
Abstract
Venous malformations (VM) are slow-flow vascular lesions that result from morphogenesis errors. Composed of dysfunctional veins lacking smooth muscle cells, VMs grow slowly and may initially be managed by observation. Treatment is indicated for lesions that cause functional impairment. One treatment option is laser therapy, which is very effective due to its tissue penetration and relative selectivity. The Nd:YAG laser has been shown to treat small and moderately sized mucosal vascular lesions; in this case, it was applied in a staged approach for treatment of a massive venous malformation of the tongue. A 66-year-old male presented with a venous malformation involving the tongue and lower lip, the lesion estimated to be 10 x 14 x 15 cm in size. The Nd:YAG laser was used in three separate stages to photocoagulate the venous lesion. Follow-up for recurrence is ongoing, but currently shows complete malformation ablation with a 36.2% volume reduction after treatment. The Nd:YAG laser is an effective tool in the treatment of large vascular lesions. Successful laser application in a staged approach for the treatment of a venous malformation of this size and complexity further supports its clinical value. Monitoring for possible recurrence of the venous malformation should be ongoing.
Keywords
Introduction
Vascular anomalies, as classified in 2018 by the International Society for the Study of Vascular Anomalies (ISSVA), consist of tumors and malformations. Vascular malformations are divided into slow and fast flow. Slow flow types include capillary, venous, and lymphatic malformations. 1 Although both vascular tumors and malformations first appear in childhood, malformations do not spontaneously involute. 2 The true incidence of venous malformations (VM), which represent a defect in vascular morphogenesis, is unknown but estimated to be approximately 1 in 10,000. 3
Most VMs are sporadic, single, and located in the head and neck region. Almost all involve the skin, mucosa, or subcutaneous tissue. An implicated mutation is a loss-of-function mutation in angiopoietin receptor gene TIE2/TEK, on chromosome 9p. 3
VMs are diagnosed clinically, and larger lesions may be further characterized with imaging. While some VMs can be observed, treatment is indicated with symptoms of pain, bleeding, functional impairment, and for lesions proximal to vital structures. 2 A variety of treatment options exists and includes sclerotherapy, surgical resection, and laser.
Sclerotherapy involves sclerosant injection directly into the malformation. Risks include damage to surrounding structures and diffuse sclerosant distribution in the systemic circulation. 2 Surgical resection is another treatment course and includes risks of iatrogenic injury, blood loss, and deformity.
Laser therapy has significantly less complications compared to other modalities and is implemented as the main VM treatment. Laser therapy specifically photocoagulates vascular lesions since the absorption of laser photons in hemoglobin-selective. 4 The neodymium: doped-yttrium-aluminum-garnet (Nd:YAG) laser has wavelength of 1064 nm, penetration depth of 1.0mm, and demonstrates photocoagulation depth of 7–10mm. 5 With photocoagulation-induced hemostasis, this laser causes little edema or bleeding and serves as an effective therapy of mucosal VMs. Complications are rare and include scarring, tissue necrosis, and dyspigmentation. 4
Case Report
A 66-year-old male with chronic massive tongue enlargement and expansion of the lower lip presented for airway evaluation prior to an orthopedic procedure (Figure 1A and 1B). Per the patient, the enlargement was first noted as an adolescent and had been present for many years. It grew gradually but had been stable since 2007. The patient was unable to fully close his mouth due to tongue protrusion but denied pain, difficulty breathing, or speech or swallowing problems. Past medical and family histories were unremarkable for cancer or similar conditions. On exam, the patient exhibited dysarthria. A large, lobulated bluish mass on the tongue prevented complete closure of the oral cavity. Lesion borders were well defined with no surface ulceration. CT imaging from an outside facility in 2019 identified the size of the lesion as 10 x 14 x 15 cm with noted mandible atrophy and obliteration of the left parotid. (A) Patient presented initially for pre-operative airway evaluation with intubation concerns. (B) Clinical image shows patient attempting to close mouth, with the tongue malformation obstructing complete closure of oral cavity. (C) Three-month follow-up after third stage of treatment with the Nd:YAG laser. (D) Three-month follow-up visit, image shows patient closing mouth. Lower lip continues to be monitored for healing, with future left lip wedge resection planned if reshaping does not occur.
The patient had previously been diagnosed with VM, and records showed a 2007 angiogram performed in preparation for sclerotherapy. At that time, the patient decided against treatment due to concerns of possible complications of the procedure, including tracheotomy and feeding tube. The option of staged laser treatment was discussed, and he was agreeable to consider it.
Serial treatment was performed using Nd:YAG laser wavelength 1064 nm on continuous mode with a power of 15W. The first treatment was a test stage done under local anesthesia due to airway concerns. An area of the right anterior tongue measuring 3 x 4cm was compressed between two glass slides and the Nd:YAG laser was applied in defocused mode. The submucosa was laser coagulated, with no bleeding. Postoperative healing was uncomplicated, and the treated area decreased significantly in size. Seven weeks later, the second stage was performed under general anesthesia. Using the same technique, the entire left-sided tongue lesion was treated resulting in similar size reduction. The third stage was performed eight weeks later under general anesthesia to treat the remaining right side of the lesion. The total energy used was as follows: 3991J, 9756J, and 8172J. At three-month follow-up, the tongue VM appeared completely ablated and the patient’s tongue was reduced to normal size with maintained normal mobility and function (Figure 1C). The most recent CT imaging compared to previous imaging notes a decrease in the size of the extensive venous malformation, supporting clinically apparent ablation (Figure 2A-D). Volumetric analysis of CT imaging data shows a reduction of 7% after the second stage of treatment, with a final volume reduction of 36.2% (from 1464.3 cm3 to 932.9 cm3) at three-month follow-up (Figure 2E-G). Currently, the patient continues to be monitored for remodeling of the expanded lower lip, and future wedge resection is planned if the lower lip remains redundant (Figure 1D). (A-D) Comparison of CT soft tissue neck with contrast imaging at initial presentation (A,C) and at 3-month follow-up (B,D). In the axial view, the pre-treatment scan (A) demonstrates a large, multi-spatial venous malformation with internal phleboliths (small arrows) replacing much of the normal soft tissues of the neck including the left parotid gland (large arrow) and oral tongue (*) with effacement of the airway. The follow-up post-treatment CT scan (B) shows a marked reduction in lesion size, most notably the oral tongue (*) component of the lesion. The sagittal view images pre-treatment (C) and post-treatment (D) support these findings. (E-G) Volumetric analysis of the CT data. Select Axial CT images at the level of the mandibular angle demonstrating the multi-spatial venous malformation: pre-treatment (A), post-stage II treatment (B), and at 3-month follow-up post-treatment(C).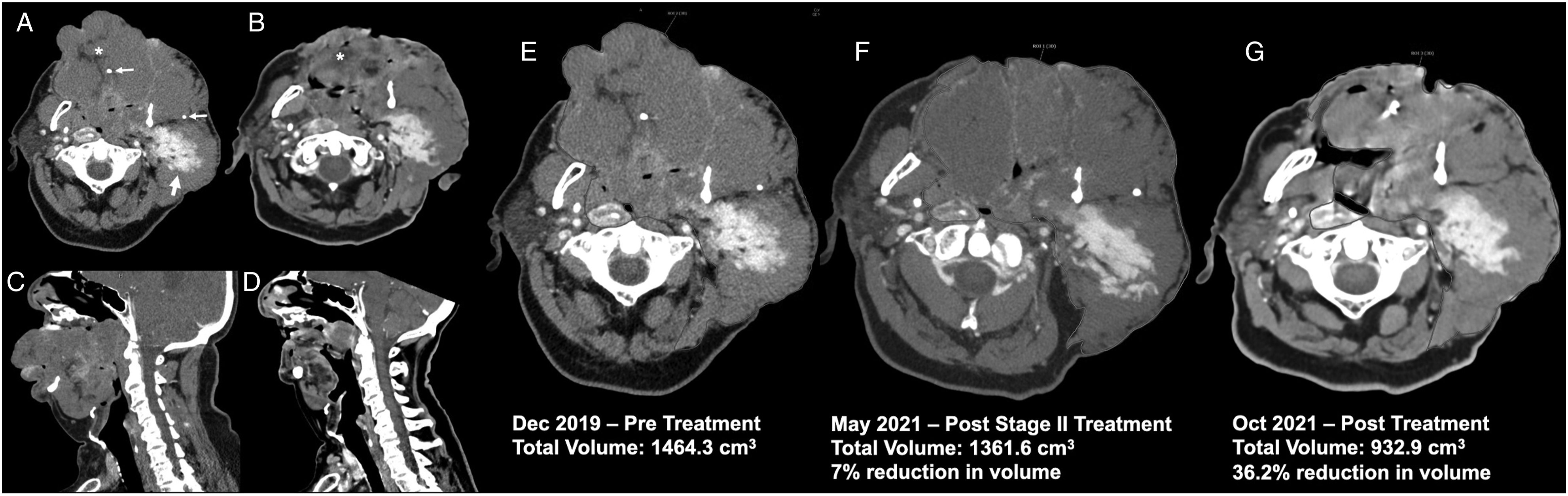
Discussion
Vascular anomalies include tumors and malformations, which are subdivided further into capillary, lymphatic, venous, and arteriovenous malformations. While the therapy options for most anomalies are similar, correct identification of the lesion is critical as the anomalies progress differently. VMs require treatment when they cause functional impairment.
Treatment is based on location, size, and nature of the lesion, but generally includes sclerotherapy, surgical resection, or laser therapy. Compared to other methods, laser therapy offers more advantages with fewer complications. Laser types can be adjusted to tissue characteristics, with specific wavelengths allowing selective photocoagulation and less damage to surrounding structures. Previously, the Nd:YAG laser was effective in single-stage treatments of vascular lesions smaller than 3 x 3 cm.(2,5) Serial application of Nd:YAG laser to this lesion measuring 10 x 14 x 15 cm shows that a staged treatment approach is effective in treating more complex VMs.
Prior to treatment, high-flow VMs must be excluded because feeder arteries would need to be occluded prior to photocoagulation. In this case, a previous cerebral angiogram from previous sclerotherapy preparation ruled out this lesion as high flow.
Although smaller lesions can be treated under local anesthesia, general anesthesia was used in later stages to control intraoperative ventilation and ensure intraoperative analgesia. It is essential that the laser be applied in a defocused mode. The lesion should be observed for shrinkage and blanching with avoidance of gross tissue desiccation and necrosis. The laser beam must be slowly moved over the lesion, without prolonged exposure of any one area. A laser safety margin must be used, as actual photocoagulation may be more extensive than what is visualized. As demonstrated here, an initial test stage in a very large malformation can help gauge response and safely plan further treatment stages.
The Nd:YAG laser has been established as a useful tool for VM ablation. Selective laser photocoagulation better targets the lesion, resulting in fewer complications relative to other available treatment modalities. Demonstrated here is a staged Nd:YAG laser treatment of a 10 x 14 x 15 cm venous malformation for a total volume reduction of 36.2%. This approach is a more effective treatment option for larger and more complex lesions than previously reported.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for publication of this article was received from the Drexel University Libraries Open Access Publishing Pilot Fund.
Informed Consent statement
Written informed consent was obtained from the patient for their anonymized information to be published in this article.