
Abstract
Objective
To examine associations of laboratory and imaging data with diagnostic parameters of necrotizing otitis externa (NOE) and its severity, and to compare between bacterial and fungal infections.
Methods
Records of patients diagnosed with NOE during 2010–2018 at the Department of Otolaryngology, Head and Neck Surgery were reviewed retrospectively for demographics; disease characteristics; and laboratory, scintigraphy, and imaging results.
Results
Of 48 patients with NOE, the mean age is 73±11.6 years; 32 (67%) were males; 83% had diabetes mellitus. Common pathogens were pseudomonas (49%) and fungi (33%). Sensitivities of the technetium-scan (SPECT ratio ≥1.5), temporal bone computed tomography (CT), and gallium-scan (SPECT ratio ≥1.3) were: 78.7%, 48.8%, and 31.4%, respectively. Gallium-scan results correlated positively with CT bone involvement (p=0.002) and hospital length of stay (p=0.0014). C-reactive protein (CRP) level correlated with hospital length of stay (p=0.028) and positive technetium-scan results (p=0.012). Fungal infection had a higher technetium SPECT ratio (2.16 vs. 1.77, p=0.04), gallium SPECT ratio (1.4 vs. 1.2, p=0.02), longer duration of systemic treatment (87.4 vs. 37.9 days, p=0.014), and longer hospital length of stay (31.6 vs. 15.2 days, p=0.004) compared to non-fungal infection. Eight (17%) patients had responded poorly to treatment. Fungal pathogens, facial nerve paresis, extra-auricular, and bilateral disease were more prevalent among the non-responders.
Conclusion
The technetium scan has higher sensitivity than temporal bone CT for diagnosing NOE. The gallium scan and CRP correlated well with hospital length of stay. A high rate of fungal infection was found, with significantly higher technetium and gallium SPECT ratios and worse outcome compared to bacterial infection. Fungal NOE remains therapeutically challenging.
Keywords
Introduction
Necrotizing otitis externa (NOE) is a severe infection of the external auditory canal, defined as osteomyelitis of the temporal bone. The majority of those affected are immunocompromised, typically with diabetes.1,2 Symptoms include severe otalgia, otorrhea, and aural fullness. The common otoscopic findings are discharge, edema, and granulation tissue; however, these do not always present.1-3 Laboratory studies are not specific, nor are histopathologic features of the granulation tissue removed from the ear canal. 1 Due to the difficulty in differentiating NOE from other types of otitis externa, diagnosis is frequently delayed, thus extending the duration of treatment, and impairing prognosis and outcome. Verifying the response to treatment can be challenging and is based on pain relief, recovery of otoscopic findings, and improvement in laboratory values.3,4
Various imaging modalities are commonly used to confirm the diagnosis of NOE and to assess the response to treatment. 4 Nuclear scans are not frequently used due to non-specificity and poor anatomic and spatial detail compared to CT and magnetic resonance imaging (MRI).4-6
For decades, the combination of technetium (Tc) and Gallium (Ga) scans was shown to be more sensitive and specific for diagnosing NOE than any other test; however, their prognostic value was poor. 7
Our main objectives were to examine associations of laboratory and imaging data with diagnostic parameters of NOE and its severity, and to compare characteristics of patients with bacterial and fungal NOEs. In addition, we conducted a subgroup analysis of patients who had no response to treatment.
Patients and methods
This is a retrospective study of patients diagnosed with NOE in the Department of Otolaryngology, Head, and Neck Surgery at Carmel Medical Center during 2010–2018.
The study was approved by the institutional Helsinki board. We evaluated underlying medical conditions such as diabetes mellitus, laboratory results (C-reactive protein [CRP] and white blood cell [WBC] count), isolated pathogens in cultures, hospital length of stay (LOS), and total duration of systemic treatment until resolution of the disease. In addition, we analyzed the Tc and Ga SPECT ratios and their correlations to bone involvement on CT scan. A CT scan was considered positive when temporal bone erosion was noticed, mainly destruction of the bony external ear canal. We evaluated associations of each parameter with disease severity, hospital LOS, and duration of treatment.
We compared between patients with bacterial and fungal NOE: Tc and Ga SPECT ratios, LOS, and duration of treatment. We also conducted a subgroup analysis of patients who had responded poorly to treatment.
Statistical analysis
We used the JMP Statistical Discovery 14 software (SAS Institute Inc., Cary, NC, USA). All the parameters were analyzed for normal distribution. Correlations between variables were done using the Pearson`s and the Spearman`s coefficients of correlation, for parametric and non-parametric groups, respectively. Univariate analysis of the measured variables was performed and statistical significance between subgroups was tested using the Log-Rank test. Multivariate analysis was performed for hospital LOS and response to therapy. For all analyses, p <0.05 was considered significant.
Results
Characteristics of patients with necrotizing otitis externa (N=48).
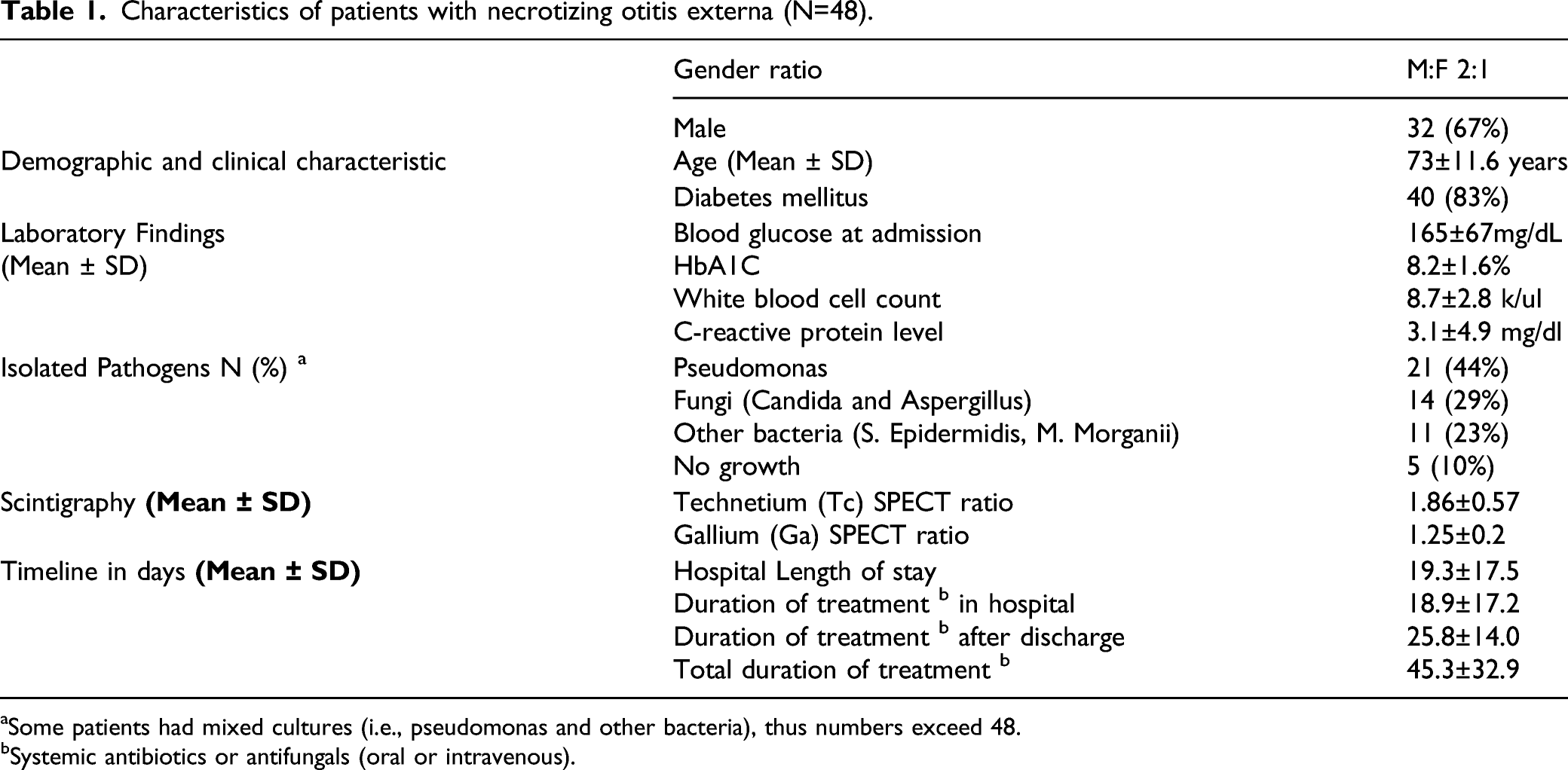
Some patients had mixed cultures (i.e., pseudomonas and other bacteria), thus numbers exceed 48.
Systemic antibiotics or antifungals (oral or intravenous).
Imaging Parameters
The imaging modalities used for diagnosis and follow-up were CT scan of the temporal bone (43 patients), Tc scan (47 patients), Ga scan (35 patients), and MRI (2 patients).
Sensitivity of imaging modalities for the diagnosis of necrotizing otitis externa.
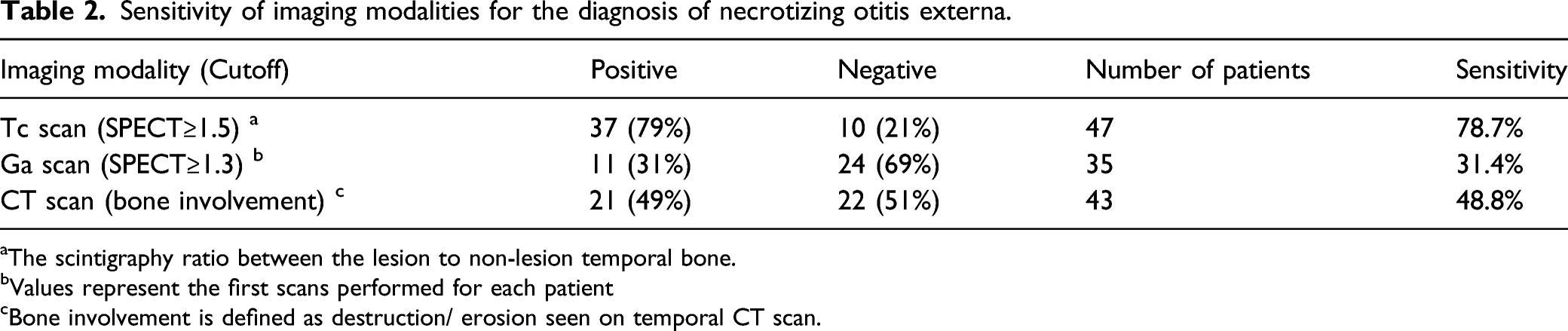
The scintigraphy ratio between the lesion to non-lesion temporal bone.
Values represent the first scans performed for each patient
Bone involvement is defined as destruction/ erosion seen on temporal CT scan.
A CT scan showed bone involvement in 21 of 43 patients (49%). Thirteen of these (30%) showed extra-auricular involvement of their disease, namely, temporomandibular joint (3 patients) and mastoid involvement (3 patients).
The diagnosis of NOE in our study was based on CT, Tc, and Ga scans for 32 patients, Tc and CT scans for 10 patients, Tc and Ga scans for 3 patients, Tc only for 2 patients, and CT only for 1 patient.
The Tc scan had the highest sensitivity (79%) for diagnosing NOE. The Tc scan was positive in 17 (34%) patients who showed no bone involvement in the CT scan. In univariate analysis, a positive Tc scan (SPECT ≥ 1.5) did not correlate significantly with bone involvement on CT, LOS in the hospital, the duration of total systemic treatment, and response to therapy. However, Tc scan results correlated linearly with the duration of systemic treatment after hospitalization (p = 0.014, F = 6.4). A positive Ga scan (SPECT ≥ 1.3) correlated well with bone involvement on CT (p = 0.004) and hospital LOS (p = 0.0014) Correlation between Ga scan (SPECT ≥ 1.3) and hospital length of stay. The total duration of hospitalization (days) = 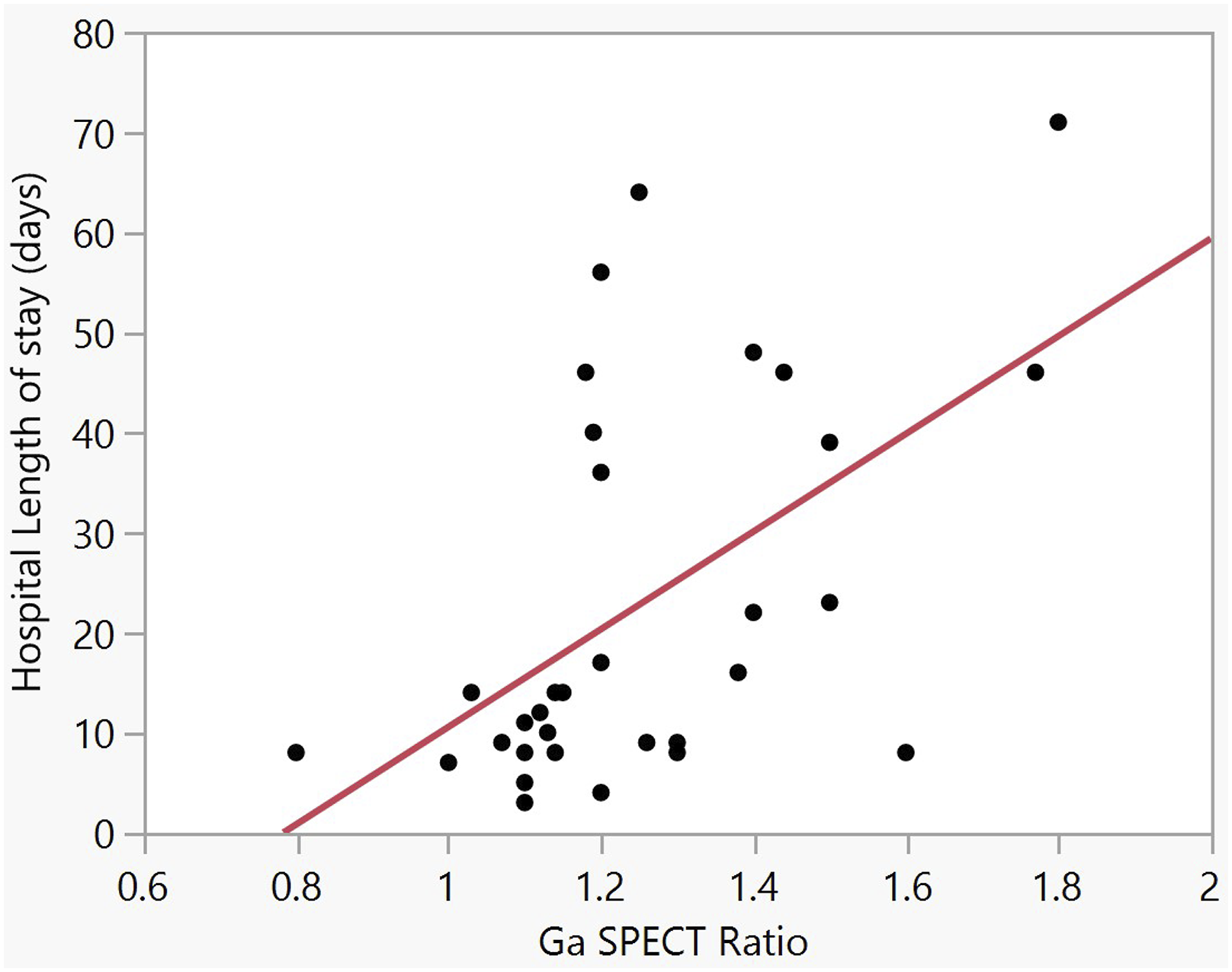
The correlation between Ga scan and the total duration of systemic treatment in the hospital and following discharge was not statistically significant (p=0.08). No significant correlation was found between a positive Tc scan and a positive Ga scan.
Laboratory Parameters
CRP level was found to be significantly associated with NOE. We found a positive correlation between CRP level and Tc SPECT ratio (p = 0.012, F = 6.9) (insert Figure 2). Similarly, CRP correlated well with hospital LOS (p = 0.028, F = 5.2). In a multivariate analysis, CRP level (p=0.07) and positive Ga scan (p=0.0068) were both associated independently with LOS. Correlation between C-reactive protein (CRP) level and Tc SPECT ratio. CRP = 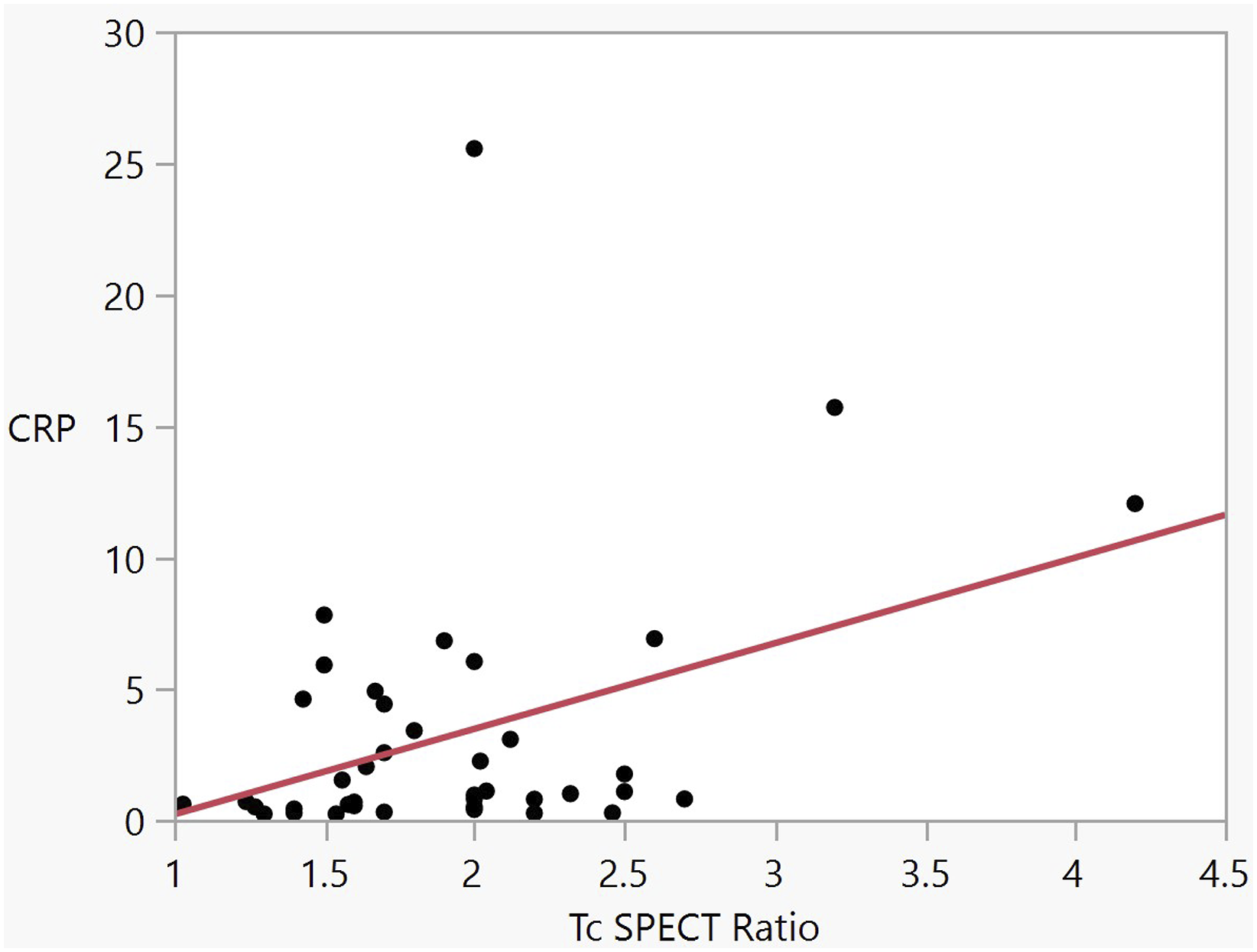
Other laboratory findings of the cohort are presented in Table 1.
Response to treatment
All the patients were treated with systemic antibiotics, mostly ciprofloxacin; the mean duration of treatment was 37.9±18.1 days. Fourteen patients (29%) were treated with systemic antifungal therapy, mostly voriconazole; the mean duration of treatment was 87.4±37.2 days.
Characteristics of patients with necrotizing otitis externa, according to response to treatment.
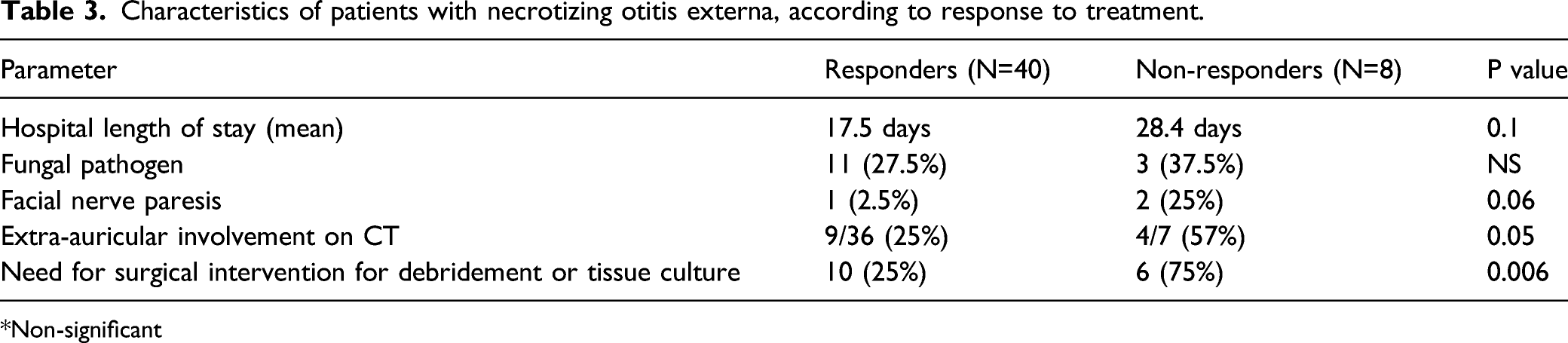
Non-significant
Three patients had facial nerve paresis during the course of the disease. Their mean hospital LOS was 46±10 days (compared to 17.6±16.4 days for patients without facial nerve paresis, p = 0.005), and the mean duration of treatment was 89.3±11.9 days (compared to 42.3±31 days for patients without facial nerve paresis, p = 0.015).
Termination of therapy was determined by a combination of symptoms resolution (mainly pain), improved physical findings (resolution of secretion and granulation tissue), and decreased CRP levels. To a lesser extent, imaging was used to determine response to treatment. Ga scan was repeated for 3 patients (8.5%) after a mean of 47 days from hospital admission, 1 of them was positive (SPECT 1.5) and did not respond to initial therapy.
Tc scan was repeated for 2 patients (4.2%) after a mean of 92 days from hospital admission, 1 of them was positive (SPECT 2.2) and did not respond to therapy. CT scan was repeated for 6 patients (12.7%), after a mean of 39 days. Four of them had bone involvement which was not shown in the first CT scan, and 3 patients did not respond to therapy.
Compared to the responders (n = 40), for the non-responders (n = 8), proportions were higher for hospital LOS, fungal pathogens, facial nerve paresis, bilateral ear disease, extra-auricular involvement on CT, and the need for surgery for debridement or culture (Table 3).
None of the following parameters was associated with response to therapy: Ga and Tc SPECT ratios, WBC count, CRP, glucose level at hospital admission, and HbA1c level.
Fourteen patients (29%) were found to have fungal infection. Compared to patients with non-fungal NOE, patients with fungal NOE had a higher Tc SPECT ratio (2.16 vs. 1.77, p = 0.04, F = 4.5), a higher Ga SPECT ratio (1.4 vs. 1.2, p=0.026, F=5.5) Correlation between Ga Scan and fungal necrotizing otitis externa (NOE). The box-plot shows the median values of the gallium SPECT ratio of the fungal and non-fungal NOE groups. The whiskers show the interquartile range. (P=0.02) Clinical parameters compared between patients with fungal and non-fungal necrotizing otitis externa.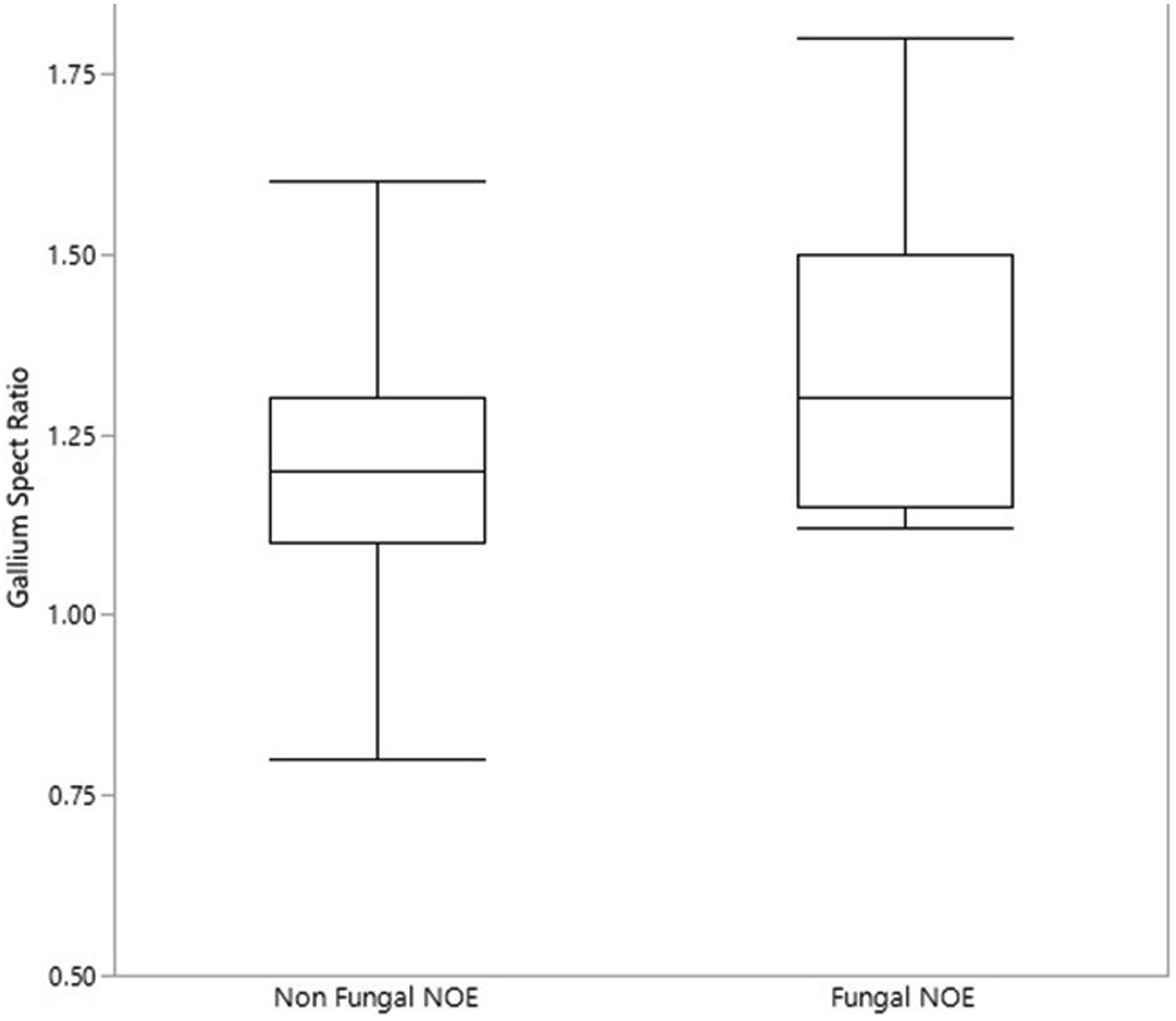

Discussion
The main finding of this retrospective cohort study is the associations of Tc and Ga scan studies with diagnostic and outcome parameters. In addition, we report a high rate of fungal infection and significant differences in nuclear imaging characteristics between those with fungal and non-fungal infections. We quantified scintigraphy SPECT ratios for diagnosing NOE. Fungal NOE showed worse outcomes than bacterial NOE. Overall, a substantial proportion of patients (17%) responded poorly to treatment, and prognostic factors to characterize this group are yet to be identified.
This study demonstrated various correlations of each of three imaging modalities to diagnosis and outcomes of NOE. This is consistent with the lack of consensus in the literature regarding the best imaging modality for initial diagnosis and follow-up of NOE. CT scan has high sensitivity for showing cortical bone erosion at the time of diagnosis. However, bone remineralization continues long after the infection is cured. CT scan was used for 43 patients and its sensitivity for NOE diagnosis was relatively low (48.8%).
Tc-99m bone scanning shows areas of osteoblastic activity and is sensitive for bony infection. Single-photon emission computed tomography (SPECT) provides good anatomic localization and may highlight areas of bony involvement before the CT scan shows structural changes. Ga-67 citrate is absorbed by macrophages and the reticular endothelial cells. In the presence of infection in soft tissue or bone, there is an increased uptake of Ga, which returns to normal after infection has resolved. 9
Tc scan diagnosed NOE in a substantial number of patients who showed no bone involvement on CT scan (17 patients, 35%). However, no correlation was shown between Tc scan and bone involvement on CT scan. This corroborates previously reported findings.4,6
In contrast, the Ga scan correlated better with bone involvement on the CT scan; however, its sensitivity was low (31.4%) for NOE diagnosis (SPECT ratio ≥ 1.3). In addition, the Ga scan correlated well with hospital LOS, suggesting that it may provide a good estimation for prolonged hospitalization.
Summarizing our findings, Tc scan had the highest sensitivity (78.7%) for NOE diagnosis (for SPECT ratio ≥ 1.5) and was positive in 17 (34%) patients with negative CT scan.
Based on these modalities, we suggest the following protocol for NOE diagnosis. Temporal bone CT should be the first imaging modality due to its high availability, if positive should be followed by Ga scan. Negative CT scan should be followed by Tc scan in order to establish the diagnosis or to rule out NOE. Ga scan may be used as an adjunct prognostic tool in any case of NOE diagnosis.
An online survey conducted in the U.S. showed CT scan as the most frequent modality used (37.5%) for diagnosing NOE. 4 Ga scan was most commonly used to assess response to treatment (30.9%), and recommended for initial diagnosis and follow-up tool for NOE.1,2 However, Ga uptake does not always decrease in response to treatment.1,4 Tc scan is highly sensitive for temporal bone osteomyelitis but remains positive long after clinical resolution. In addition, it has lower specificity than the Ga scan and may be positive in simple otitis externa.1,3,4,10 A lesion-to-non-lesion ratio greater than 1.5 in a Tc scan and greater than 1.3 in a Ga scan were shown to have high sensitivity and specificity for NOE detection. 6
Similarly, in the 24/4 SPECT study, the lesion-to-non-lesion count ratio threshold that yielded the best sensitivity for detecting NOE was 1.05. 8
A number of studies based the diagnosis of NOE on the combination of CT, nuclear scans, MRI, and FDG-PET/CT.1,10-12
A recently published meta-analysis did not support the routine use of Tc-99 and Ga-67 in detecting NOE, due to poor specificity, lack of anatomic resolution, unproven ability to detect disease resolution, and variable availability. 7 Correlations were not found between Tc-99 and Ga-67 scans and disease resolution. The gold standard reference for each modality was standard otitis externa which, indeed, may show positive results in nuclear scans. However, the difference between SPECT ratios of standard otitis externa and NOE is still not known. In addition, the studies included in the meta-analysis vary in the number of patients and in the diagnostic criteria of nuclear imaging modalities for NOE. The findings of the current study suggest that Tc and Ga scans may have diagnostic and prognostic value.
Our findings suggest that a combination of imaging modalities rather than a single modality may provide optimal sensitivity and specificity for diagnosis and prognosis. Notably, advantages have been reported for other modalities, such as MRI, for determining the extent of NOE (41.9%); and FDG-PET/CT (PET/CT), for diagnosis and follow-up of NOE.4,10
PET/CT has become a highly specific and sensitive tool for diagnosing axial osteomylitis. 13 In a recent study, the sensitivity, specificity, and positive predictive value of PET/CT in diagnosing skull base osteomylitis were 96.7%, 93.3%, and 98.3%, respectively. 14
To date, PET/CT has been utilized successfully in NOE but in a limited number of patients without a control group. 10 Furthermore, it is still not available for diagnosing NOE in many centers worldwide, as same as in our center.
Future, prospective trials comparing PET/CT to nuclear imaging are necessary to establish its role in the management of NOE.
Our findings confirm the prognostic value of CRP, though this is not specific for NOE. CRP correlated well with Tc SPECT ratio and hospital LOS but not with response to therapy. Higher CRP levels were reported in patients whose admission for NOE was delayed, compared to those admitted early. 15 A correlation between CRP and Tc scan in this context was not previously shown.
Past studies reported that the vast majority (>90%) of isolated pathogens in NOE were pseudomonas and only the minority were fungi.1,4,16,17 In the current study, we observed high rate of fungal pathogens, mainly candida and aspergillus types (29%), and lower rates of bacterial pathogens than reported in the past, mainly pseudomonas (49%). A similar shift was reported by Glikson and others.11,18 A possible explanation is the use of prolonged topical antibiotic treatment prior to the diagnosis of NOE.17,18 The current study shows that nuclear imaging SPECT ratios were significantly higher in fungal in comparison to non-fungal NOE, and it may facilitate the diagnosis of fungal NOE in the absence of bacterial growth.
The mean duration of treatment with systemic antibiotics in our cohort was 37.9 days (5.4 weeks), while the mean duration of systemic antifungal treatment was significantly longer, 87.4 days (12 weeks). Similar rates were reported by others.2,11,16,19,20 The most frequent antifungal agent in our cohort was voriconazole, while other studies reported frequent use of amphotericin B.16,17 For treatment of invasive aspergillosis, voriconazole has shown a better response rate and fewer side effects than amphotericin B. 21
Outcomes differed significantly between patients with fungal and bacterial NOE. Those with fungal NOE had worse outcomes, with higher Tc SPECT ratio, Ga SPECT ratio, and duration of systemic treatment; and longer hospital LOS. The few studies that have compared clinical outcomes of fungal versus bacterial pathogens22,23 did not specify the imaging parameters of each group.
A substantial proportion of our patients (n=8, 17%) responded poorly to treatment and required repeated hospitalizations and prolonged treatment. Compared to patients who responded to treatment, this group had a higher proportion of fungal pathogens and worse outcomes: a higher rate of facial nerve paresis and bilateral disease. However, we did not find significant laboratory or scintigraphy parameters that were associated with response to therapy, other than fungal growth. Antibiotic resistance may partly explain these outcomes. A couple of studies have shown a rising rate of ciprofloxacin-resistant pseudomonas.11,17 Of a cohort of 83 patients with NOE, 24% did not respond to conservative systemic treatment and required surgery. 18 Stevens et al. presented a risk stratification system for severe and non-severe NOE. Similar to our study, higher proportions of those with severe disease had fungal growth, prolonged treatment courses, and relapse. The investigators suggested the following radiographic findings as predictors for severe disease: bone erosion (tegmen, infratemporal fossa, and temporomandibular joint) and intracranial or nasopharyngeal involvement. 22
The limitations of the current study are the retrospective single-center design, small sample size, lack of control group, and limited use of MRI. Since the imaging modalities were interpreted by radiologists in our institute, inter-observer errors may be relevant.
Although NOE is not a rare phenomenon, much is to be learned regarding establishing a treatment protocol. Studies that will compare between imaging modalities of NOE and severe otitis externa are needed, and predictors for response to therapy should be identified.
Footnotes
Author contributions
Margulis Itai, data collection and analysis and preparation of the first draft of the manuscript; Cohen-Kerem Raanan, study design and revision of the manuscript; Roitman Ariel, data collection; Gez-Reder Hadar, data collection and analysis; Aviram Ariel, data collection; Biterman Fisher Sivan, data collection; Kugelman Nir, data collection; Doweck Ilana, study design, data analysis, and revision of the manuscript. All the authors approved the submitted version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was presented as a poster in the annual meeting of the Israeli Society of Otolaryngology, Head, and Neck Surgery, in Eilat, Israel, on February 27, 2020.