
Abstract
The reported donor site morbidity of the fibula free flap (FFF) is low; however, several uncommon complications have been reported with tibia fracture rarely being reported. We present a case of a pathological tibial fracture in the setting of chronic osteomyelitis after FFF. A 54-year-old female presented with a benign fibro-osseous lesion of the right mandible and was treated with mandibulectomy and reconstructed with a left FFF. Approximately 1 year following surgery, the patient presented to the emergency department. Imaging showed a pathological fracture of the distal third of the tibial shaft with persistent erythema and cellulitis of the lateral prior graft harvest site without signs of systemic infection. She was taken to the operating room for irrigation and debridement with culture and biopsy as well as external fixation of the tibial fracture. Intraoperative biopsy and culture demonstrated fracture site change with callus formation and negative culture. The patient was discharged on 6 weeks of IV vancomycin and ceftriaxone. In conclusion, tibial fracture following FFF is an uncommon complication, yet it can be exacerbated by chronic osteomyelitis. This report highlights the importance of close observation and comprehensive wound care of donor sites after free flap harvest for head and neck reconstruction.
Introduction
Vascularized fibula free flaps (FFFs) are commonly utilized in head and neck reconstructive surgery for their versatility and reliability, offering a large bony segment that may be segmented for anatomic mandibular reconstruction, a long pedicle length, and a skin paddle.1,2 FFFs have success rates over 95% and low donor site morbidity. However, uncommon complications have been reported and include wound infection, osteomyelitis, ankle valgus deformity, lateral lower leg and dorsal foot numbness, toe and ankle movement restriction, gait abnormality, pain, hematoma, and chronic edema.2,3 A further less recognized potential complication of fibular harvest is a fracture of the tibia with few cases reported in the literature.1-10
Although the tibia is the primary weight-bearing bone in the lower limb, the fibula accounts for about 15% of leg load. 1 Fibula free flap harvest increases the stress on the ipsilateral tibia, which typically has a negligible effect on patient health and lifestyle. 4 Wound infection can lead to osteomyelitis and subsequent bony destruction, and weakening of the affected bone that may persist beyond treatment. This lowers the threshold for fracture.11,12 Here, we report an unusual case of delayed pathological tibial fracture in the setting of chronic osteomyelitis after FFF. The Thomas Jefferson University Institutional Review Board does not review case reports of less than 3 patients.
Case presentation
A 54-year-old obese female presented with a cemento-ossifying fibroma of the right mandible (Figure 1). She underwent segmental mandibulectomy and reconstruction with a left fibula free flap including a 6 × 20 cm cutaneous paddle. There were no apparent complications during the procedure. Postoperatively, the patient recovered well during her hospital stay. At her 1-week postoperative visit, she was stable without complaint or sign of infection. At her 3-week postoperative visit, her leg incision demonstrated expected erythema and partial loss of the skin graft with granulation. Pre-resection and post-reconstruction imaging. CT scans depicting the patient’s cemento-ossifying fibroma of the mandible (pre-resection, A) requiring resection and fibula free flap reconstruction (post-reconstruction, B).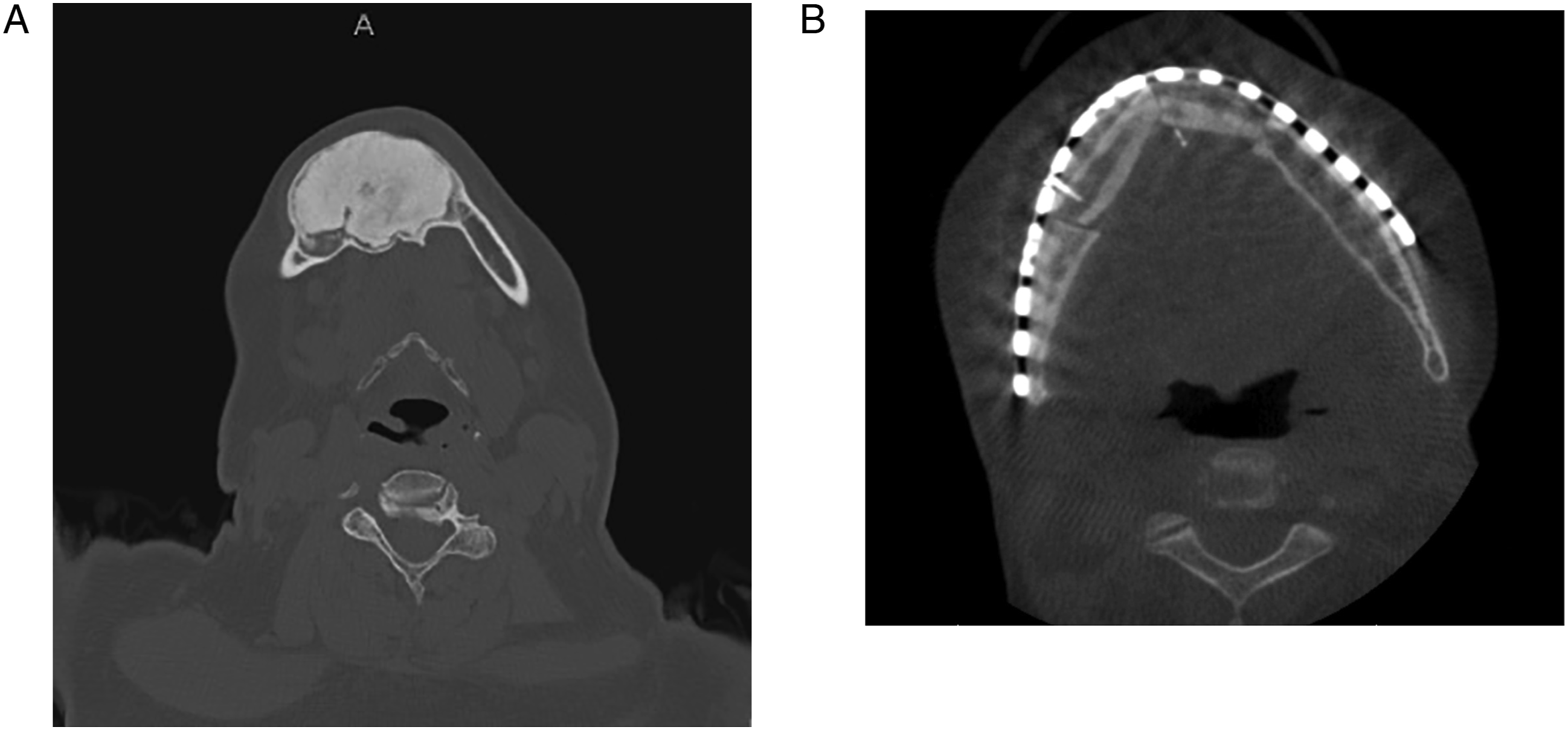
She presented to the emergency department (ED) 1 month later with 3 days of cellulitis, pain, and swelling of the FFF donor site. On x-ray imaging, there was periosteal reaction and cortical irregularity along the proximal fibular diaphysis resection margin with overlying soft tissue swelling and edema concerning for osteomyelitis (Figure 2A). Blood cultures were negative. She was treated with 1 dose of intravenous (IV) clindamycin while in the ED and then IV vancomycin and cefepime during her 3-day admission. Per infectious disease, she was discharged on 2 weeks of oral sulfamethoxazole-trimethoprim. Follow-up visits in clinic showed decreasing size of the donor site wound to a 3 by 6 cm area of granulation with further local wound care. AP and lateral view x-rays prior to and after tibial fracture. (A) Two months after FFF at time of initial presentation with osteomyelitis. Radiology report at this time said, “There is periosteal reaction and cortical irregularity along the proximal fibular diaphysis resection margin. There is overlying soft tissue swelling and edema. These findings are compatible with osteomyelitis.” (B) Thirteen months after FFF at time of presentation with tibial fracture. Radiology report at this time said, “Acute, comminuted fracture of the distal tibia with lateral angulation.” (C) One month after presentation of tibial fracture and subsequent treatment with external and internal fixation. Radiology report at that time said, “External fixator in place with 2 pins traversing the proximal tibial shaft, and 2 through the distal diametaphyseal region. Alignment of the tibial fracture is now anatomic, with a small lateral butterfly fragment displaced by approximately 5 mm.” (D) Ten days after placement of external fixator and subsequent removal of external fixator. Radiology report at this time said, “Interval placement of a transtibial nail with antibiotic beads placed at the distal tibial diaphysis fracture fragment. Wound VAC projects over the lateral aspect of the leg.”
Approximately 1 year following surgery, the patient was seen by her primary physician with a complaint of increasing pain and erythema around the lateral leg region for 10 days and was prescribed a 10-day course of cefalexin. Subsequently, she presented to the ED with increased pain and was found to have a 10 × 6 cm area of induration with scar and eschar. She was admitted to the hospital. On x-ray of the tibia and fibula, there were stable postsurgical changes with mild nonspecific edema throughout the lower extremity. There were no cortical erosions to suggest osteomyelitis and no evidence of fracture. Given her recent history, she received intravenous clindamycin for 1 day with improvement of erythema on exam. She was discharged with a 7-day course of oral clindamycin.
The patient returned to the ED 11 days later after standing up at home and feeling her leg “pop” and “give way.” She was admitted with an atraumatic pathological closed displaced transverse fracture of the distal third of the tibial shaft in the setting of cellulitis of the prior fibular graft harvest site, chronic osteomyelitis of the tibial bone, and no signs of systemic infection (Figure 2B). She was taken to the operating room for irrigation, debridement of non-healing, devitalized soft tissue and bone, and external fixation of the tibial fracture (Figure 2C). Biopsy taken intraoperatively demonstrated fracture site change with callus formation. Wound cultures were negative, however; given the findings, the patient was discharged on 6 weeks of IV vancomycin and ceftriaxone.
The patient was taken back to the OR on postoperative day 10 for removal of the external fixator as well as repeat irrigation and debridement with VAC closure and definitive intramedullary nail fixation of the pathological fracture (Figure 2D). To date, the fracture has fully healed, and the chronic wound issues have resolved. There was no persistent evidence of any infection. The patient was able to be independent with all mobility and gait while wearing a controlled ankle movement (CAM) boot.
Discussion
Tibial fracture following fibula free flap harvest for reconstruction of head and neck defects has been reported in 14 other individual patients.1-10 The underlying etiologies of the other cases have mostly been stress fractures without an infectious component.1-10 It has been shown that donor-side tibial adaptation includes deposition of new bone mainly in the interosseous space and replacement of some of the bony area lost with fibula resection; however, this adaptation is incomplete, and the newly formed bone does not meet normal cortical bone mineral density values. 11 However, the spontaneous stress fractures in the donor-side tibia that have been discussed in the literature occurred after a short postoperative timeframe of 116 months when the tibial adaptative remodeling was still likely incomplete.3-11 This patient experienced an atraumatic tibia fracture after receiving FFF 13 months prior. This patient’s presentation was unique in that the fracture occurred after a delayed presentation after presumed prolonged chronic osteomyelitis. The inciting cause of cellulitis is not entirely clear as most donor sites heal with or without skin graft loss uneventfully; however, in this case, recurrent cellulitis developed perhaps due to other risk factors such as morbid obesity (patient BMI = 39.94 kg/m2).
Chronic osteomyelitis is defined as a bone infection lasting 6 or more weeks and is known to increase susceptibility to fractures due to bony destruction.12,13 Chronic osteomyelitis has been reported at a rate of 15% after closed and 350% after open fractures. 14 Treatment of osteomyelitis involves initial nonsurgical treatment with appropriate wound care and IV antibiotics; however, in serious cases resulting in sepsis or bony instability, treatment may include surgical irrigation, debridement, stabilization, and soft tissue reconstruction.12,15 Similarly, the patient presented here received irrigation, debridement, and fixation of the tibial fracture along with biopsy and culture testing. She was discharged on IV antibiotics due to high clinical suspicion given a prolonged and relapsing infectious course despite negative intraoperative culture. The patient has not had any other complaints or further interventions in the lower leg in follow-up. In the setting of chronic or recurrent donor infection after FFF, the possibility of deeper underlying infection, osteomyelitis or risk of pathologic fracture should be considered.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author’s Note
Presented at the American Head and Neck Society 10th International Conference on Head and Neck Cancer, Virtual, July 22, 2021.