
Abstract

Most hemangiomas are benign tumors occurring in the head and neck, which rarely occur in oral cavity structures such as the tongue, lips, and buccal mucosa, and occurrence in the tongue is extremely rare.1,2 In particular, very rarely reported cavernous hemangiomas in children’s tongues. Special attention is needed because the tongue has high mobility; is vulnerable to minor trauma; is highly related to swallowing, respiratory, and anesthesia disorders; and is also cosmetically important. 3 Herein, we present a case of ventral surface midline cavernous hemangioma of anterior tongue in a child.
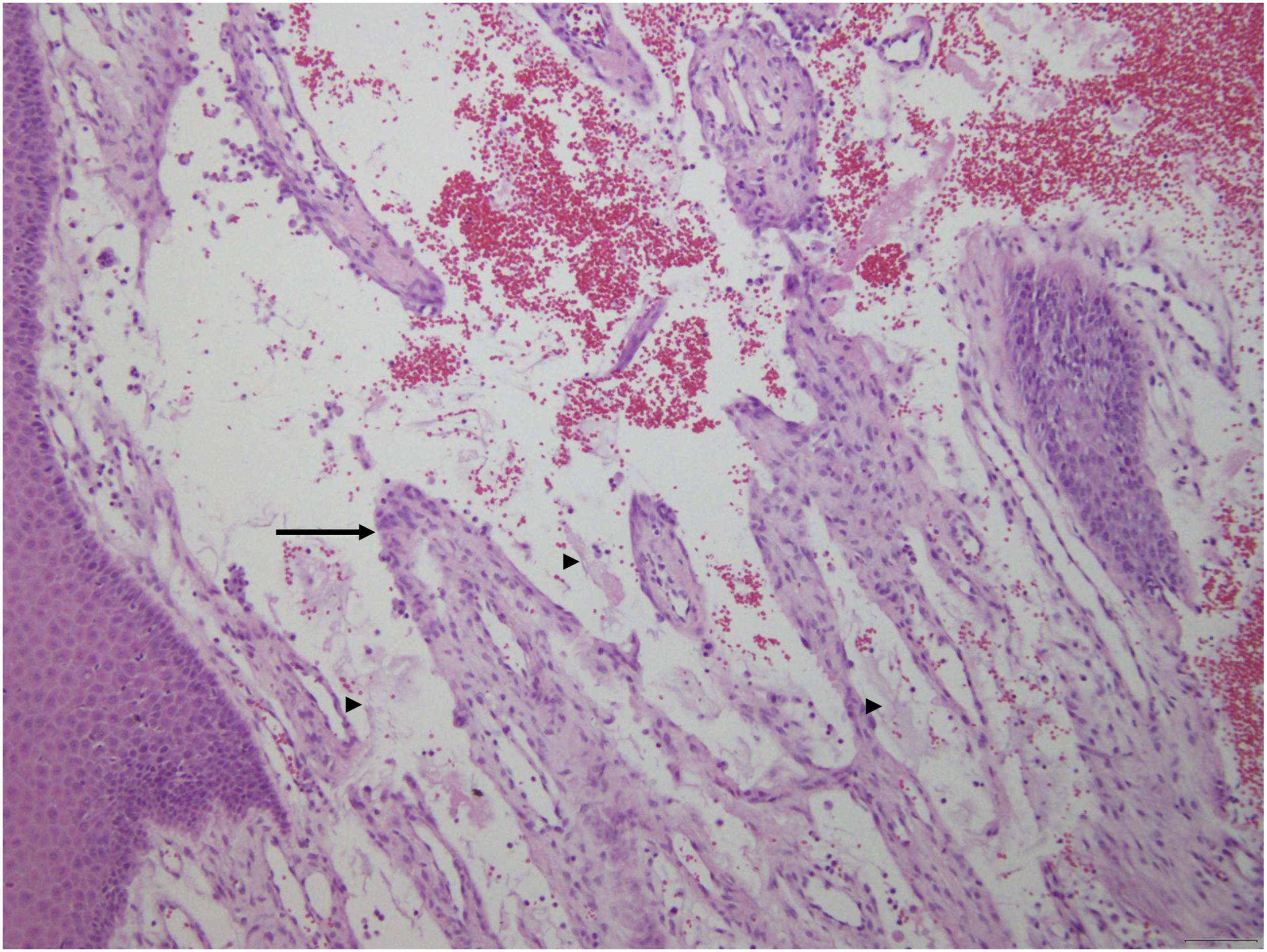
A 6-year-old girl visited our hospital with a protruding ventral surface midline mass on the anterior tongue, which had appeared 3 months prior. The ventral surface of the small tongue mass gradually increased in size from 3 months prior. The patient did not have any underlying diseases, and there were no dietary or developmental challenges other than discomfort due to the mass. Physical examination revealed an approximately 0.7-cm size non-tender, pinkish, smooth-walled, and mildly hard mass on the ventral surface of the tongue, and the patient did not complain of pain upon palpation (Figure 1A). An excisional biopsy was performed under general anesthesia, and the mass had a long diameter (0.7 cm [Figure 1B]). The pathologic report revealed that the mass comprised thin-walled vessels lined with epithelial cells and separated by a thin layer of connective tissue septa (Figure 2). There was well-controlled bleeding at the excision site, and the patient was discharged one day after surgery without complications. An ovoid-shaped pinkish mass identified at the ventral surface of the anterior tongue; B. Excisional specimen of 0.7 cm sized ovoid shape tongue mass. Thin-walled vessels lined by epithelial cells (Arrow) and separated by a thin layer of connective tissue septa (arrowheads) (100x, H&E).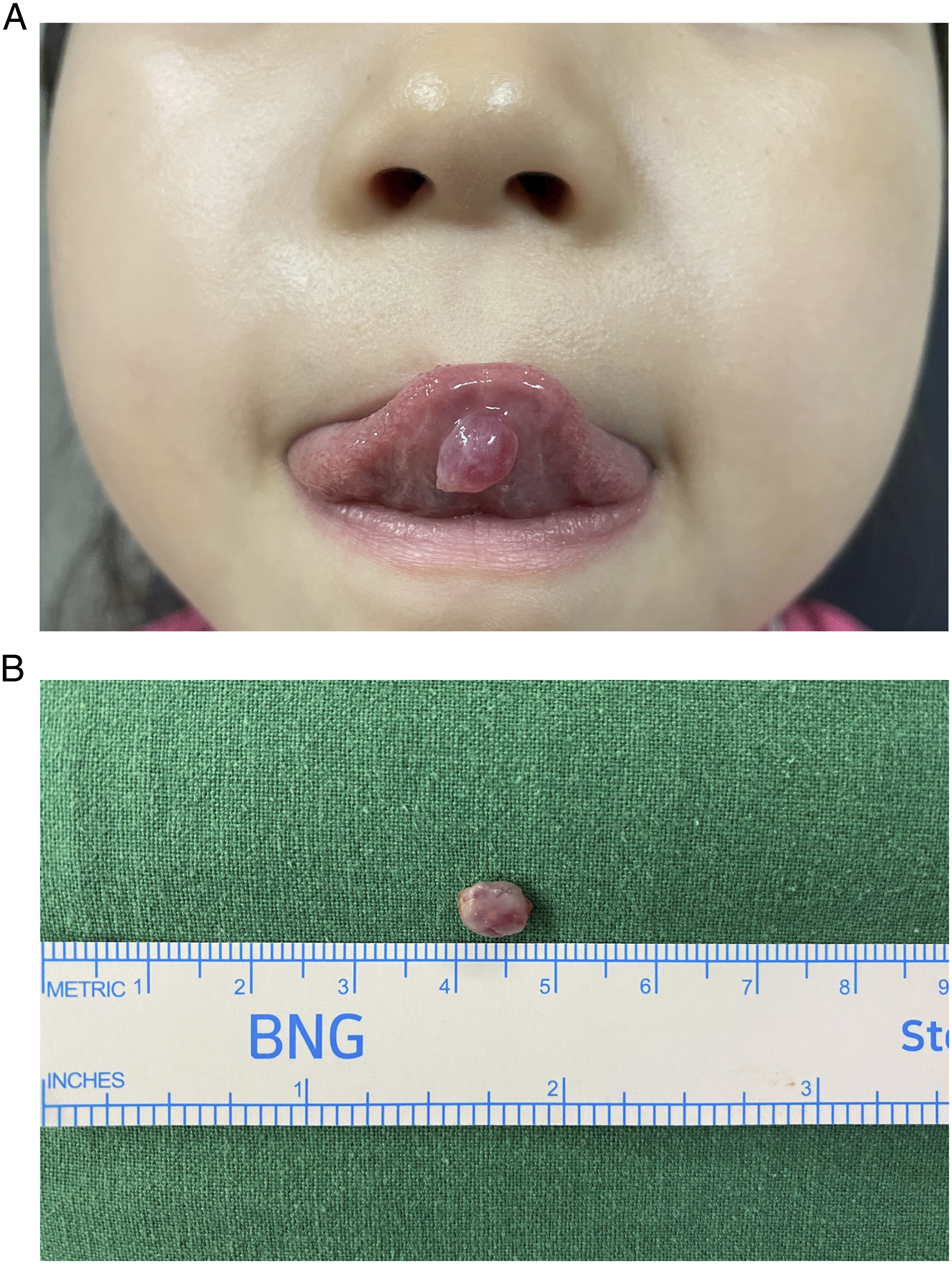
Hemangioma is caused by hormonal changes, infections, and trauma, and clinically demonstrates a hard, pulsatile, and warm mass. According to the vessel type, hemangiomas are classified into capillary, cavernous, and venous forms. 4 The clinical diagnosis is based on histopathological evaluation, and the lesion pattern may vary depending on the evolution stage. In the early stage, it is observed as a cellular lesion with a small vascular lumen and solid nest of endothelial cells. The established stage presents capillary shaped, comprising flat, well-differentiated endothelial cells of various sizes. In the involuting stage, the lumen is closed, with increased capillary wall fibrosis and hyalinization. 5 In cavernous hemangioma, sinusoids or large, thin-walled vessels composed of epithelial cells and mostly blood-filled findings are observed. 2
The treatment of hemangioma may vary depending on the patient’s age and the location and size of the lesion; it includes medical therapy (propranolol, systemic steroids), laser therapy, and surgical resection. Propranolol is used as a treatment of choice in complicated infantile hemangioma, demonstrating an effect of 96–98% during the treatment period of approximately six months. Corticosteroid therapy can be used in patients who do not respond to propranolol or where steroid use is contraindicated. However, side effects such as adrenal axis suppression and cushingoid facies should be monitored. The surgical treatment effectively treats bleeding and significantly protruding hemangioma and can be administered rapidly and permanently. 6 After cautiously considering our patient’s age and mass location, surgical treatment under general anesthesia was selected.
Horn et al. analyzed tongue lesions in pediatric patients and reported that tumors in the anterior area of the tongue had a high incidence of hamartoma, papilloma, mucocele, and hemangioma. 7 Therefore, tongue hemangioma in children requires a differential diagnosis from benign tumors.
Hamartoma refers to a tumor-like appearance resulting from normal cells undergoing tumor-like proliferation, histologically demonstrating irregularly organized smooth muscle bundles and ectopic large-caliber blood vessels. Lingual hamartoma rarely occurs, and more than 50% of it occurs with the oral-facial-digital syndrome. 8 Tongue hamartoma may look similar to cavernous hemangioma in appearance; however, histologically, hemangioma differs from large, thin-walled vessels or sinusoids lined by epithelial cells.
Papilloma is a common benign oral lesion with a cauliflower shape and a vascular core at the center. In the oral cavity and oropharynx, papilloma commonly occurs on the soft palate, uvula, tonsils, tongue, and lips. 9 It can be distinguished from hemangioma in appearance and is histologically different.
Mucocele is a mucus-filled space caused by the outflow of saliva from the accessory salivary gland duct to the surrounding connective tissue or the tube stretching due to the tube closure to form a reservoir. 10 Most mucoceles are bluish with a transparent cystic edematous appearance; therefore, they can be distinguished in appearance from hemangioma and can be differentiated by histological differences.
Significance Statement
Cavernous hemangiomas have rarely been reported in children’s tongues, and differential diagnosis is essential. The tongue is responsible for the essential element of humans, such as language activity and dietary life. Therefore, clinicians should perform accurate diagnosis and treatment through biopsy, with detailed history recording and physical examination.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.