
Abstract
The primary treatment for nasopharyngeal carcinoma (NPC) is radiotherapy. In rare cases, patients with NPC treated with radiotherapy may develop radiation-induced sarcoma (RIS), a malignant tumor, in the field of previous radiation. The prognosis is poor, and complete surgical resection is the only potentially curative treatment. We report a case of radiation-induced nasopharyngeal sarcoma after radiotherapy for NPC with suspected lung and liver metastases in a 69-year-old woman.
Introduction
Radiation-induced sarcoma (RIS) is a bone or soft tissue tumor that occurs after radiotherapy. Patients with primary cancers of the breast, cervix uteri, corpus uteri, lung, ovary, prostate, and rectum and those with lymphoma have a higher propensity for RIS. 1 However, few reports exist on RIS in the nasopharynx. Moreover, no standard treatment protocol for RIS is currently available, and RIS has a poor prognosis. Considering the rarity of RIS and its significant effect on patient survival rate, we present the case of a 69-year-old woman with nasopharyngeal RIS.
Case Report
A 69-year-old woman presented to the outpatient department with a 1-month history of diplopia. She had a history of nasopharyngeal carcinoma (NPC), for which she underwent radiotherapy 30 years ago. Her medical and surgical history revealed type 2 diabetes mellitus, hypertension, peptic ulcer, and hyperlipidemia. Physical examination revealed no obvious palpable mass over the head and neck region. Nasopharyngolaryngoscopy revealed a large necrotic mass in the nasopharynx, which obstructed over 90% of the bilateral posterior choana. No other lesions in the hypopharynx were noted, and bilateral vocal cord function was normal.
Tumor biopsy revealed spindle-shaped cells with marked nuclear atypism, bizarre nuclei, and frequent mitoses. Immunohistochemical analysis revealed that these spindled-shaped cells expressed vimentin but not AE1/AE3, EMA, p40, desmin, or myogenin (Figure 1), thus supporting the diagnosis of RIS. Microscopic finding of biopsy of the left nasopharyngeal tumor, A: AE1, AE3 negative staining, B: spindle-shaped cells with marked nuclear atypism (hematoxylin–eosin staining, 400×).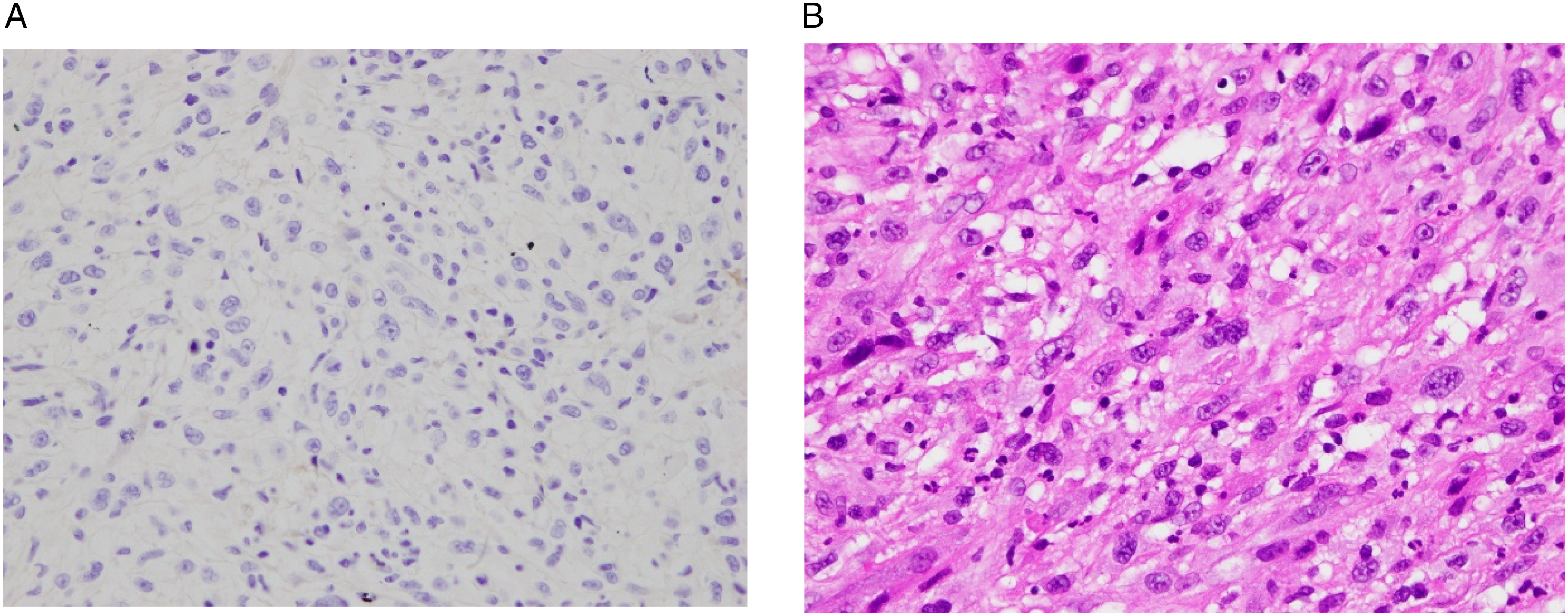
The patient was then admitted for further tumor staging examination. Contrast-enhanced magnetic resonance imaging (MRI) revealed a nasopharyngeal tumor with the largest diameter of approximately 7.4 cm, extending to the bilateral nasal cavity, left cavernous sinus, and left hypoglossal canal and infiltrated beyond the lateral surface of the lateral pterygoid muscle, with no obvious involvement of the neck lymph nodes (Figure 2). A: Nasopharyngeal magnetic resonance imaging revealed a nasopharyngeal tumor with the largest diameter of approximately 7.4 cm. B: Tumor invasion into the brain and cranial nerves. C: Tumors infiltrated the hard palate and bilateral nasal cavity.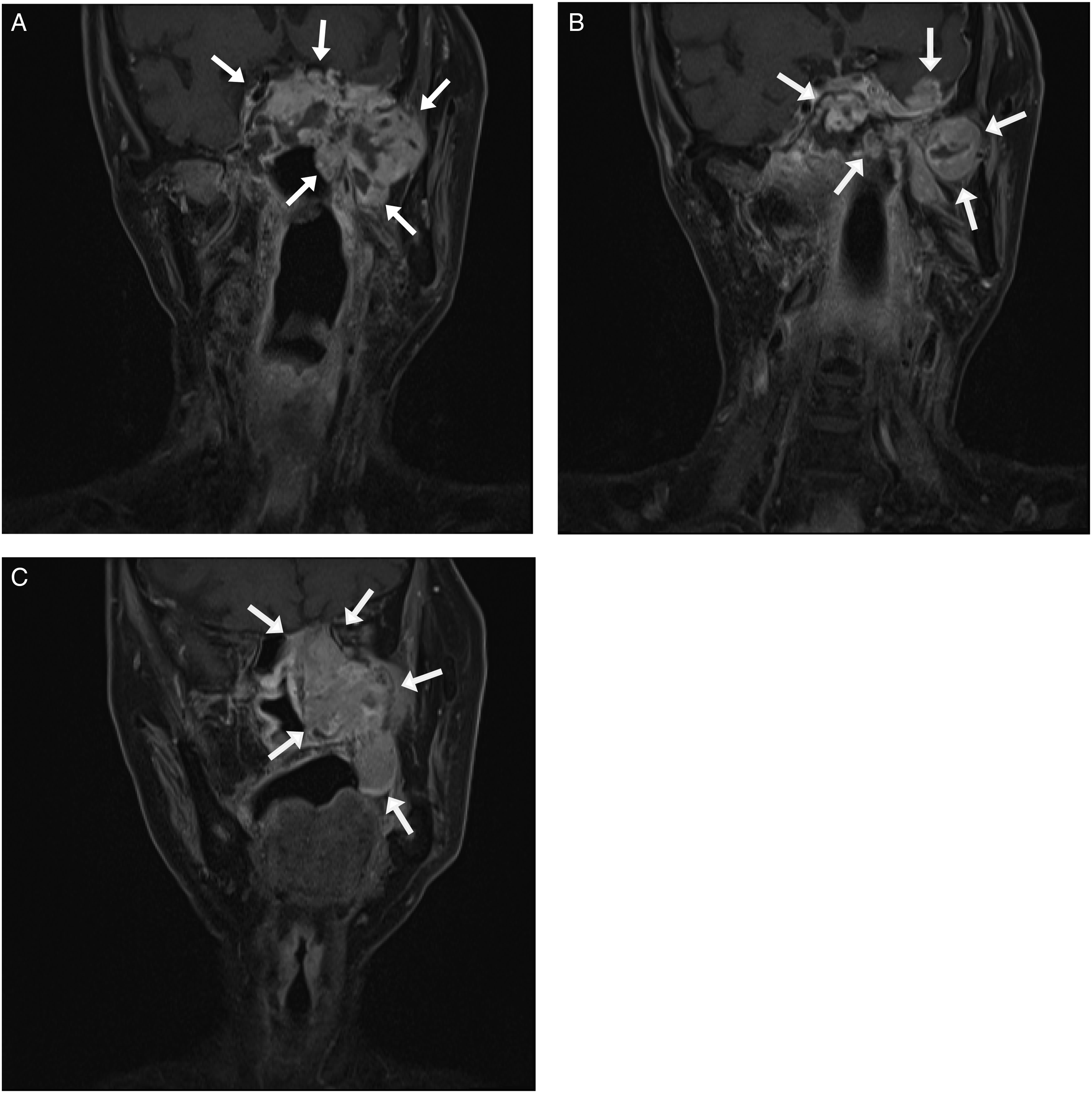
Chest X-ray indicated radiopaque patches in both lungs, and a subsequent chest computed tomography scan revealed suspicious bilateral lung and pleural metastases. Upper abdominal ultrasonography indicated a 1.5 × 1.3-cm2 hypoechoic nodule in S6 segment of the liver. Liver MRI revealed multiple hepatic nodules in S6 and S7, suggesting metastasis.
The final diagnosis was nasopharyngeal RIS with suspected lung and liver metastases. Palliative care was chosen due to the poor prognosis and the advanced stage of the disease. However, she needed to go to the ER due to fever and dyspnea just 1 week after being discharged and was admitted under the impression of pneumonia. Her condition worsened rapidly, and she died the next day.
Discussion
Radiation-induced sarcoma is a rare malignancy that occurs after radiotherapy for primary tumors. It was first reported in 1922. 2 Because of the increased survival rate of patients with cancer because of radiotherapy, the incidence of RIS has also been increasing. Radiotherapy is also a standard treatment for NPC.
The cumulative incidence of RIS is .03%–.8%. 3 In a systematic review, Coca-Pelaz et al. reported that the frequency of RIS of head and neck (RISHN) was .15%. 4 Yang et al retrospectively analyzed 27 714 patients with NPC who underwent radiotherapy from December 1998 to September 2012, and 69 (.25%) of them developed RISHNs. 5 The exact etiology of RIS remains controversial, but radiation may induce its development through DNA damage. 6 A dose–response relationship between radiotherapy and RIS incidence has been demonstrated for some malignancies.7,8 The predisposing factors of RIS include the dose and area of irradiation, age of the patient at radiation exposure, type of primary tumor, combination of chemotherapy, and genetic makeup.5,9 The latency period for establishing the diagnosis of RIS is controversial and ranges from 3 to 37 years after radiotherapy.5,10 The latency of our case between radiotherapy and RIS was within this range.
Most RISs after radiotherapy for NPC are located in the maxillary sinus or mandibular ramus, followed by the neck and gingiva; nasopharyngeal RIS is rare. The most common histologic types are fibrosarcoma and osteosarcoma.6,11 The main characteristic of RIS on MRI is soft tissue mass formation. Heterogeneous signal intensity was observed in our patient before and after intravenous administration of the contrast medium, with marked enhancement in soft tissue compared with adjacent muscles. The overall prognosis of patients with RISHN is poor. Lou et al 10 reported a 2-year overall survival (OS) rate of 50.3% and a 5-year OS rate of 14.4%. Xi et al 11 reported a 3-year OS rate of 32.4%. Chan et al 12 reported a 5-year OS rate of 24.2%. Prognostic factors include the site of RIS; histologic grade; tumor, nodes, and metastases stage; and treatment modality. 11
Radical excision is the only potentially curative treatment because RIS is extremely aggressive and strongly resistant to chemotherapy.11,13 Its radical excision is challenging because it is observed in older patients and is usually invasive. Especially when the tumor infiltrates intracranial sinuses, cranial nerves, or carotid artery, dissection of vital organs may cause major complications. Unfortunately, the nasopharyngeal RIS in our patient was not surgically accessible, and tumor infiltration into the brain, cranial nerves, and cervical vertebrae as well as lung and liver metastases were suspected. The early identification of RIS requires regular follow-up, especially in patients with long survival after radiotherapy for NPC. When encountering any suspicious lesion that progresses rapidly in the area subjected to previous radiotherapy, clinicians should, in addition to tumor recurrence, consider the possibility of RIS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.