
Abstract

Syphilis, also known as “the great imitator,” is a sexually transmitted infectious disease that can clinically present with non-healing or recurrent oral mucosal ulcers which may be mistaken for extraintestinal manifestations of Crohn’s disease or other autoimmune disorders. Here, we report a case of a 25-year-old female who presented to clinic for biopsy of non-healing recurrent ulcers as a part of herwork up for autoimmune disease. Biopsy revealed secondary Treponema pallidum infection.
A 25-year-old female with a six-month-long history of recurrent ulcers on the upper and lower lips, nasal mucosa bilaterally, and posterior oropharynx was referred to our clinic after failed resolution despite treatment with nystatin, valacyclovir, and triamcinolone paste. She had unintended weight loss secondary to odynophagia for 5 months prior to her clinic visit. Past medical history was significant for aphthous stomatitis, Crohn’s disease, tobacco abuse, migraines, menorrhagia, anxiety, and depression. She was of childbearing age and endorsed sexual activity. Specific sexual practices (i.e., oral sex) were unknown. Of note, there was documentation of a remote history of a spontaneously resolved genital lesion of unclear etiology. At the time of referral, she was undergoing treatment with adalimumab for Crohn’s disease. Given her lack of response to treatments for suspected Candida and herpes infections along with her 13-pound weight loss, the leading suspicion was Crohn’s exacerbation with oral involvement vs vasculitis. On physical exam, she was found to have a 1-cm ulceration on the right lower lip mucosa (Figure 1) with additional lesions scattered throughout the oral cavity including the left retromolar trigone. Though previously noted by a referring provider, no lesions were found in the nasal mucosa at the time of the biopsy. Punch biopsies were obtained from the right lower lip and left posterior buccal mucosa. Histology findings were inconsistent with Crohn’s disease which typically has limited inflammation and scattered epithelioid granulomas. Instead, microscopic analysis of biopsy tissues revealed thickened mucosa with hyperkeratosis, indicative of a reactive squamous epithelium, abundant intraepithelial neutrophils suggestive of acute inflammation, and a very dense submucosal chronic inflammatory infiltrate with numerous plasma cells. These histologic features, particularly the plasma-rich dense chronic inflammation, led to additional immunostaining which showed numerous thread-like organisms diagnostic of Treponema palladium infection (Figure 2). The patient and referring provider were promptly informed, and the patient elected to seek treatment at their local health department.
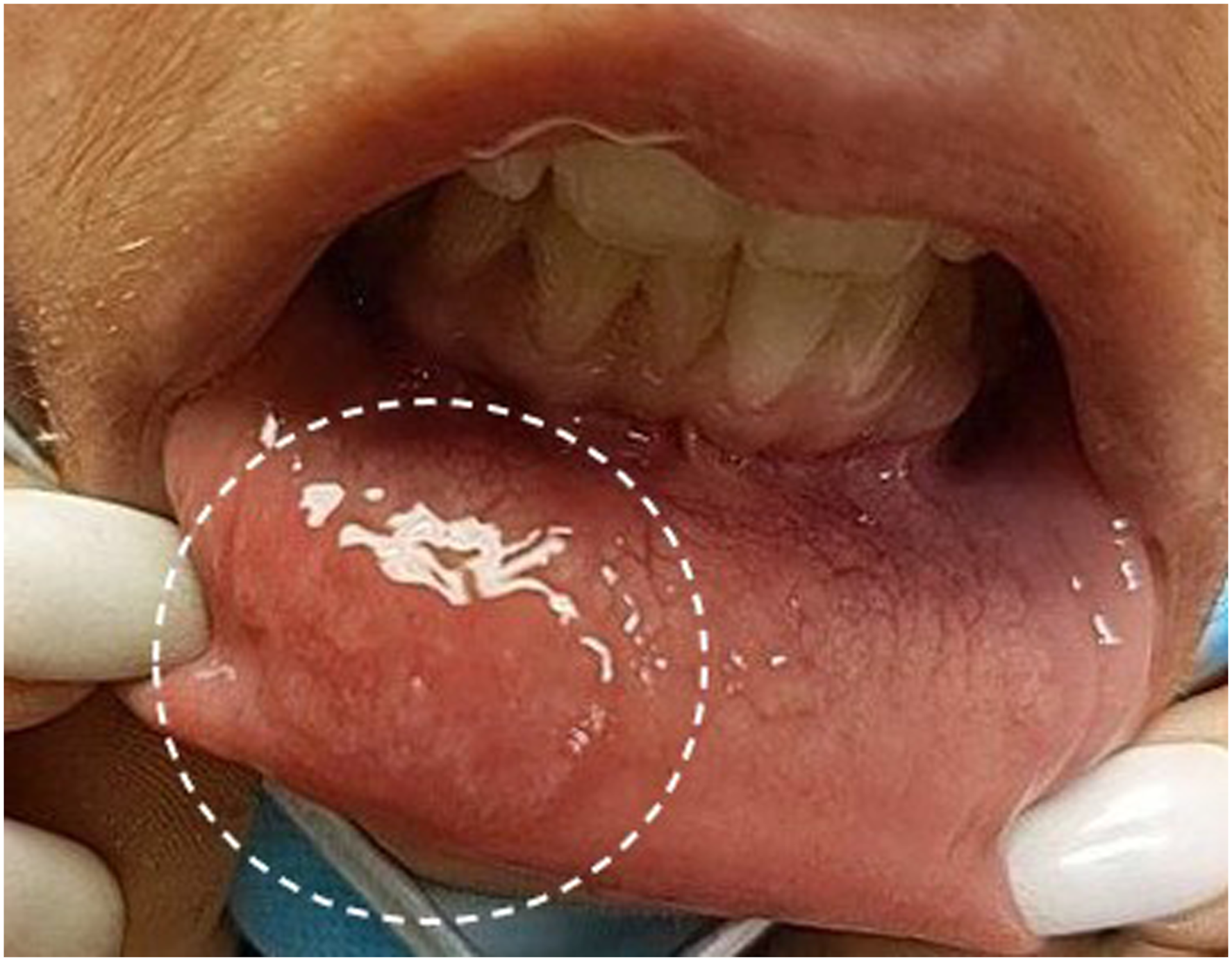
1-cm ulceration on the mucosal surface of lower lip.
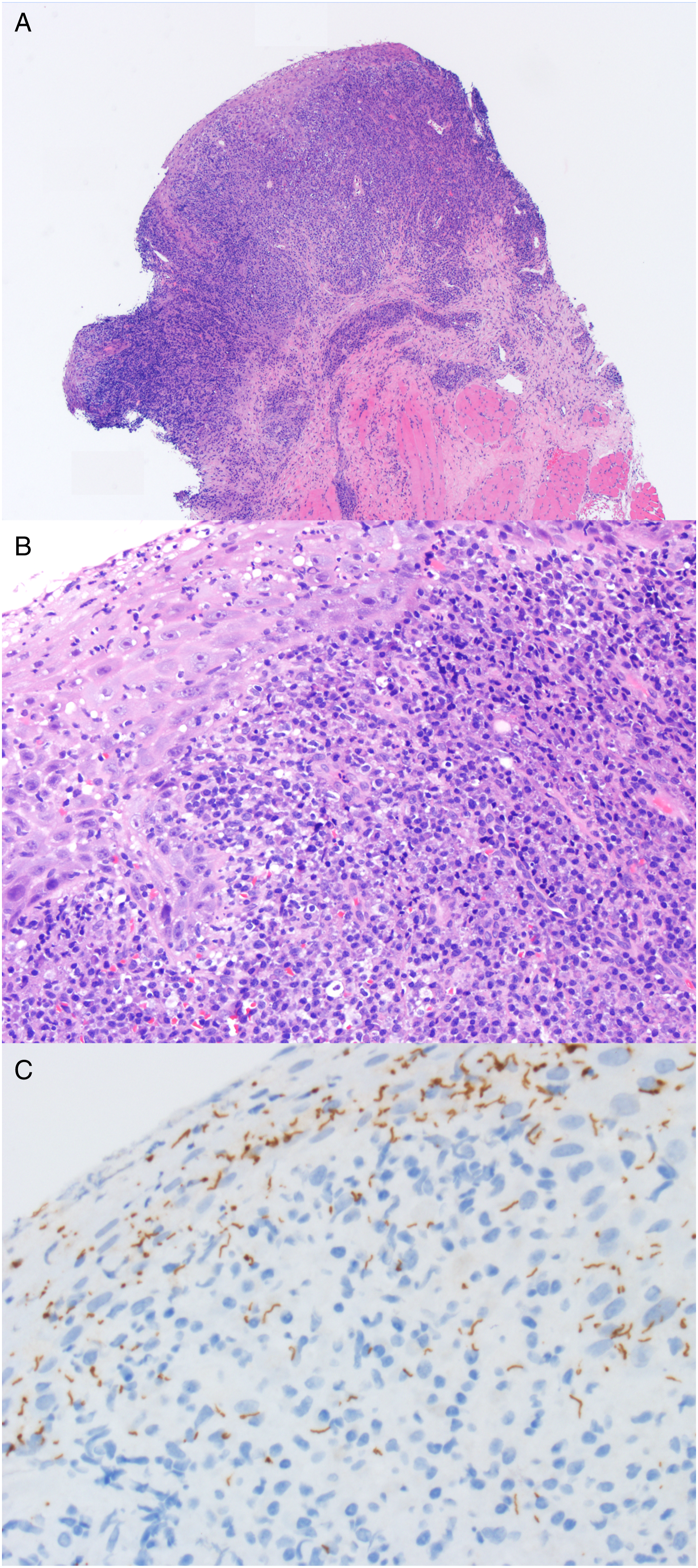
Surgical pathology from the patient’s oral cavity and lip biopsies. (A) The buccal mucosa shows a very dense lymphoplasmacytic submucosal infiltrate (H&E ×4 magnification). (B) On higher power, the squamous epithelium is thickened and reactive with acute inflammation and associated with the dense, plasma cell-rich submucosal infiltrate (H&E ×20 magnification). (C) Treponema pallidum immunostaining shows abundant thread-like and irregular brown staining organisms throughout the epithelium (×40 magnification).
Syphilis is a sexual or congenitally acquired infectious disease caused by the spirochete T pallidum. The classic presentation involves a painless chancre that emerges on the tissue surface of transmission and self-resolves over 3-6 weeks. Most often, the lesion is found on genital surfaces; however, it can also be found on the oral mucosa if contact occurs during oral sex. The incidence of oral syphilis has been increasing in recent years and therefore should be considered in the differential diagnosis of oral ulcers.1,2 If not adequately treated, the disease can progress to a secondary stage characterized by the development of skin rashes and/or painful sores along mucous membranes. On occasion, patients will present with non-healing and/or recurrent oral ulcers that mimic those seen in rheumatologic diseases such as Crohn’s.
Common etiologies of oral ulcers include gastrointestinal diseases (i.e. Crohn’s and ulcerative colitis), other autoimmune disorders, trauma, and contact hypersensitivities.3,4 Aphthous stomatitis, periodontitis, and orofacial granulomatosis are all described as oral pathologies associated with Crohn’s disease and affect 5% to 50% of adult patients.5-7 While aphthous stomatitis can also present as a sign of Behcet syndrome, a chronic vasculitis associated with inflammatory bowel disease, or with other rheumatologic diseases such as reactive arthritis and systemic lupus erythematosus, clinicians should take care to consider infectious etiologies even in patients with known autoimmune conditions. In our case, a broad differential and attention to histologic findings helped to uncover a diagnosis of syphilis.
If syphilis is suspected, diagnosis is usually made via serologic testing. Two serologic tests are required for a presumptive diagnosis of syphilis, a nontreponemal test and a treponemal test. 2 Definitive diagnosis can also be established by histology and immunostaining of biopsied tissue as was the case in our patient. Penicillin G is the standard of care for patients with all stages of syphilis. While few cases of occupational and other non-sexual transmission have been reported, 8 care should be taken to use correct personal protective equipment and hand hygiene, especially when a communicable disease is suspected. This case highlights that a broad differential should be considered in patients who present with recurrent oral ulcers, including autoimmune and infectious causes such as oral syphilis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.