
Abstract
Hyaluronic acid (HA) is a commonly used injectable material in temporary vocal fold injections (VFI) in patients with unilateral vocal fold paralysis (UVFP). Hyaluronic acid has generally been known for its three–six months of longevity following VFI. Owing to recent advances in cross-linking technologies, the longevity of HA-based materials, including deep-volumizing cross-linked HA used in VFI, has been improved. However, persisting injectable material in the subepithelial space poses undesirable complications following VFI. Herein, we report 2 cases of unexpected persistence of superficially injected cross-linked HA. In the first case, a 70-year-old man with iatrogenic UVFP received VFI with cross-linked HA three years ago and was referred for persistent dysphonia. Previously injected HA spilled out from the vocal fold (VF) when an epithelial incision was made in the subepithelial cystic lesion. In the second case, a 72-year-old woman with iatrogenic UVFP received VFI with cross-linked HA that migrated into the subepithelial space. Diffuse swelling of the injected VF caused dysphonia that lasted for a year. The previously injected HA spilled out when an epithelial incision was made in the swollen VF. Since superficially injected deep-volumizing cross-linked HA can persist for up to three years, laryngologists should be aware of possible sequelae upon suboptimal VFI with cross-linked HA.
Introduction
Since the first vocal fold injection (VFI) was performed with paraffin in 1911, various materials, such as collagen, hyaluronic acid (HA), calcium hydroxylapatite (CaHA), and autologous fat, have been utilized. 1 Hyaluronic acid is a naturally occurring biocompatible polysaccharide without tissue specificity or immunogenicity. 2 Its strong hydrophilic and hygroscopic properties are suitable for volume augmentation of tissues. 2
However, naturally derived HA is short-lived, rapidly absorbed, and easily degradable. 2 Cross-linking is a chemical modification process that improves its physical properties and durability.1,2 The enhanced biostability of HA via cross-linking enables its medical application in soft tissue augmentation.1,2 Commercially available cross-linked HA (XLHA) has been commonly used for temporary VFI with an expected clinical longevity of 3 to 6 months.1-3 However, recent cross-linking technologies have prolonged its longevity. 3
In this case report, we present 2 cases of dysphonia that persisted between one and three years after VFI due to the prolonged longevity of XLHAs. In addition, a literature review was conducted on the cause of persistence of recently developed XLHA following superficial VFI and its treatment policies.
Case Reports
Case 1
A 70-year-old man was referred to our hospital with persistent hoarseness that lasted for more than three years. He had been diagnosed with iatrogenic left vocal fold (VF) paralysis after Ivor Lewis esophagectomy and had undergone VFI with XLHA (Neuramis® Deep Lidocaine, Medytox, Seoul, Korea) due to severe aspiration tendency and dysphonia three years ago. Laryngoscopy revealed a round mass in the left VF (Figure 1A). In acoustic analysis, the maximum phonation time (MPT); fundamental frequency (F0); and jitter, shimmer, and noise-to-harmonic ratio (NHR) were 3.8 s; 287.8 Hz; and 13.4%, 21.9%, and 0.717, respectively. The voice handicap index-10 (VHI-10) score was 36. Preoperative and intraoperative findings of Case 1. (A) Indirect laryngoscopy shows a round mass on the left vocal fold (white arrowheads). (B) Suspension laryngoscopy shows a subepithelial cystic lesion in the anterior portion of the left vocal fold (white arrowheads). (C) A gelatinous material (black arrowheads) spills from the subepithelial space after an epithelial incision. (D) The injectate is completely removed.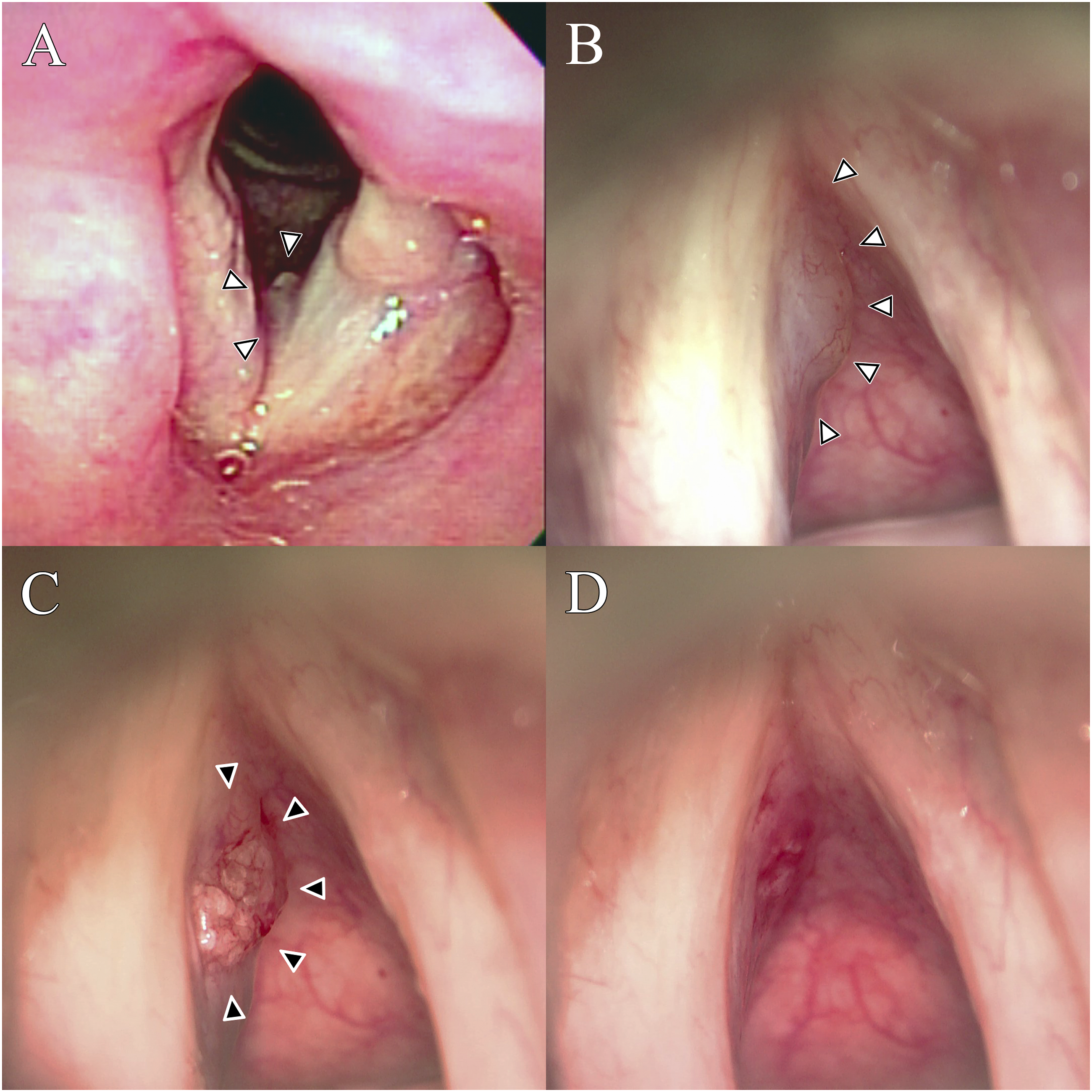
Suspension laryngoscopy revealed a subepithelial cystic lesion in the anterior portion of the left VF (Figure 1B). A gelatinous material spilled from the subepithelial space after the epithelial incision (Figure 1C), and the previous injectate was completely removed (Figure 1D). One month later, an additional outpatient VFI to the left VF was performed with the previously used material via trans-cricothyroid membrane approach. The subjective and objective voice parameters (VHI-10: 3, MPT: 7 s, F0: 131.0 Hz, jitter: 2.4%, shimmer: 7.9%, and NHR: 0.166) showed improvement after six months of the revision VFI.
Case 2
A 72-year-old woman was referred to our hospital with dysphagia after a right hemithyroidectomy. Laryngoscopy revealed an immobile right VF in the paramedian position. Outpatient VFI with XLHA (Perfectha® Deep, Sinclair Pharma, London, UK) was performed using trans-cricothyroid membrane approach. Although the MPT increased from 4.14 to 7.70 s, the subjective voice worsened (VHI: 52 to 112) following VFI. Vocal fold mobility recovered three months after VFI, but subjective dysphonia (VHI: 77) persisted for a year. Subsequent laryngoscopy revealed diffuse swelling in the right VF (Figure 2A). In the acoustic analysis, the MPT, F0, jitter, shimmer, and NHR were 7.4 s, 159.4 Hz, 1.0%, 4.7%, and 0.129, respectively. Preoperative and intraoperative findings of Case 2. (A) Indirect laryngoscopy shows diffuse swelling of the right vocal fold (white arrowheads). (B) Suspension laryngoscopy shows diffuse subepithelial bulging in the right vocal fold (white arrowheads). (C) Previous injectable material (black arrowheads) spills from the subepithelial space after an epithelial incision. (D) The injectate is completely removed until the right vocal fold edge is straightened.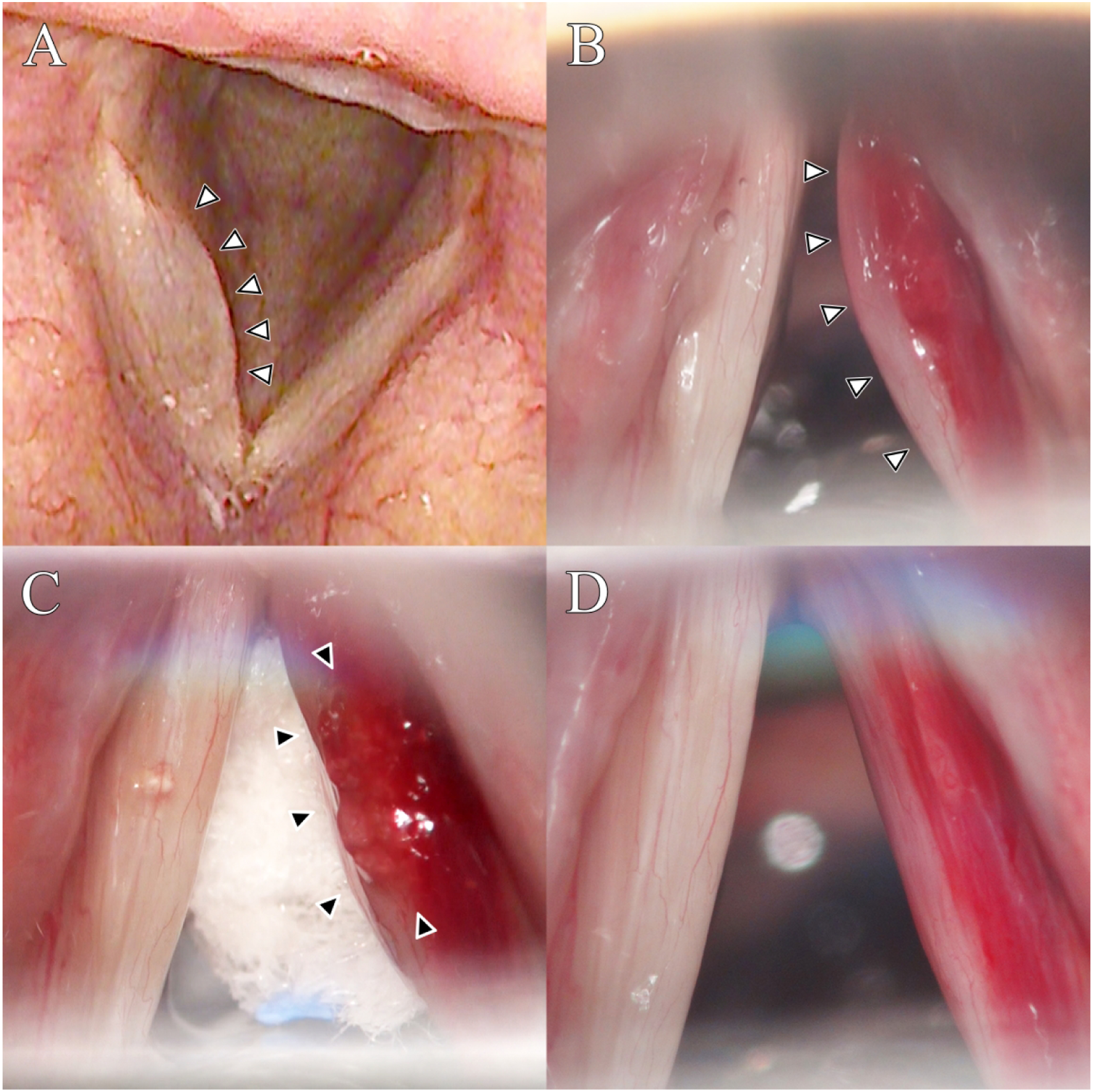
Suspension laryngoscopy revealed subepithelial bulging of the right VF (Figure 2B). The previous injectate spilled from the subepithelial space after the epithelial incision (Figure 2C). The remaining injectate was gently removed using microflap technique until the right VF border was straightened (Figure 2D). The subjective and objective voice parameters (VHI: 31, MPT: 11.8 s; F0: 178.0 Hz; jitter: 0.6%, shimmer: 4.0%, and NHR: 0.139) showed improvement after six months.
Discussion
This case report presents 2 cases of prolonged persistence (>1 year) of XLHA in the subepithelial space after VFI. One patient had a persistent injectate for up to three years following VFI. Such persistence of XLHA is unprecedented, and it is the longest reported longevity of XLHA after VFI till date. Both the subjective and objective voices of the patients improved after the surgical removal of the remaining XLHA.
Persistence of the injectable material in the subepithelial space is an undesirable complication after VFI. 4 Superficial injection of highly viscous permanent materials, such as CaHA, results in decreased VF viscoelasticity and severe dysphonia. 1 Immediate removal of CaHA is the recommended treatment.1,4,5 Although a few reports have shown worsening of VF vibration after superficial injection or overinjection of HA-based materials,4,5 its management has not been discussed thoroughly. Three potential options have been suggested to treat the ensuing complications of superficial HA injection—“wait and see,” 4 hyaluronidase, 5 and surgical removal. 5 In both of our cases, surgical removal was performed and voice improvements were achieved six months after the treatment. Our results suggest that unlike CaHA, superficially injected XLHA can be safely removed even after three years without permanent voice deterioration.
Because all HA-based materials used in VFI were initially developed as dermal fillers, recent improvements in HA-based injection materials have focused on overcoming their short longevity. Recent advancements in cross-linking technologies have enhanced the longevity of XLHAs. 6 Although these materials seem similar, their mechanical, rheological, and clinical stabilities differ with the proprietary cross-linking technology, thereby providing distinct longevities for each material.1,2,7,8 Among these properties, the most important factor is elastic modulus (G`), which affects gel firmness or ability to lift tissue. 2 Products with high G` are more resistant to deformation due to applied stress and are highly viscous, resulting in increased longevity. 2 Consequently, low G` materials are usually utilized for fine lines and wrinkles, while high G` materials are better suited for deeper tissue elevation. 2 Based on physical properties, commercially available XLHAs are categorized into superficial, midlevel, or deep-volumizers according to their respective indicated depth of use.
Hyaluronic acid is widely known as a temporary VFI material.1,5 However, a recent study on the longevity and effectiveness of deep-volumizing XLHA (Juvederm®) used in VFI showed a mean longevity of 10.6 months. In addition, HA is ideal for medial mucosal injection (or subepithelial injection into Reinke’s space) due to its potency to preserve the mucosal wave and to reduce phonation threshold pressure.9,10 However, Kimura et al. reported that the viscoelasticity of Juvederm®, along with CaHA and other collagen materials, was higher than that of the normal VF. 11 The superficially injected deep-volumizing XLHA in our cases (Neuramis® Deep Lidocaine and Perfectha® Deep) had high G`, resulting in deterioration of normal VF vibration and its prolonged persistence in the subepithelial space even after three years. Moreover, prolonged longevity of deep-volumizing XLHAs has been reported in various anatomical sites, with persistence ranging from 24 to 40 months.12-14 In an animal model, Sheptulin et al. suggested that neocollagen synthesis and lack of hyaluronidase activity can explain the unexpected HA persistence. 14 Further studies on different anatomical distributions of HA and hyaluronidase at the VF subsites are required to verify our observations.
In conclusion, contrary to the established temporary nature of HA, prolonged persistence of deep-volumizing XLHA for up to three years was observed following its injection into the subepithelial space. Although delayed surgical removal restored the voice profiles of our patients, there is no doubt that the sequelae of superficial XLHA injection may cause distress for both laryngologists and patients. Hence, laryngologists should be meticulous in implementing VFI in the subepithelial space when using deep-volumizing XLHA.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by the National Research Foundation of Korea grant funded by the Korean government (Ministry of Science and ICT), grant number 2021R1F1A1062700. The funder had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Ethical Approval
Ethical approval to report this case was obtained from the Institutional Review Board (IRB No. SC20ZISE0109) of the Yeouido St. Mary’s Hospital, The Catholic University of Korea.
Human and Animal Rights
All procedures in this study were conducted in accordance with the Institutional Review Board (IRB No. SC20ZISE0109) of the Yeouido St. Mary’s Hospital, The Catholic University of Korea. This study was conducted in accordance with the World Medical Association Declaration of Helsinki.
Informed Consent
The requirement for written informed consent was waived by the IRB owing to the retrospective nature of this study.