraesthesia. 10 Magnetic resonance imaging (MRI) is the gold standard for diagnosing tumours. Schwannomas are radiologically characterized as well-demarcated masses that displace the surrounding structures without direct invasion and they frequently show cystic and fatty degeneration. 9 Surgical resection is considered the standard treatment for managing schwannomas. 11 In this report, we presented the case of a patient with a trigeminal schwannoma extending from the medial portion of the middle cranial fossa to the parapharyngeal space and deep parotid lobe. We resected the whole tumour via 3 approaches and reviewed the scientific literature of the schwannoma and surgical approach to the parapharyngeal space tumour.
Case Report
A 57-year-old female was diagnosed with left breast cancer after the operation and regularly followed up at the General Surgeon Department. She complained of left ear fullness that persisted for weeks. She visited a local physician, and a left oropharyngeal tumour was identified. She then presented to our clinic.
There was no dysphagia, odynophagia, body weight loss, facial hypoesthesia, paraesthesia or visual disturbance on admission. Physical examination revealed a giant left oropharyngeal bulging tumour with smooth mucosa. Computed tomography (CT) showed a 3.8 × 2.6 × 4.9–cm3 heterogeneous low-density lesion in the left parapharyngeal and masticator spaces, compressing the left side of the oropharynx, and left intracranial component involvement was suspected (Figure 1). Preoperative computed tomography images showing a 3.8 × 2.6 × 4.9-cm heterogeneous low-density lesion in the left parapharyngeal and masticator spaces; left side skull base involvement was suspected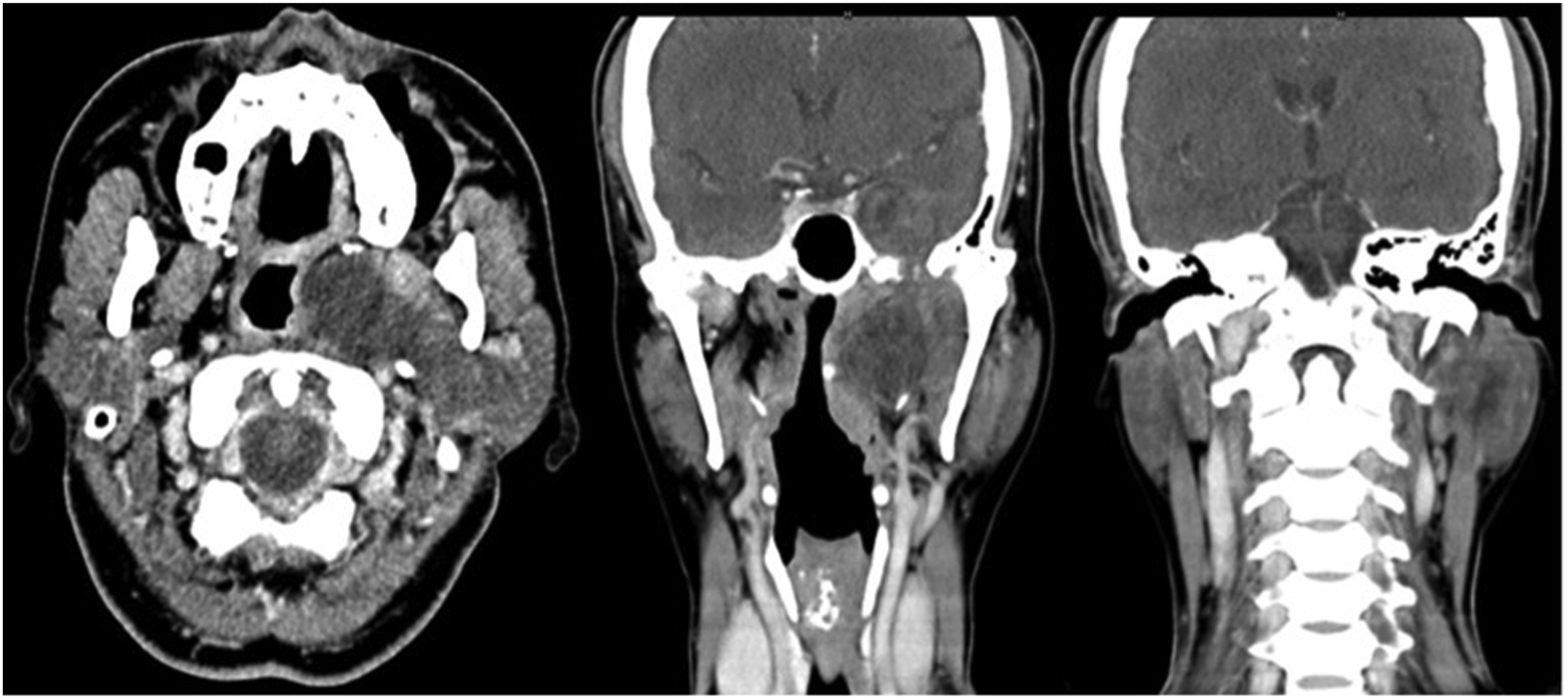
The left oropharyngeal tumour was excised for tissue proof via the transoral approach, and the stalks connecting the tumours in the deep parotid area and skull base were ligated. The tumour was well-defined and firm in consistency. The patient underwent MRI to check for residual tumours. Images showed a large lobulated enhancing tumour residue in the left parapharyngeal space abutting the deep lobe of the parotid gland and expanding through the left foramen ovale to the medial portion of the left middle cranial fossa. Pathology reports revealed a neurilemoma (schwannoma) with ancient changes (Figure 2). H and E staining of the specimen showing tumour cells composed of hypercellular Antoni A areas and myxoid hypocellular Antoni B; and the second; Immunohistochemical staining was positive for S-100 ruling out tumour of muscle origin.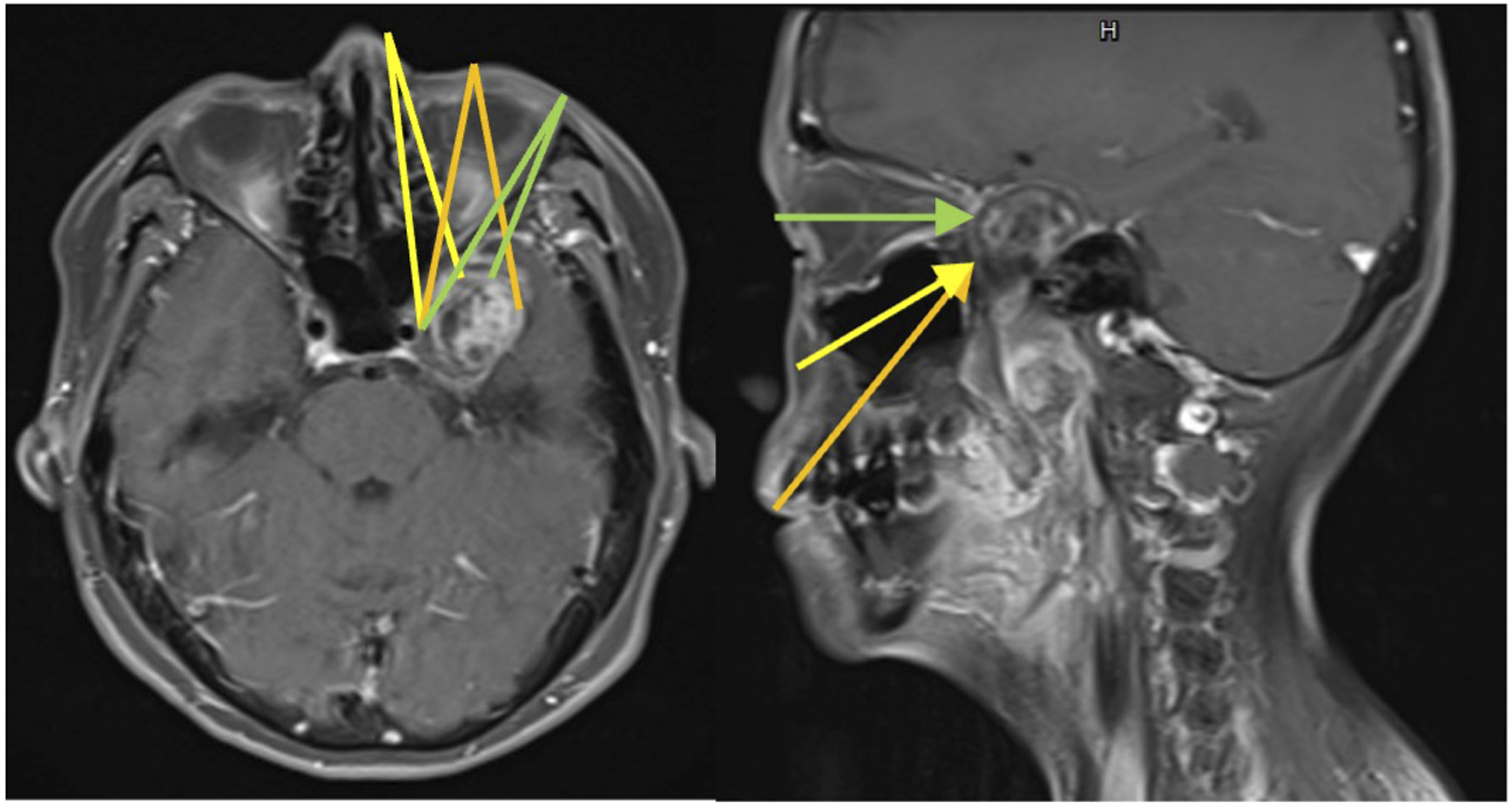
Excision was performed using the transparotid approach for facial nerve dissection of the tumour in the deep parotid area and the wound was closed before proceeding to the next step. Skull base tumour excision was initiated via the endoscopic endonasal transpterygoid approach. However, the tumour was located in the medial portion of the middle cranial fossa and the lateral side of the Meckel’s cave, making it difficult to access via the transpterygoid approach as the Meckel’s cave may block the way to the tumour. We attempted to use the anterior transmaxillary approach (Caldwell–Luc operation) with canine fossa trephination to access and resect the tumour; however, we found that the visualization of the lateral side of the infratemporal fossa and skull base tumour was limited. We considered using the transparotid approach for the parotid area tumour first while keeping the wound open, which allowed us to press the tumour through the wound to obtain a clear view of the lateral side of the infratemporal area and the skull base tumour.
Postoperatively, the patient complained of chin numbness and paraesthesia in the left anterior part; however, there was no facial palsy. She also complained of head fullness and left eye compressive pain; however, these symptoms progressively improved over 1 week. There was no evidence of recurrence on MRI at the 3-month follow-up.
Discussion
Schwannomas are tumours that grow slowly for a long time without any symptoms. Trigeminal schwannomas are unusual tumours in the head and neck and rarely extend into the parapharyngeal space. 5
It is difficult to resect a giant schwannoma extending from the intracranial space to other regions using a single approach; thus, we should consider dividing the tumour into several parts using clinical images before initiating the operation and design a plan to resect the whole tumour via multiple approaches.
There are various approaches to reach the parapharyngeal space lesions, including transoral, transcervical, transparotid and transmandibular approaches. 9 The surgeon should select the approach based on the tumour size and location and peripheral structures. The transoral approach reportedly increases the risk of complications including nonradical tumour resection, massive bleeding and cranial nerve damage. 12 The transcervical approach is used to access the poststyloid parapharyngeal space and provides a wider surgical view. The transparotid and transmandibular approaches are used to access the prestyloid parapharyngeal space. In this case, the oropharyngeal wall was protruded by the tumour, and the transoral approach was the shortest path. Therefore, we selected the transoral approach for biopsy sampling. Subsequently, we used the transparotid approach to resect the residual parapharyngeal tumour.
There are several approaches to access the medial portion of the middle cranial fossa, such as pterional craniotomy, orbitozygomatic approach, subtemporal approach, endoscopic lateral orbitotomy, endoscopic endonasal approach (EEA) and anterior transmaxillary approach (modified Caldwell–Luc operation). Recently, EEA has been modified to access the skull base with direct and short route of access to the middle cranial fossa tumours. Endoscopic surgery has several advantages, including small craniectomy opening, less temporalis muscle dysfunction and faster recovery. Conversely, endoscopic surgery involves destruction of the normal nasal cavity and risk of cerebrospinal fluid (CSF) leakage.13,14
The best approach to access the tumour remains unidentified. Compared with transmaxillary approaches, including the endonasal endoscopic and modified Caldwell–Luc approaches, endoscopic lateral orbitotomy has the advantage of allowing operative access to the medial portion of middle cranial fossa because of its entry angle from the front to back and from the lateral to medial sides. The entry angles in the transmaxillary approach are from the bottom to up and from the lateral to medial sides. This approach provided a better operative access to the lateral portion of medial cranial fossa. The endoscopic endonasal transmaxillary approach is limited by the maxillary structure to approach Meckel’s cave. The anterior transmaxillary approach allows a wider manipulation field (Figure 3).15,16 Preoperative plan: The green lines indicate the range of the lateral orbitotomy approach; the lateral part of the tumour could not be accessed. The orange lines indicate the range of the anterior transmaxillary approach. The yellow lines indicate the range of the endonasal transmaxillary approach.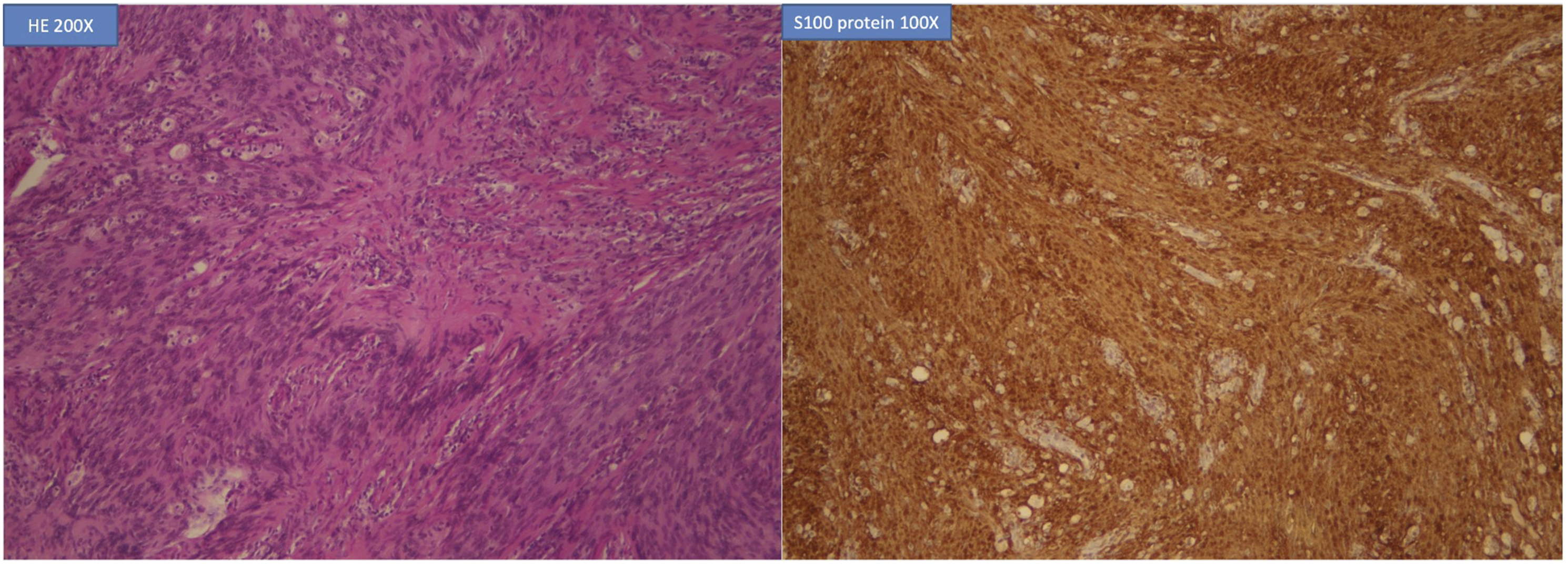
In our case, the tumour arose from the mandibular branch of the trigeminal nerve and was located on the lateral side of the Meckel’s cave. We selected the transmaxillary approach. We started with using EEA; however, the tumour was located in the medial portion of the middle cranial fossa and the lateral side of the Meckel’s cave, which may block the path of the transpterygoid approach to the tumour. We attempted to use the anterior transmaxillary approach with canine fossa trephination to access and resect the tumour.
Trigeminal schwannomas rarely extend to multiple regions as seen in our case. An integrated plan must be designed on the basis of the preoperative images, including MRI and CT scans. This will help find the best and shortest path to access the tumour with a maximum operative field and minimal complications.
Conclusion
We presented the case of a patient with a trigeminal schwannoma extending from the middle cranial fossa through the foramen ovale to the parapharyngeal space and the deep lobe of the parotid gland. We divided the tumour into 3 parts using the images. We used the transoral approach to access the parapharyngeal space; the transparotid approach to remove the tumour from the deep lobe of the parotid gland and the endoscopic endonasal transmaxillary approach to intracapsularly excise the medial portion of the tumour from the middle cranial fossa. There was no sign of a CSF leak; however, the patient complained of left face paraesthesia, head fullness and left eye compressive pain. These symptoms were relieved 1 week postoperatively. Furthermore, there was no obvious sign of residual or recurrence at the last follow-up.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.