
Abstract
Objective
To characterize the clinical features of patients with congenital hearing loss and unilateral cochlear nerve canal stenosis (CNCS).
Methods
A retrospective review of 12 patients with unilateral CNCS diagnosed between January 2018 and December 2019 at a tertiary referral hospital was performed.
Results
Of the 12 patients identified, there were 6 males and 6 females. All patients presented with hearing loss, with no other chief complaints. Two patients had accessory auricles. Eleven patients had a severe to profound sensorineural hearing loss on the affected side, while 1 patient had an isolated high-frequency hearing loss. Nine patients demonstrated atresia of the cochlear nerve canal (CNC), while three patients had a stenotic, but patent, CNC.
Conclusion
Prompt radiologic diagnosis of patients with unilateral CNCS is important for patient counseling and appropriate rehabilitation.
Introduction
Congenital sensorineural hearing loss (SNHL) is relatively common, with an incidence of approximately 1–2 newborns per 1000. The osseous or bony cochlear nerve canal (CNC) is the area between the modiolus of the cochlea and the internal auditory canal that transmits the cochlear nerve fibers. In a subset of patients with congenital hearing loss, the bony CNC is stenotic. Cochlear nerve canal stenosis (CNCS), first described in 2000, is associated with hypoplasia or aplasia of the cochlear nerve in addition to inner ear malformations. 1 Estimates of the prevalence of CNCS in children with unilateral SNHL are as high as 57%. 2
Computed tomography (CT) of the temporal bones is the preferred radiologic test to diagnose CNCS. A CNC diameter of less than 1.5 mm is generally accepted as stenotic. 3 CT also provides insight into the presence of concomitant internal auditory canal (IAC) stenosis or inner ear malformations, both of which are more common in patients with CNCS. 4 Magnetic resonance imaging (MRI) allows for detection of a hypoplastic or aplastic cochlear nerve on heavily T2-weighted sequences.
Whereas bilateral hearing loss is often detected at the newborn hearing screen or within the first year of life, unilateral pediatric hearing loss, particularly in the absence of robust neonatal screening, can present much later in childhood. Unilateral hearing loss has been associated with poorer speech and language scores in the pediatric population. 5 In this study, we describe our experience with a series of patients with unilateral hearing loss and CNCS presenting at a tertiary academic medical center in childhood.
Case series
Institutional review board approval was obtained (2021-P2-044-01). A retrospective review was performed of patients diagnosed with unilateral hearing loss at a tertiary academic medical center between January 2018 and December 2019.
Inclusion criteria were unilateral congenital hearing loss with radiological evidence of CNCS on the affected ear, defined as a CNC diameter less than 1.5 mm on axial imaging. Exclusion criteria were inadequate radiological examination (both CT and MRI were required) as well as medical comorbidities, such as prematurity, neonatal hypoxia, hyperbilirubinemia, trauma, and meningitis.
Diagnostic tests performed on all patients included pure tone audiometry, acoustic immittance, distortion product otoacoustic emissions (DPOAE), CT temporal bones, and MRI of the brain and IAC without intravenous contrast.
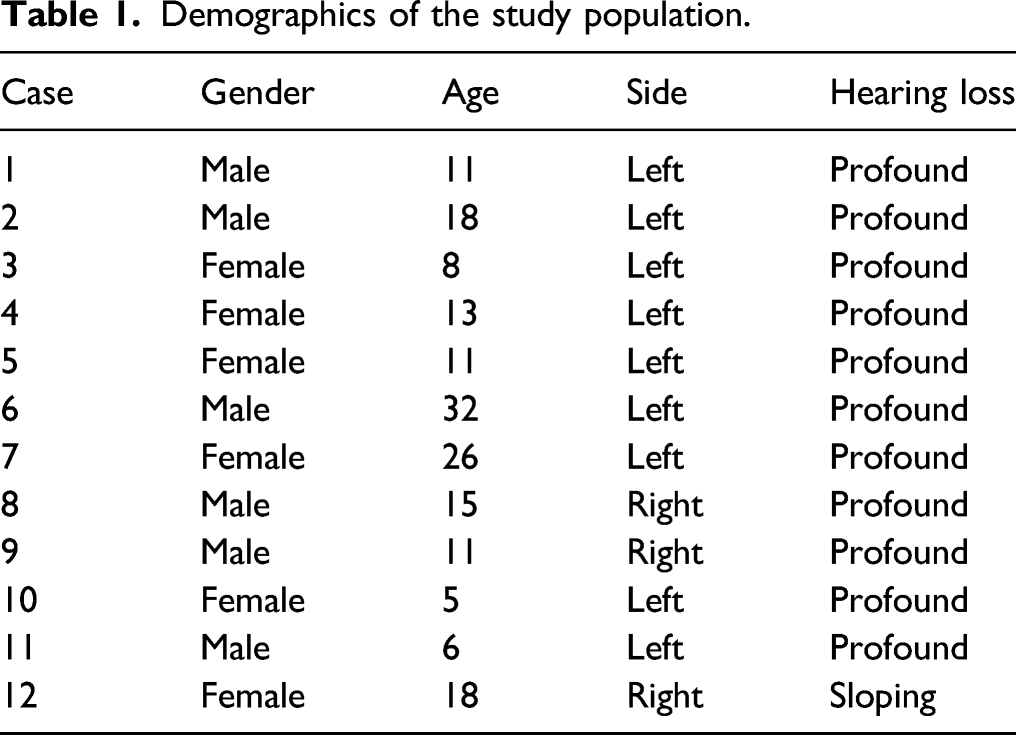
Demographics of the study population.
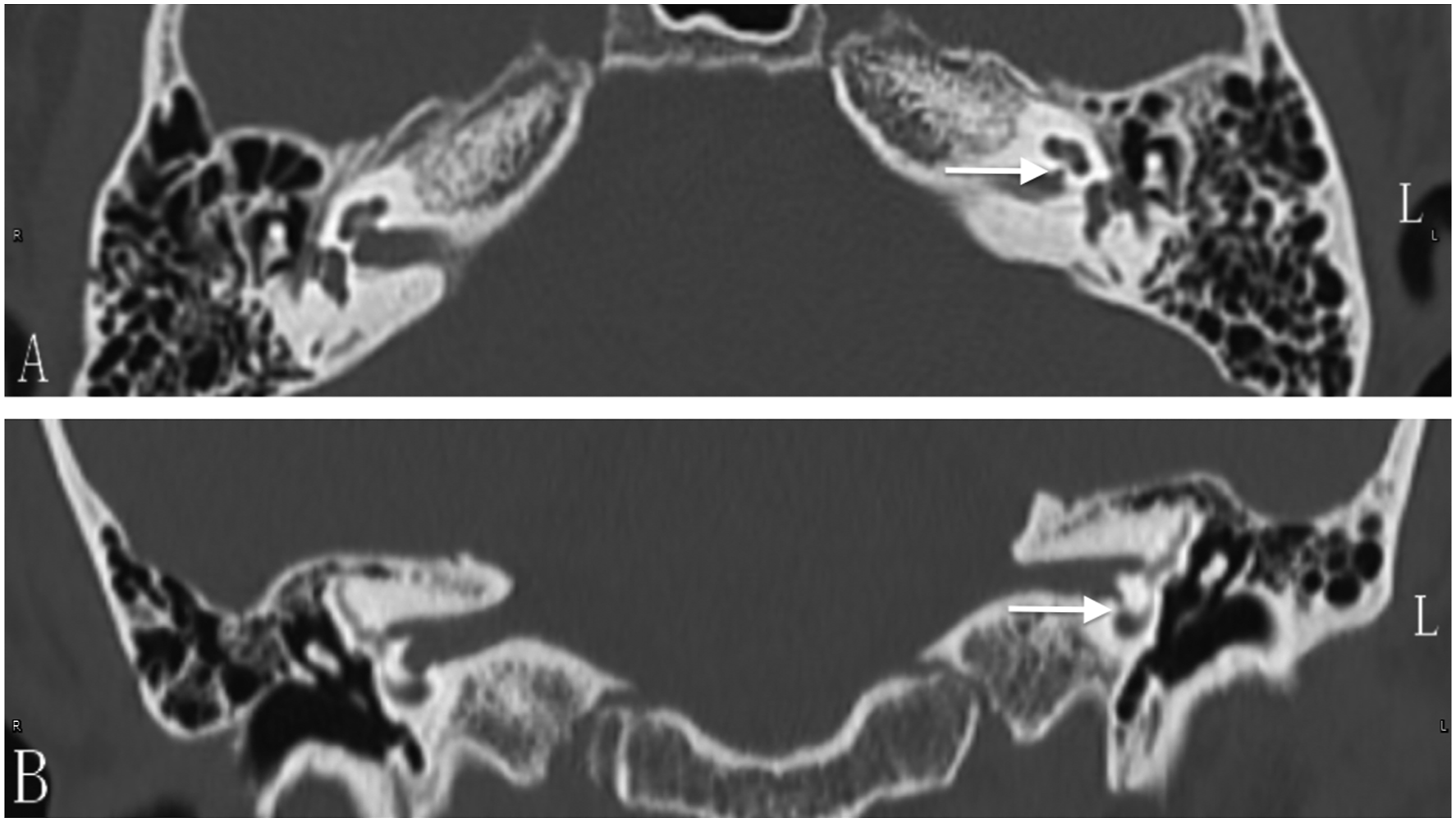
Computed tomography imaging of a patient with left cochlear nerve canal stenosis. A, axial view. B, coronal view. Arrows denote stenosis of bony cochlear nerve canal, seen on the left side only.
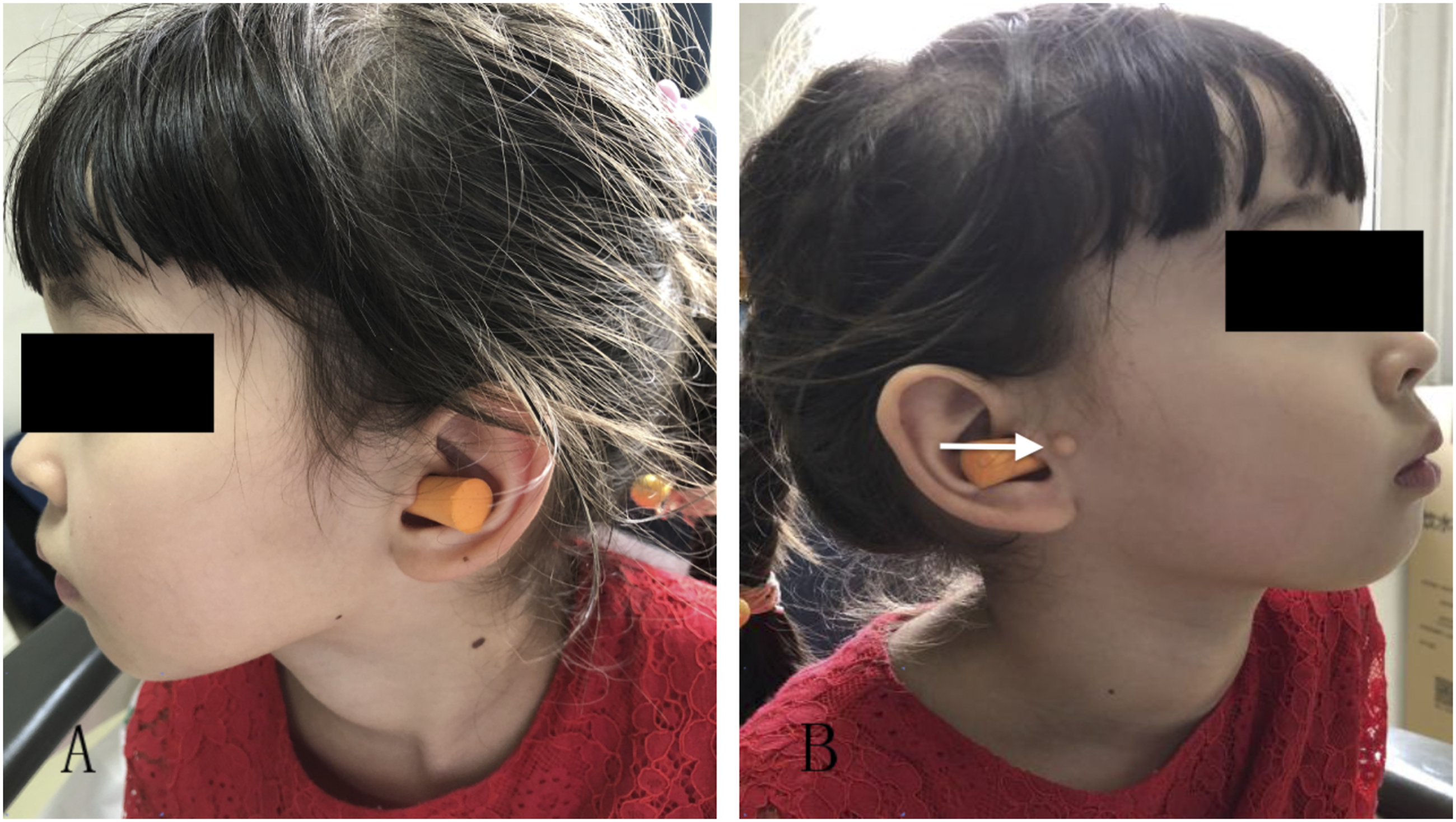
Accessory auricle (arrow) ipsilateral to cochlear nerve canal stenosis; this was observed in two of 12 patients.
Eleven of the 12 cases presented with profound hearing loss across all frequencies in the affected ear; in one case, a sloping audiogram configuration was noted, with low frequency hearing preserved. Acoustic immittance was within normal limits (type A tympanometry) in all affected ears.
DPOAE testing was performed on all subjects. In six patients, DPOAE were absent in the affected ear. In the remaining six patients, DPOAE were present, but the amplitude was diminished. No cases demonstrated normal DPOAE.
The diameter of the CNC was measured in all patients on CT imaging. In 9 patients, atresia of the CNC was seen. In the remaining 3 patients with a patent, but stenotic, CNC, the mean diameter was 1.17 mm (standard deviation, 0.09 mm). Two patients had concomitant IAC stenosis, defined as a diameter less than 2 mm. No abnormalities of the inner ear, middle ear, or external auditory canal were noted in any patient.
MRI imaging, including heavily T2-weighted sequences, was performed in all patients. Sagittal reconstructions were performed to identify the nerves in the IAC. The cochlear nerve was aplastic in 9 patients and hypoplastic in 3 patients (Figure 3). Magnetic resonance imaging of a patient with left cochlear nerve canal stenosis and left cochlear nerve aplasia. A, sagittal reconstruction of left internal auditory canal (IAC) reveals absent cochlear nerve (arrow denotes expected position). B, sagittal reconstruction of right IAC reveals normal anatomy with cochlear nerve in expected anteroinferior position (arrow).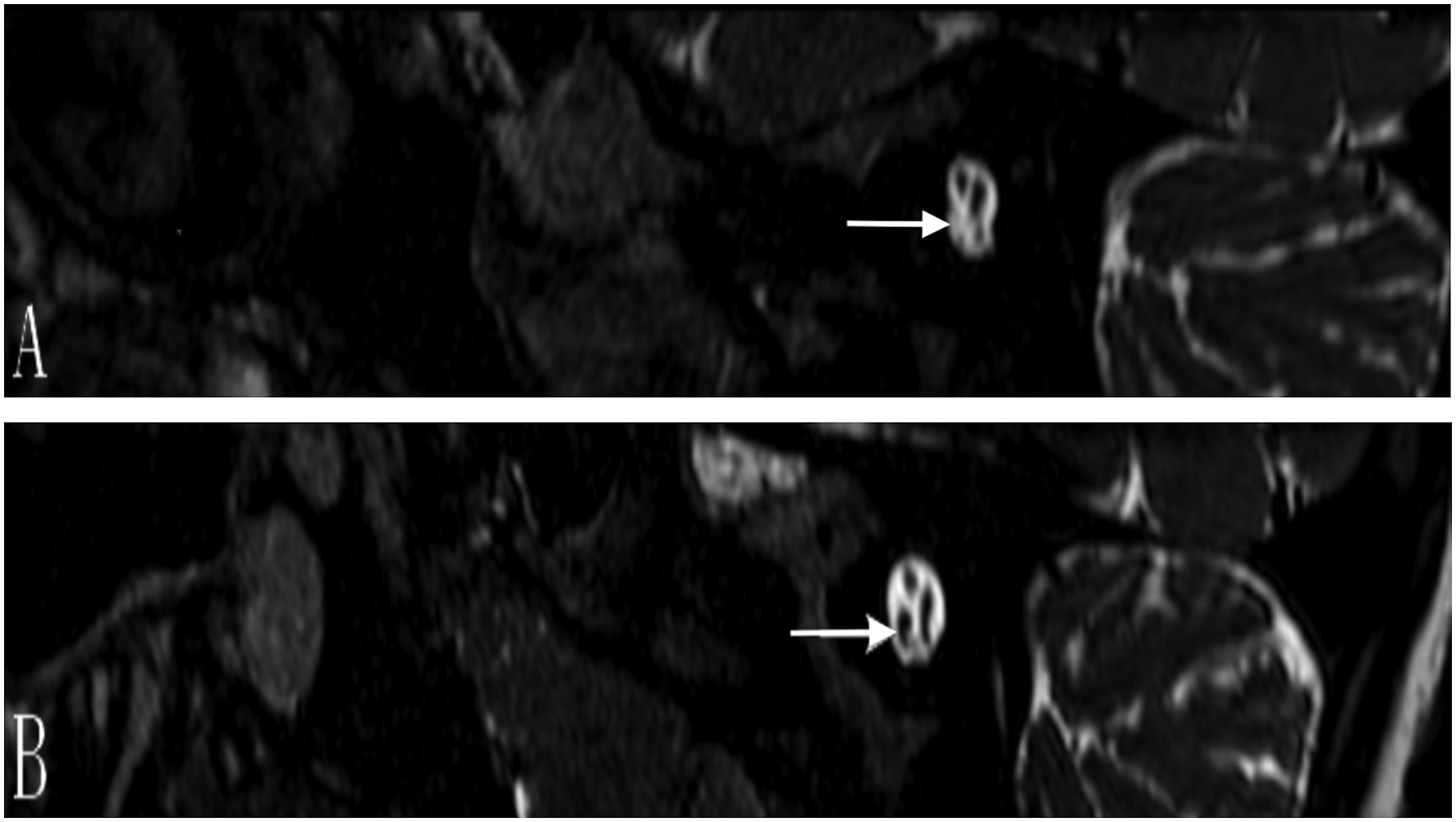
Discussion
Hearing loss is detected in roughly 0.2–0.3% of children at birth, and is as such a relatively common health condition. Unilateral sensorineural hearing loss (SNHL) is more insidious, and, particularly in the absence of robust newborn screening, is often discovered in primary school. If the unaffected ear has normal hearing, the vast majority of these patients develop normal language and speech skills. Still, evidence exists that children with unilateral deafness may demonstrate lower full-scale and performance intelligence quotient (IQ) scores and poorer speech and language skills compared to normal-hearing peers. 5
Unilateral congenital profound hearing loss may arise secondary to genetic factors, inner ear malformations, and perinatal infections, among other causes. The incidence of cochlear nerve deficiency may be as high as 18% among children with congenital sensorineural deafness. First described in 2000, cochlear nerve canal stenosis (CNCS) is highly associated with congenital unilateral SNHL. 1 The incidence of CNCS in this population has been estimated at 52%, which is significantly higher than in children with bilateral deafness. 6 The mechanism by which CNCS occurs has not yet been elucidated. While congenital failure to canalize may seem the most likely explanation, post-developmental degeneration, fibrosis, or scarring are also possible.
Interestingly, in our series, 11 patients had profound hearing loss on the affected ear, but one patient had normal hearing sloping to a profound loss. In cases of CNCS with residual hearing remaining, it has been hypothesized that a diminutive cochlear nerve is present. CNCS has been associated with inner ear malformations in a minority of cases. 3 CNCS has also been associated with syndromic hearing loss, 7 but in our series, zero of 12 patients demonstrated inner ear malformations or a syndromic association with hearing loss. Two patients had an accessory auricle on the affected ear. Perhaps unsuprisingly, cochlear nerve hypoplasia or aplasia is strongly associated with CNCS, with an incidence estimated at around 19% in one series. 3 In our series, 9 (75%) had complete aplasia of the cochlear nerve on MRI, and 3 (25%) demonstrated cochlear nerve hypoplasia.
A recent report described the risk of progression of ipsilateral hearing loss in patients with CNCS. 8 This was less applicable in our cohort, as nearly all patients presented with a profound hearing loss at an average age of diagnosis of 14.5 years, but the possibility of a hearing decline from birth until the time of presentation at our medical center cannot be excluded.
Cochlear implantation is not yet widely performed for pediatric patients with a unilateral profound loss. Nevertheless, the potential for hearing deterioration in CNCS patients to profound levels is an important factor to consider. 8 Furthermore, in this population, cochlear nerve hypoplasia and aplasia need to be taken into account, but it is important to note that certain patients with cochlear nerve hypoplasia and even aplasia derive benefit from cochlear implantation. 9 This may be secondary to the fact that cochlear nerve fibers may travel along other nerves within the IAC. Previous research has suggested that CNCS is associated with higher thresholds on electrocochleography after cochlear implantation, adding to the complexity of cochlear implantation in this population. 10 In our series, no patients underwent cochlear implantation in the affected ear.
One limitation of the study is that neonatal screening results were not available for any subject within the series; correlation of newborn screening results to hearing performance at the time of presentation would be valuable. In China, newborn hearing screen practices vary widely by geographical location: while newborn hearing screening is relatively commonplace in large cities, the same cannot be said of rural settings. In the future, more consistent newborn screening will allow us to understand typical neonatal DPOAE and ABR performance in patients with unilateral CNCS. Future research will also investigate the role of cochlear implantation in patients with CNCS.
Conclusion
Unilateral cochlear nerve canal stenosis most commonly presents as a congenital unilateral hearing loss. Prompt diagnosis is important for optimal audiological rehabilitation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Beijing Municipal Health System Academic Leaders of High-Level Health Personnel Program (No. 2013-3-063).