
Abstract
Introduction
Stapes surgery is one of the most technically demanding procedures in otology. Rediscovery of key areas of the complex anatomy of the middle ear and intratemporal facial nerve through oto-endoscopy has revolutionized the surgical approach. Thus, endoscopic stapedotomy (ES) has become a practical and cost-effective alternative to microscopic stapedotomy (MS). 1 It provides better visibility, proximity to the surgical field, adequate magnification without loss of illumination, less bone work/tissue trauma, and angled vision, promising a better success rate with fewer morbidities. However, for the otolaryngology residents in most parts of the world, there is yet to be a structured, curriculum-based, formal training exclusive to ES. Furthermore, for today’s otologists, the transition to ES is almost always from the conventional microscope with which one had begun surgical training. Thus, the learning curves for these two techniques are not synchronous. With the gradual decrease in the incidence of stapes surgery, the experience of a surgeon as determined by her/his position on the learning curve becomes vital in deciding a preferable technique in a given situation.1,2 Keeping this in mind, the present study attempts to analyze outcomes of the two techniques with predetermined evaluation parameters, from the perspectives of a group of otologists who are in different positions in their learning curves for the respective surgical approach concerned.
Materials and methods
Selection criteria for the subjects considered during their inclusion in the study.
For bilateral otosclerosis, the laterality of surgery was determined by the relatively worse ear [larger air-bone gap (ABG); Weber lateralization] and by the patient’s choice if the pure tone average (PTAv) in both ears was comparable. In occasional situations when the patients were undecided about their choices, the right ear was selected (all operating surgeons were right-handed). The 34 ears to be operated on were initially placed alternately in the microscopic and endoscopic groups; however, this alternate selection could not be maintained due to exclusion at surgery due to conditions other than otosclerosis and attrition at follow-up.
The surgeries were performed by the same group of surgeons, that is, the first 3 authors. At the time of the inception of the present study, all had more than 12 years’ experience in MS, and had been consistently performing ES for 3 years. They had learned transcanal endoscopic ear surgery (TEES) once the facility was introduced to the institute 5 years ago. Therefore, they were considered to belong to the “traditional school” when this study was started. The 3 surgeons in the group performed ES and MS as and when required on a case-by-case basis, and followed identical principles and techniques of surgery in respective procedures.
Each patient signed an informed consent that included information on known complications and drawbacks of surgery in the near- and long-term follow-up, their choice of surgery over hearing aid as a nonsurgical treatment, and, when appropriate, the laterality chosen. The study received approval from the Institutional Ethics Committee.
Regardless of whether a microscope or endoscope was used, optimal surgical field exposure (“adequate surgical exposure”; ASE) with the minimum possible tissue trauma was achieved. The ASE consisted of the oval window niche (OWN) along with the second genu of the fallopian canal, the pyramidal process with the stapedius tendon, and the round window niche; the ASE ensured proper placement of the piston. The OWN itself consisted of the footplate and suprastructure of the stapes, the incudostapedial joint, and the distal part of the stapedius tendon. In some ears, the OWN was partly or completely obscured by a bony overhang that needed drilling/curettage to attain the ASE. Again, in some ears, the OWN was visible, but with a bony overhang obscuring the ASE. Following our principle of performing surgery with minimal tissue trauma, in some ears, such bony overhang could be negotiated by adjusting the patient’s head relative to the surgeon using the microscope or by maneuvering the endoscope, using an angled one when required. However, in the rest, this bony overhang had to be drilled/curetted to attain the ASE. The concept is represented diagrammatically in Figure 1. Diagrammatic representation of the concept of approach to adequate surgical exposure (ASE) (hand-sketches provided by the first author). The oval window niche (OWN) may remain completely or partially obscured by bony overhang (yellow shade) (A). In such instances, drilling/curettage is attempted until the ASE (C) is achieved. Occasionally, the OWN is visible but still there is a bony overhang (B). This overhang may be negotiated by adjusting the patient’s head with respect to the surgeon (while using a microscope) or by maneuvering the endoscope, using an angled one when needed. If it is impossible for the overhang to be negotiated, further drilling/curettage is attempted for attaining the ASE. Abbreviation: OWN, stapes suprastructure and footplate, incudostapedial joint, distal part of the stapedius tendon; ASE, OWN + second genu of the fallopian canal, round window niche, pyramidal process and stapedius tendon; I, incus; ST, stapedius tendon; P, pyramidal process; F, fallopian canal; RWN, round window niche; CT, chorda tympani; TM flap, tympanomeatal flap]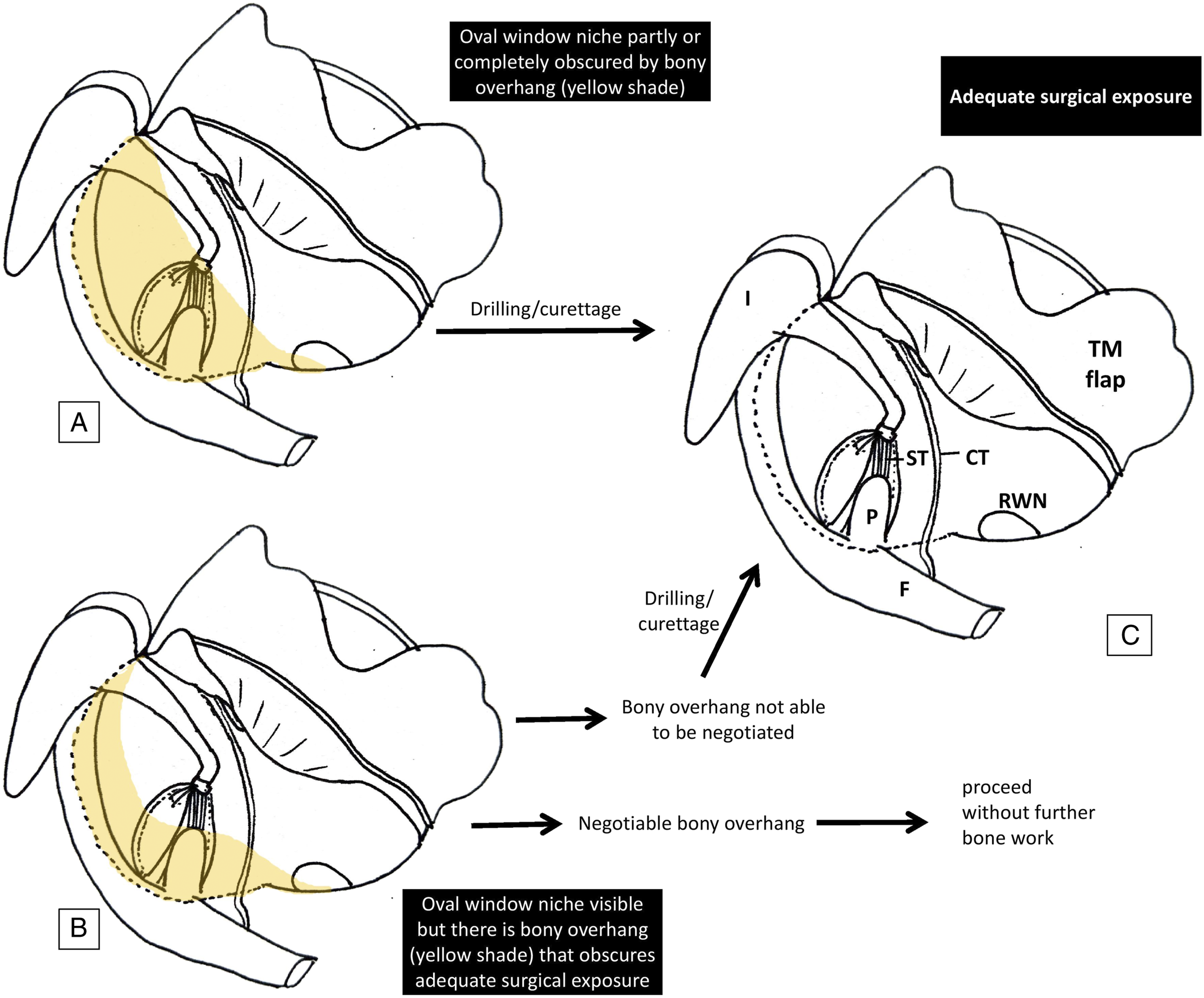
The surgical steps at the OWN were similar in all ears. This involved dislocation of the incudostapedial joint, sectioning of the stapedius tendon, fracturing the crurae, and subsequent removal of the suprastructure. The fixed footplate was perforated in the posterior third with a conventional hand-held perforator (.7 mm diameter), and a Teflon piston (Shea variety; .6 mm diameter) was inserted. Standard 0° and 30° oto-endoscopes, 3 mm in diameter, 14 cm long (Karl Storz SE and Co. KG, Tuttlingen, Germany) and an operating microscope (Carl Zeiss Meditec AG, Goeschwitzer Strasse 51-52; 07745 Jena, Germany; Model: OPMI 1FC) were used in the respective groups.
Statistical analysis
The results were tabulated in Microsoft Excel spreadsheets (Microsoft Corporation; Redmond, Washington, USA), and analyzed in terms of the given epidemiological, preoperative, perioperative, and postoperative parameters, with a minimum follow-up of 12 weeks. Closure of ABG within 10 dB was considered “successful” outcome of surgery. Calculations were made with IBM SPSS (International Business Machines Corporation; Statistical Package for Social Sciences) Statistics software version 22 (Armonk, New York, USA) with appropriate statistical parameters. The level of statistical significance was established at P < .05.
Level of evidence
2b (according to the Oxford Centre of Evidence-Based Medicine) 3
Ethical standards
All procedures contributing to this work comply with the ethical standards of the relevant national and institutional guidelines on human experimentation, as laid down in the Helsinki Declaration of 1975, as revised in 2008.
Results
Of the 17 ears alternately included in each of the MS and ES groups, the pathology in 3 and 2 ears, respectively, was evident at surgery to be conditions other than otosclerosis. A patient in each group was lost to follow-up. In addition, surgery in one ear in the microscopic group was abandoned due to cerebrospinal fluid gusher. There was no incidence of floating footplate or other perioperative complications. Therefore, the attrition in the groups consisted of 5 and 3 ears/patients, respectively, and the study was completed with 26 ears/patients, 12 in the microscopic group, and 14 in the endoscopic group.
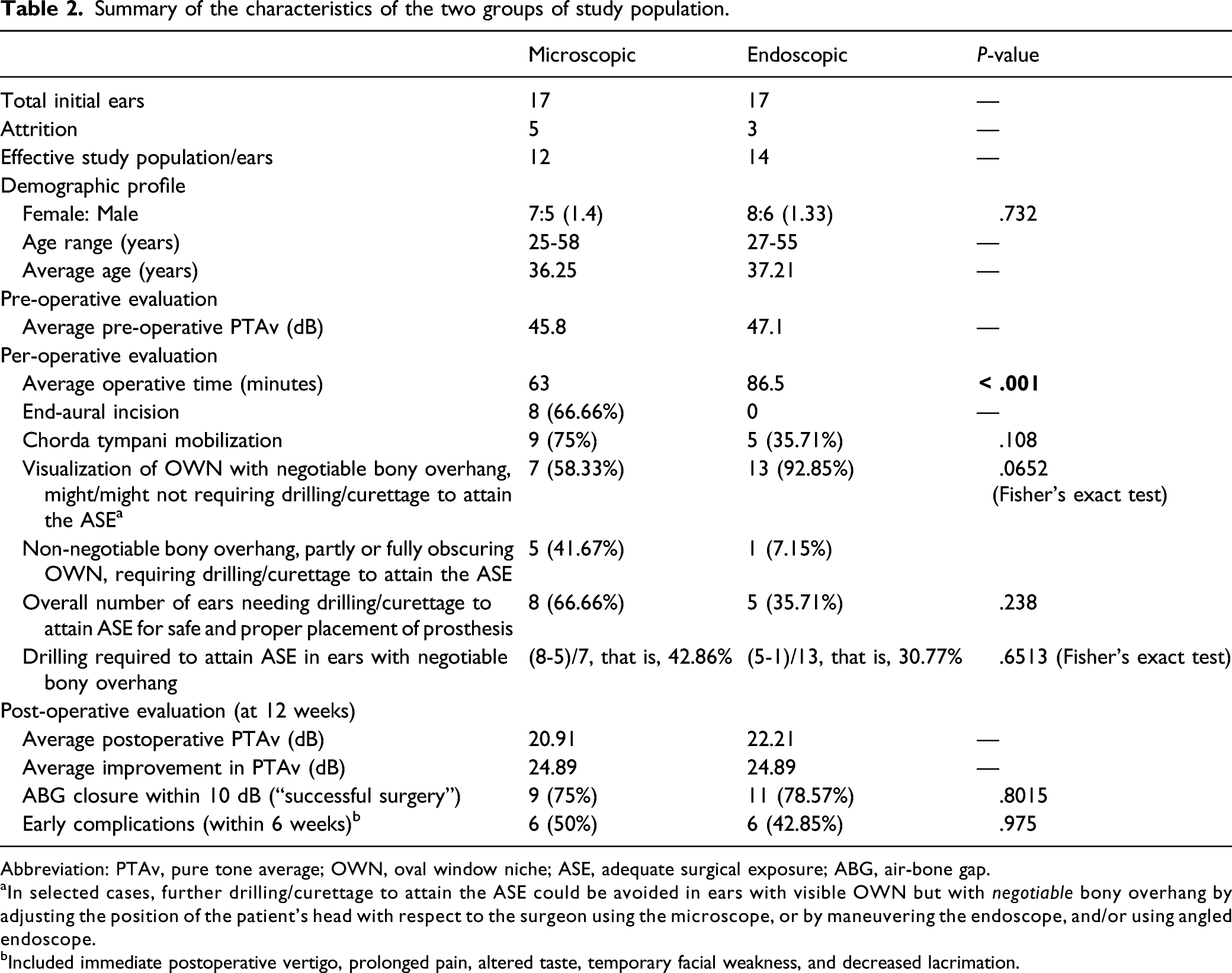
Summary of the characteristics of the two groups of study population.
Abbreviation: PTAv, pure tone average; OWN, oval window niche; ASE, adequate surgical exposure; ABG, air-bone gap.
aIn selected cases, further drilling/curettage to attain the ASE could be avoided in ears with visible OWN but with negotiable bony overhang by adjusting the position of the patient’s head with respect to the surgeon using the microscope, or by maneuvering the endoscope, and/or using angled endoscope.
bIncluded immediate postoperative vertigo, prolonged pain, altered taste, temporary facial weakness, and decreased lacrimation.
The average age in the microscopic group was 36.25 years and in the endoscopic group 37.21 years. There was marginal female predominance in both groups that was not statistically significant. The average preoperative PTAv was 45.8 dB and 47.1 dB, respectively.
Almost 67% of ears undergoing MS required an end-aural incision to widen the external auditory canal (EAC); however, the average operative time was significantly shorter compared to ES (63 minutes and 86.5 minutes, respectively; P < .001). To achieve ASE for safe and proper piston placement, drilling/curettage was required in ∼67% of microscopic and ∼36% of endoscopic groups (P = .238) and mobilization of the chorda tympani in 75% and ∼36% ears, respectively, (P = .108). In ∼42% and ∼7% of the respective groups, the bony overhang partially or completely obscured the OWN, necessitating drilling/curettage to achieve the ASE. In the rest, that is, in ∼58% and ∼93% of the respective groups, the OWN could be visualized, but with a bony overhang that appeared negotiable. The differences were noticeable, but not statistically significant (P = .0652; Fisher’s exact test). Among ears with apparently negotiable bony overhang, ∼43% of the microscopic group and ∼31% of the endoscopic group actually required further curettage/drilling to achieve ASE (P = .6513; Fisher’s exact test).
At 12 weeks of follow-up, the average PTAv improved by 24.89 dB in either group. ABG closure within 10 dB (defining “success”) was recorded in 9 and 11 ears in the microscopic and endoscopic groups, respectively, although this difference was not statistically significant (P = .8015). Some complications were encountered in the early postoperative period (within 6 weeks); however, the difference in the number of patients who had such complications was not significant (P = .975).
Discussion
The present study showed that although the precise surgical work in the OWN remained the same in both the MS and ES groups, they differed in operative time and in approaches to achieve ASE. We sought to see how they differed in these aspects and in their postoperative outcomes from a group of otologists in differential positions in their learning curves with respect to these two procedures. Carefully selected ears in patients with statistically insignificant differences in demographic profile provided credibility to our results. The average ages of the subjects in microscopic and endoscopic groups (just over 36 and 37 years, respectively) corroborated with the observation that hearing impairment in otosclerosis does not become clinically evident before the fourth and fifth decades of life. 4 In general, the values of all the parameters considered in this study were statistically insignificant, except the operative time.
The operative time for ES was longer. Engagement of the non-dominant hand and single-handed procedures (raising tympanomeatal flap, curettage/drilling, simultaneous suction, and placing adrenaline-soaked cottonoids) were the preliminary hurdles. Anatomical factors like relatively narrow EAC in non-Caucasian subjects caused difficulty in negotiating the oto-endoscope and the operating instrument simultaneously. Also, regardless of laterality, anchoring the piston to the perforated stapes footplate, gripping the long process of incus with a pick, and crimping the loop of the piston required 3 different moves that might initially be challenging for the endoscopic surgeon. The lack of three-dimensional stereoscopic view and depth perception, unlike microscope-aided vision, further complicated the learning with endoscopes.1,5
The present study revealed that other than the operative time, ES appeared to have advantages over MS in visualization and postoperative results (Table 2). However, those advantages were only numerical and not statistically significant. Understandably, the ease of locating anatomical landmarks with adjustable proximity can be achieved through minimal surgical trauma, and this far exceeds the inconveniences of one-handed protracted surgery. This is evident in the lesser proportion of subjects in the endoscopic group that required the mobilization of the chorda tympani (∼36%, vs 75% with a microscope) and drilling/curettage (∼36%, vs ∼67% with a microscope) to properly visualize OWN and achieve ASE. Existing literature supports this trend. Sproat et al. 6 documented the need for chorda tympani mobilization in 7% of ES compared to 23% in MS. 6 Likewise, with the endoscope, removal of the scutum and mobilization of the chorda tympani were reported to be less frequent by Kojima et al. 5 and Surmelioglu et al., 7 while Hunter et al. 8 experienced the need for curettage in ∼72% of their study population. The OWN could be satisfactorily visualized by an endoscope in more than 80% of the subjects in a study by Naik et al., who required atticotomy and mobilization of the chorda tympani in only 30% and 25% of the patients, respectively. 9
As an important observation, drilling/curettage was actually required for ASE in only ∼31% of ears undergoing ES and ∼43% in MS in subjects who had proper visualization of the OWN but with negotiable bony overhang. That is, in ∼69% of ears undergoing ES, exposure of the OWN was sufficient to bring about ASE by maneuvering the endoscope, using an angled one when needed. Similarly, in ∼57% of MS, further drilling/curettage could be avoided by adjusting the patient’s head relative to the surgeon. This further signifies that proper visualization of OWN even without significant bony overhang did not always provide the ASE—an experience also shared by Nogueira et al. 1 with ES. 1 Thus, the approach to ASE could differ in the two groups with respect to the extent of bone work involved. In this context, it should be reiterated that ASE is meant for safe and confident placement of piston, and the need for additional surgical work beyond the OWN to achieve this had not been compromised irrespective of ES or MS in this study. Indeed, the endoscope was better at avoiding this facultative step, but since the difference was not statistically significant, this article does not suggest that ES should be performed without bone removal if such a need actually arises.
In a different perspective, the results of the perioperative and outcome parameters indicate that MS could also be equally rewarding. Although the approach to stapes suprastructure and footplate required end-aural incision in ∼67% subjects in this group, its primary reason apparently was geoanthropometric. The EAC of the eastern Asian population is narrower, 10 although updated statistical data on comparative interracial dimensions are lacking. The Western literature describes MS with the need for end-aural incision in a relatively lower proportion of subjects (for example, ∼34% in the study by Sproat et al. 6 ), or even without it. 11 The remaining parameters of our study, including outcome factors such as hearing improvement, showed statistically insignificant differences. The number of patients with ABG closure within 10 dB (“successful” surgery) was closely comparable between the groups.
The present study has certain limitations. The sample size in both groups could have been increased had the study period been extended further; this could add to the credibility of our results. This is especially relevant for the apparently modest success rate of surgeries and the relatively more early complications. Similarly, a prolonged follow-up could better evaluate hearing outcome and complications. However, the present sample strength along with the strict evaluation protocol and follow-up schedule provided an initial trend, especially when the surgeons’ positions in the learning curve for the two procedures had to be an important deciding factor.2,12
The surgeons who participated in this study had different levels of experience in stapedotomy with microscope and endoscope. With more than 12 years of experience in MS, the surgeons have started the procedure with endoscope on a regular basis for 3 years. Accordingly, they were in different positions of their learning curves with MS and ES. Furthermore, since ES is generally considered the final step in acquiring expertise in the spectrum of TEES, the surgeons could have given themselves more time with the other TEES procedures before starting with ES. These can aptly explain the statistically significant difference in operating time. However, the differential experience level of the surgeons was a deliberate and intrinsic consideration in this study design because our objective was to analyze stapedotomy through the microscope and endoscope from the perspectives of surgeons of the “traditional school.” On a different note, this further explains the small sample size and shorter follow-up schedule, lest the surgeons shift to a comparably favorable position in their learning curves for ES. Also, it has been conventionally assumed here that since the surgeons belonged to the same school of training with equivalent experience, their level of expertise in each procedure would be comparable and would not significantly affect the results when compared.
We might consider the inclusion criteria of a minimum preoperative ABG of 25 dB a true limitation for this study. This could potentially lead to selection bias, but it was an unavoidable factor to consider. However, instead of “change in ABG” after surgery, we tried to negate any potential selection bias by assuming “closure of ABG within 10 dB” as one of the outcome parameters defining success, so that it remains independent of the preoperative value of ABG. Again, had the point of selection been at surgery instead of prior to it, the exclusion of conductive hearing impairment with intact tympanic membrane for reasons other than otosclerosis could have been avoided. However, we believe that the present selection would least influence the final outcome as the exclusions were carried out meticulously.
The present study captures the perspectives of the contemporary generation of otologists in a transition zone between traditional microscopic procedures and the ever-increasing potentialities of TEES and endoscopic skull-base surgery.12,13 It deals with the experience of a representative group of surgeons in their transitional phase, who are experts in microscopic procedures and have been performing otologic surgeries with the endoscope relatively recently. We consider this background and timeliness as a major strength of our study.
Conclusion
There was no statistically significant difference between MS and ES in the standard surgical steps and in the postoperative outcomes, except the time consumed. The operative time for ES may be significantly longer, which could be attributed to the differential learning curves of the participating surgeons with the two techniques. Numerically, MS and ES differed at the ease at surgical maneuverability and visual adequacy, where the endoscope was better. However, there appeared to be little difference between the two for the “traditional school” otologists, other than when they wish to ascend the learning curve with a newer technique (here, endoscopic).
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Authors’ note
Please note that this study is not multi-institutional. The study was conducted at Medical College and Hospital, Kolkata, India, in the departments of Otorhinolaryngology and Head-Neck Surgery (where the first 3 authors, i.e., SK, MD, and BG, worked at the time of the study; MD still works there) and Community Medicine (where the last author, PG, was affiliated). The authors hold government jobs which are transferable. The above affiliations are the most updated ones at the time of submission of this paper.