
Abstract
We hereby present a rare case of laryngeal zoster presenting with unilateral odynophagia and hemifacial pain in an immunocompetent host. Visualization of the characteristic vesicles is challenging given their short-lived and at times delayed appearance; thus, laryngeal zoster may be a largely unrecognized cause of laryngitis and cranial neuropathies. Heightened awareness may improve prompt diagnosis, referral and initiation of antiviral therapy, while guiding patient counselling on the associated long-term sequelae such as voice and swallowing impairments, and post-herpetic neuralgia.
Case Description
A 24-year-old male known for untreated ulcerative colitis (no immunomodulators for the past year) and well-controlled schizophrenia presented to the emergency department with a 5-day history of left-sided odynophagia and throbbing hemifacial pain. He had no infectious symptoms, no history of trauma, and denied any dysphagia, dyspnea, or dysphonia. Interestingly, he had seen a community dentist the day prior who had initiated a course of acyclovir empirically given the unilaterality of symptoms, despite no visible intra-oral or facial lesions. Nasolaryngoscopy revealed vesicular lesions along the left lateral pharyngeal wall, base of tongue, and laryngeal inlet with normal vocal fold mobility. The contralateral side remained strikingly uninvolved, as evidenced by epiglottic erythema solely to the left of the midline (Figure 1). Nasolaryngoscopy revealing erythema of the left hemi-epiglottis and white vesicular/ulcerated lesions along the left lateral pharyngeal wall, base of tongue (A), and mucosa overlying the left arytenoid and aryepiglottic fold (B).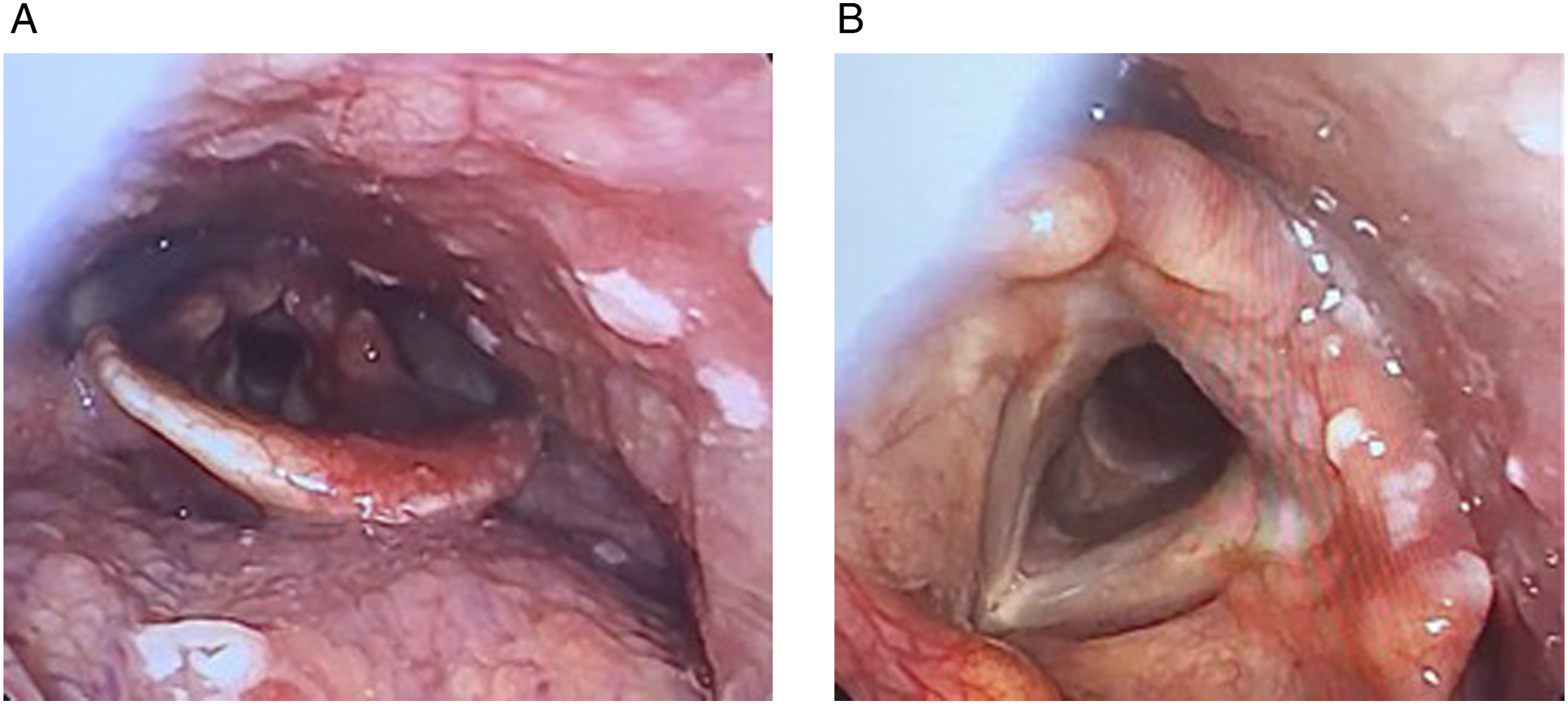
A presumptive clinical diagnosis of laryngeal zoster involving the glossopharyngeal and vagal nerves was made, and was later confirmed by polymerase chain reaction (PCR) testing of a base of tongue unroofed vesicle. The patient was treated with oral antivirals and supportive care (analgesia and anti-emetics). Unfortunately, he returned 2 weeks post-initial presentation with intractable coughing episodes and post-tussive emesis with limited oral intake, requiring a brief admission for enteral nutrition and optimization of pain management. Repeat nasolaryngoscopy at this time revealed complete resolution of the previously seen vesicles. We suspected neurogenic hypersensitivity and recommended a trial of low-dose amitriptyline (initially 10 mg daily, tapered up to 30 mg daily over 3 weeks). At 4-month follow-up, he noted full resolution of symptoms and had hence since stopped the medication.
Discussion
The varicella-zoster virus (VZV) usually lays dormant in dorsal root ganglia after primoinfection, but may reactivate in the context of impaired or waning cellular immunity (immunodeficiency or advanced age), psychological stress or physical trauma. 1 It characteristically causes severe, burning pain in a dermatomal distribution accompanied by a pathognomonic vesicular rash in the territory of the affected nerve root. 2
Pharyngolaryngeal involvement, termed herpes zoster laryngitis, is a rare presentation of VZV and may occur in conjunction with other cranial neuropathies or as an isolated phenomenon. In the largest review cumulating 54 cases, odynophagia, dysphagia, and hoarseness were predominant clinical features. 3 Although sensory symptoms prevailed, almost half of all patients had associated hemilaryngeal or pharyngeal paresis. Pharyngolaryngeal dysfunction was objectified in 11 of 20 patients in whom a videofluoroscopic swallowing study was obtained.
Laryngeal zoster poses a unique diagnostic challenge, as symptoms may mimic a typical viral laryngitis, and prompt endoscopic examination is infrequently performed during the short-lived course of the typical mucosal eruption. 4 Viral genome detection by PCR is the most commonly used laboratory method to confirm the diagnosis, with high sensitivity and rapidly available results, and has therefore largely surpassed conventional serologic testing for IgM and IgG antibodies against VZV. 2 Although elevated IgM titers also confirm the diagnosis, they may be falsely negative and typically only appear 8-10 days after the eruption. IgG antibodies rise 4-6 days after the vesicular rash and peak 3 weeks later, but lack specificity and are thus of little clinical utility. 1 Imaging is seldom obtained unless there is an associated vocal fold or facial paralysis; however, if performed, magnetic resonance imaging may show enhancement of the affected cranial nerve. 3
The mainstay of treatment remains symptomatic management and early antiviral therapy (ideally within 72 hours of symptom onset) to hasten healing of the mucosal lesions and reduce the severity/duration of pain.3,5 Adjunctive high-dose steroids remain controversial, yet some authors postulate they may decrease the risk of post-herpetic neuralgia. 6 Given the lack of substantial evidence, the potential benefit should be weighed against their known deleterious effects, particulary in patients with diabetic or psychiatric comordbidities.
Unfortunately, full recovery rates remain poor, and the majority of patients may have persistent deficits, including voice and swallowing sequelae, with significant impairment of their quality of life. 3 Similarly to our patient, Ling et al 7 reported 2 cases of chronic cough after laryngeal zoster reactivation, hypothesized to result from sensory hyperesthesia by a mechanism akin to post-herpetic neuralgia. Neuromodulators such as gabapentin and amitriptyline in subtherapeutic doses have been used by otolaryngologists for idiopathic chronic cough. 8 Conceptually, they may help dampen the aberrant sensory stimulus and thus add to our therapeutic armamentarium.
In summary, laryngeal zoster is a rare, likely underdiagnosed cause of laryngitis. Prompt endoscopic visualization should be sought in patients with odynophagia, hoarseness and characteristically unilateral symptoms to guide early diagnosis and treatment initiation. This case additionally highlights a potential role for neurogenic medications in post-herpetic cough, although this has yet to be formally studied.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.