
Abstract
Objectives
Although the guidelines clearly recommend the fasting time of children before anesthesia, it is usually difficult to control. For pediatric patients, prolonged fasting time before surgery will lead to dehydration and hypoglycemia. Adenotonsillectomy is one of the most common operations in pediatric patients, but its complications are not rare. The purpose of this study is to analyze the relationship between preoperative fasting time and postoperative complications in children undergoing adenotonsillectomy.
Methods
The medical and surgical records of 480 pediatric patients who underwent adenotonsillectomy were analyzed retrospectively. They were divided into three groups, including adenoidectomy group, tonsillectomy group, and adenotonsillectomy group. Logistic regression analysis was used to analyze the effect of preoperative fasting time on postoperative complications and hospital stay in pediatric patients of the three groups.
Results
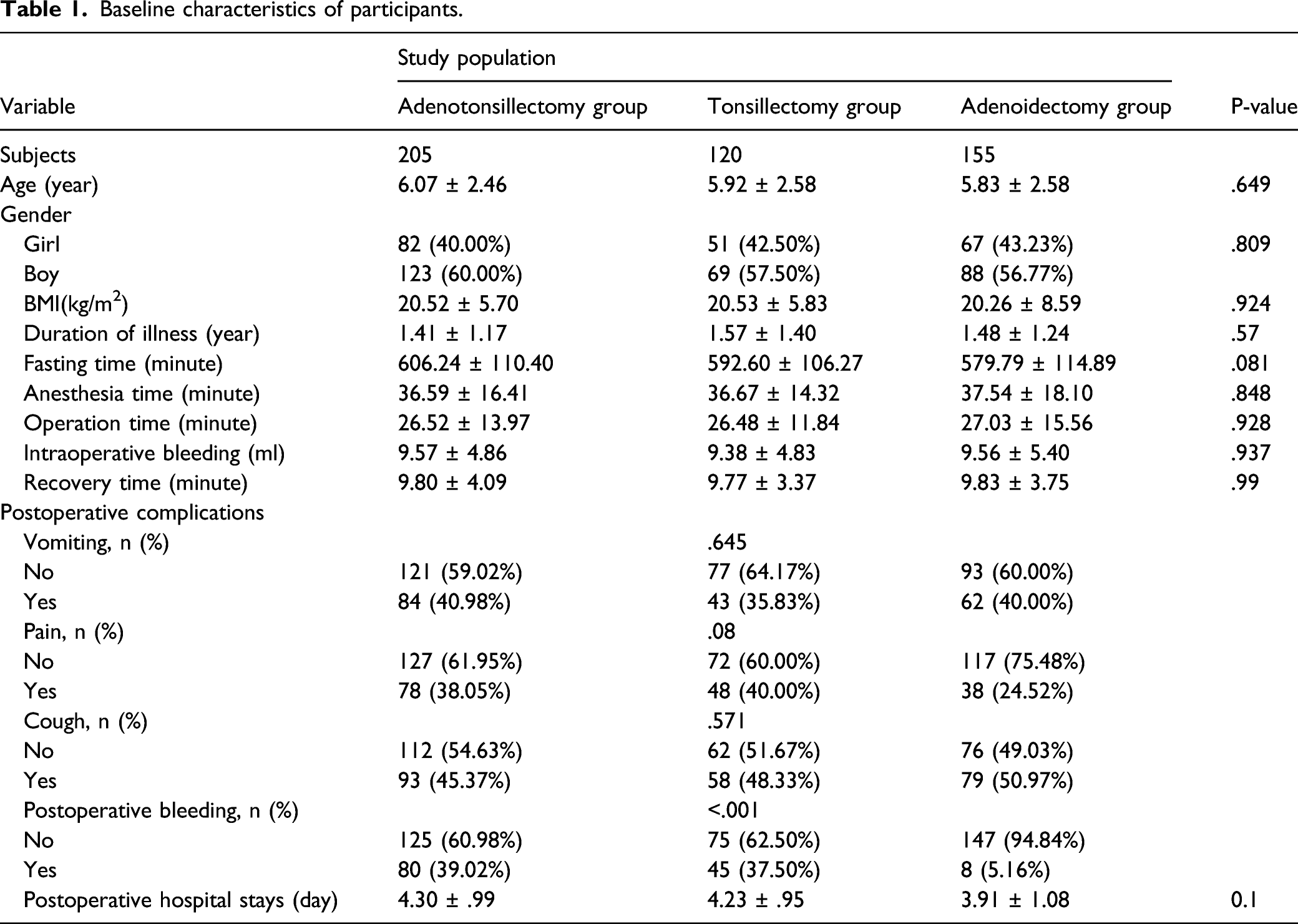
The postoperative bleeding rate in the adenoidectomy group (5.16%) was lower than tonsillectomy group and adenoidectomy group (P < .001). Logistic regression analysis showed that the fasting time was positively correlated with the vomiting and pain in adenoidectomy group, tonsillectomy group, and adenotonsillectomy group. And, the postoperative hospital stay was also positively correlated with fasting time in three groups.
Conclusion
The prolonged fasting time before otolaryngology surgery in children is related to the occurrence of postoperative complications like vomiting and pain, and also to the increase of postoperative hospital stay.
Introduction
The most common explanation for preoperative fasting is to allow sufficient time for gastric emptying, so as to prevent the contents of the stomach from being inhaled into the trachea during general anesthesia. The American Society of Anesthesiology (ASA) recommends that children fast for 2 hours of clear liquid, 4 hours of breast milk, and 6 hours of solid food or formula milk before general anesthesia. 1 Although there are clear recommendations in the guidelines, usually, most pediatric patients are required to preoperative fasting at midnight on the day of surgery. Our hospital recommends that parents give children clear liquid in the morning, but many parents will forget or give the wrong drink, resulting in prolonged preoperative waiting time. Moreover, the rearrangement and cancellation of the operation list will also make it possible for children to arrange the operation in advance, which makes it more difficult to control the preoperative fasting time.
Prolonged preoperative fasting may affect the operation and postoperative recovery process of patients. The reduction of body fluid may bring various intraoperative complications, such as increased blood loss, electrolyte imbalance, and hypoglycemia. Other clinical problems may include physical signs and symptoms such as hunger, thirst, discomfort, drowsiness, and coma. 2 For pediatric patients, prolonged fasting time before operation will soon bring the symptoms of dehydration and hypoglycemia, 3 which is a common cause of anxiety and pain for patients and their families before operation. 4 Adenotonsillectomy is one of the most common surgical operations in pediatric patients. Although it is a relatively common operation, it puts forward high requirements for surgeons and anesthesiologists. 5 The development of surgical techniques and equipment and anesthesia has reduced the risk of adenotonsillectomy, but this does not mean that there are no potential adverse events; the complications of adenotonsillectomy are not rare and sometimes serious enough to cause death. 6
The purpose of this paper is to analyze the relationship between preoperative fasting time, postoperative complications in pediatric patients undergoing adenotonsillectomy, so as to determine whether fasting time is related to the occurrence of complications in pediatric patients undergoing adenotonsillectomy, and to provide evidence for the preoperative fasting time recommended by the ASA in the perioperative environment.
Patients and methods
Subjects
This study reviewed 480 children under general anesthesia who underwent surgery of adenotonsillectomy by surgeons in our hospital from October 2018 to June 2021. Children under 14 years of age with ASA grade 1 or 2, non-emergency, no gastrointestinal absorption problems, and no obesity were included in the study. Special populations with specific fasting guidance or patients with non-standard fasting guidance given by their doctors and patients with known metabolic or endocrine disorders were excluded from the study. The start time of fasting is uniformly informed by the hospital to the parents of the children as midnight. If the time of fasting is more than 12 hours or less than two hours, the patients will be excluded. This research project was carried out following the Declaration of Helsinki by the World Medical Association and was approved by the Research Ethics Committee. All participants provided informed consent.
Data collection
We collected information from medical and surgical records, including age, gender, Body mass index (BMI), duration of illness, preoperative fasting time, anesthesia time, operation time, intraoperative bleeding, recovery time, various postoperative complications such as vomiting and cough, and the postoperative hospital stay.
Grouping
The pediatric patients were divided into three groups, including adenoidectomy group, tonsillectomy group, and adenotonsillectomy group. Fasting time was divided into two groups according to the median.
Statistical analysis
Statistical analyses were conducted using SPSS version 20.0. Values for continuous variables were represented as mean standard deviation, and those for categorical variables were described using number and percentage. Student’s t-test was used to analyze difference between two groups for continuous variable, and chi-square analysis was performed for categorical variables. Logistic regression analysis was performed to evaluate the effect of preoperative fasting time on various postoperative complications and hospital stay.
Results
Baseline characteristics of study population
Baseline characteristics of participants.
The effect of fasting time on postoperative complications in three groups
Logistic regression analysis of fasting time and vomiting in three groups.
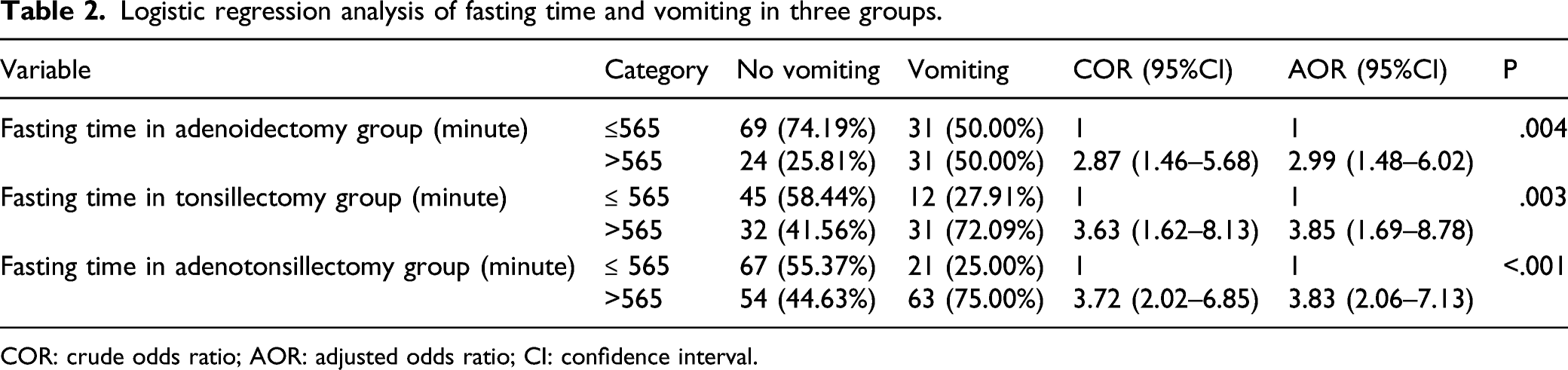
COR: crude odds ratio; AOR: adjusted odds ratio; CI: confidence interval.
Logistic regression analysis of fasting time and pain in three groups.
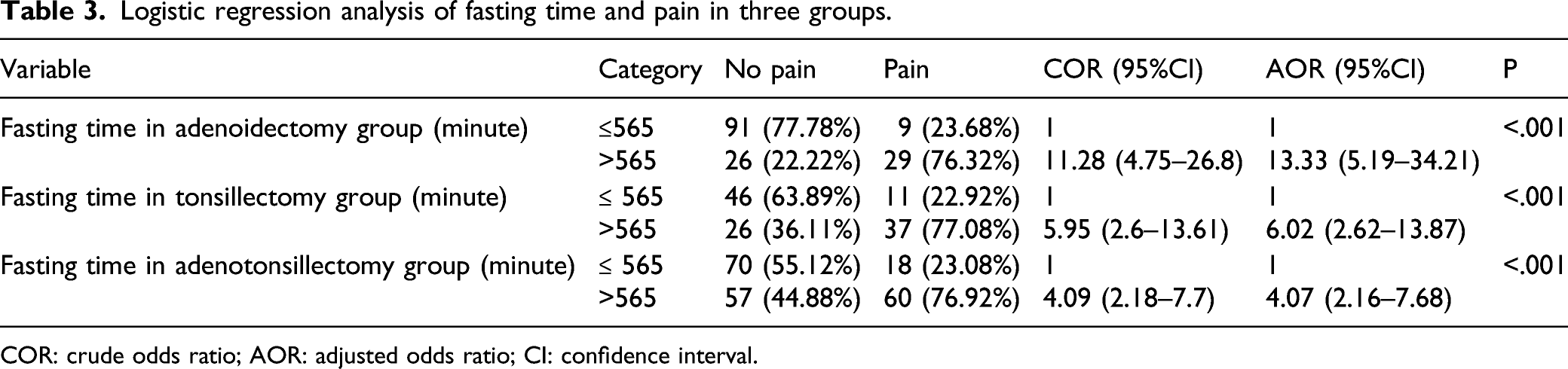
COR: crude odds ratio; AOR: adjusted odds ratio; CI: confidence interval.
Logistic regression analysis of fasting time and cough in three groups.
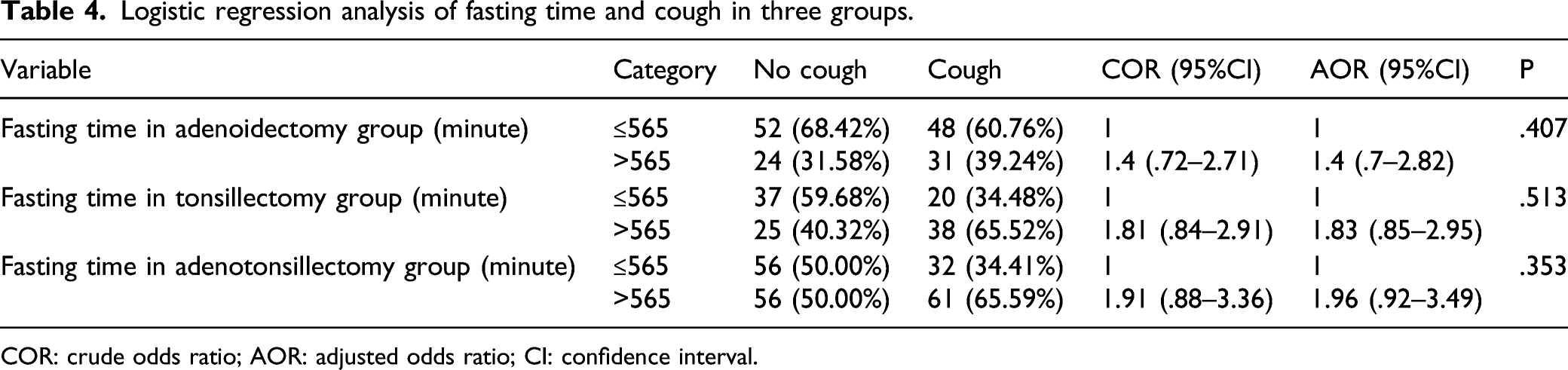
COR: crude odds ratio; AOR: adjusted odds ratio; CI: confidence interval.
Logistic regression analysis of fasting time and postoperative bleeding in three groups.
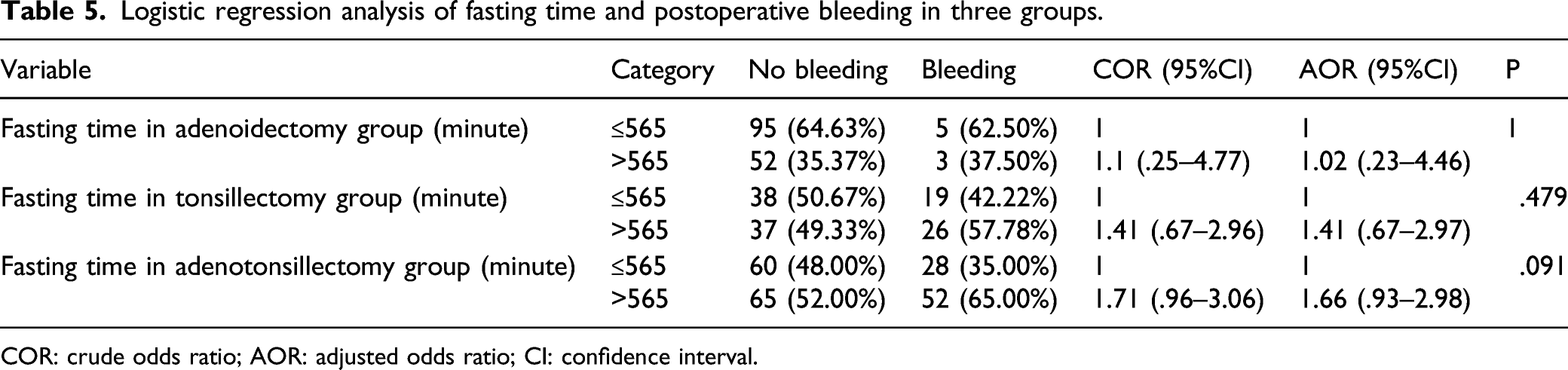
COR: crude odds ratio; AOR: adjusted odds ratio; CI: confidence interval.
The relationship between fasting time and postoperative hospital stay in three groups
Logistic regression analysis of fasting time and postoperative hospital stay in three groups.
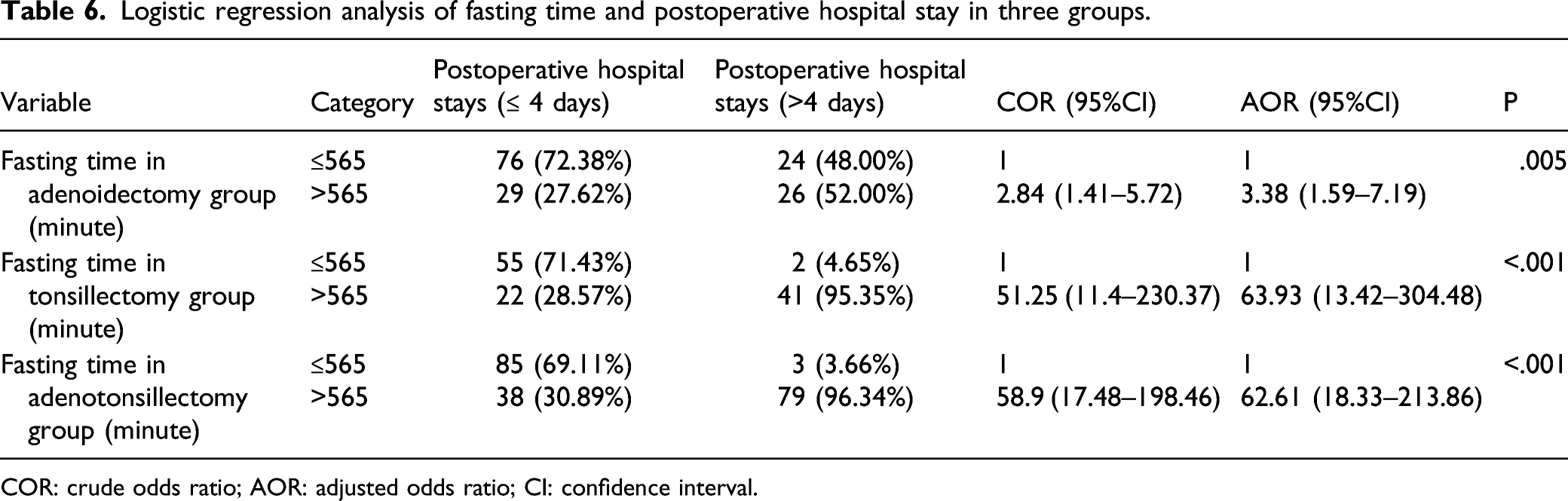
COR: crude odds ratio; AOR: adjusted odds ratio; CI: confidence interval.
Discussion
This retrospective study analyzed the relationship between fasting time and postoperative complications in children with otolaryngology. The main finding is that the longer the fasting time, the more likely the children are to have complications such as vomiting and pain, and the postoperative hospital stay will be prolonged accordingly. We found that the actual preoperative fasting time of children in our hospital was much longer than that recommended by the ASA, which may be due to the medical staff, patients and their families, or the arrangement of operating room. However, even in the United States and other developed countries, long-term preoperative fasting is still common. 7
Prolonged preoperative fasting may lead to low blood volume and metabolic imbalance, which may increase the possibility of adverse events, including arterial hypotension, venous access difficulties, and hypoglycemic events. 8 Surgical trauma, a large number of secretions in the mouth and nose, and reactive postoperative edema are the causes of postoperative complications. After adenotonsillectomy, the most common early postoperative complications in children are cough and bleeding, followed by pain, vomiting, and dehydration; infection and cardiac complications are rare. 9
Postoperative vomiting is a common complication in pediatric anesthesia. Various independent risk factors are related to the occurrence of vomiting, which often occurs in otolaryngology surgery, including tonsillectomy and adenoidectomy. 10 Our results showed that the fasting time of the three groups was positively correlated with the occurrence of vomiting. This is consistent with Urits et al, 11 who pointed out that preoperative fasting is a factor that may affect the occurrence of postoperative vomiting especially in pediatric anesthesia. We do not provide antiemetic drugs to patient conventionally, which may be different from most developed countries. In subsequent studies, we need to consider the changes after giving antiemetic drugs.
Pain after tonsillectomy is very common, inflammation and stimulation of nerve endings, pharyngeal muscle spasm, and preoperative anxiety may be one of the causes. 12 And it is well known that the preoperative anxiety increases with the increase of the preoperative fasting time. Our results also show that the fasting time in three groups is positively correlated with the occurrence of postoperative pain. Postoperative pain assessment in children is difficult to complete and depends on physiological, behavioral, and self-report methods. 13 But because this is a retrospective study, it can only judge whether children have postoperative pain through medical records, which is one of the limitations of this study. We will standardize the pain score in the follow-up study.
Endotracheal tube may cause cough during anesthesia recovery after otolaryngology surgery in children, which usually lasts for several hours to several days. 14 However, no study has reported whether the fasting time will lead to the occurrence of postoperative cough. A large sample statistical article from Korea 15 reported that adenotonsillectomy did not change the risk of upper respiratory tract infection in children. Our results show that although the incidence of postoperative cough is about 50%, the fasting time has no effect on its occurrence.
In terms of bleeding reporting, some people will define any small or large bleeding after tonsillectomy as bleeding, while others will only strictly define bleeding as large bleeding that needs to be returned to the operating room for control. 16 In the medical records retrospectively analyzed in this study, whether a small amount or a large amount of bleeding is defined as postoperative bleeding, this may result in a high postoperative bleeding rate. Our results showed that although the probability of postoperative bleeding in adenotonsillectomy group and tonsillectomy group was higher than that in adenoidectomy group, the fasting time of the three groups was not related to postoperative bleeding. The results of Spektor et al 17 pointed out that age and history of recurrent tonsillitis were related to the occurrence of bleeding after tonsillectomy in children, but there was no study on the relationship between preoperative fasting time and postoperative bleeding. Further research studies are needed to find out the specific causes.
Postoperative complications will lead to prolonged postoperative hospital stay and increased medical expenses. 18 Our statistical results showed that there was a positive correlation between preoperative fasting time and postoperative hospital stay in three groups, which was corresponding to the results of complications.
Shortening the fasting time before operation can improve the metabolism and hemodynamics during anesthesia. 19 It can also relieve patients' preoperative anxiety, especially in children. 20 In order to protect pediatric patients from long preoperative fasting time, freer fasting programs and better interdisciplinary cooperation need to be considered. 21
Conclusion
Preoperative fasting time is related to the occurrence of postoperative complications, such as vomiting and pain. In addition, the preoperative fasting time also leads to the extension of postoperative hospital stay. Although the standards of our hospitals are different from those in most developed countries, they are indeed common in developing countries. Our results may lead more people to consider improving preoperative fasting strategies in order to prevent postoperative complications in children’s otolaryngology better. Medical staff should communicate more with children’s parents to formulate a more optimized fasting program that meets the standards.
Footnotes
Acknowledgment
This research was supported by the Yanbian University Hospital.
Author contributions
Writing—original draft preparation: Yonghao Huang and Junhu Tai
Review and editing: Yongshan Nan
Supervision: Yongshan Nan
All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The data collection was approved by the medical ethics committees of the Yanbian University Hospital
Informed consent
Written informed consent was obtained for each participant.