
Abstract
Coronavirus disease 2019 (COVID-19) is a pandemic with a variety of symptoms and complications. Impairments of taste and smell caused by COVID-19 are well known as otolaryngological sequelae. However, dysphonia due to bilateral vagal neuropathy has not been well described as a presenting symptom or complication of COVID-19 infection. In this paper, we report a case of a 47-year-old patient who experienced dysphonia after remission of COVID-19 infection and diagnosed bilateral vagal neuropathy.
Introduction
COVID-19 disease, caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is the first pandemic of the twenty-first century. SARS-CoV-2 uses the angiotensin-converting enzyme 2 (ACE2) receptor to infect cells, after which it injures many organs and triggers complications. 1 Neurological symptoms are evident in 36% of patients with COVID-19 infections 2 but, to the best of our knowledge, the report of vagal neuropathy presenting with dysphonia has not been well reported after COVID-19 infection.
We present here a case who experienced dysphonia after remission of COVID-19 infection. Bilateral vagal neuropathy was evident on laryngeal electromyography (L-EMG). The symptoms were successfully controlled via bilateral vocal fold injections.
Case
A 47-year-old female had been diagnosed with COVID-19 3 months before visiting us, but made a complete recovery as confirmed by negative RT-PCR conversion without special treatment. Starting from COVID-19 remission, she had experienced vocal discomfort and visited our otolaryngology outpatient department. The patient had no other medical history, no history of intubation, and no structural abnormalities on computed tomography of the larynx and hypopharynx. However, on videostroboscopic examination vocal fold (VF) tension was decreased, accompanied by incomplete glottic closure and a severely breathy voice (Figure 1). To clarify the cause of bilateral vocal cord paresis, we performed neurologic examinations, serologic tests to identify systemic diseases like diabetes and autoimmune diseases, and computed tomography of the chest to identify the sarcoidosis. All results showed no specific findings. Laryngeal electromyography (L-EMG) revealed that the interference patterns of the bilateral thyroarytenoid and cricothyroid muscles were reduced, reflecting bilateral vagal neuropathy. We presumed it was related to the neurological sequelae from a COVID-19 infection. The fiberolaryngoscopic image. (a) Reduced VF tension and incomplete glottic closure during “E” phonation were observed. (b) The glottic gap and VF tension improved after injection of calcium hydroxyapatite. (c) One month later.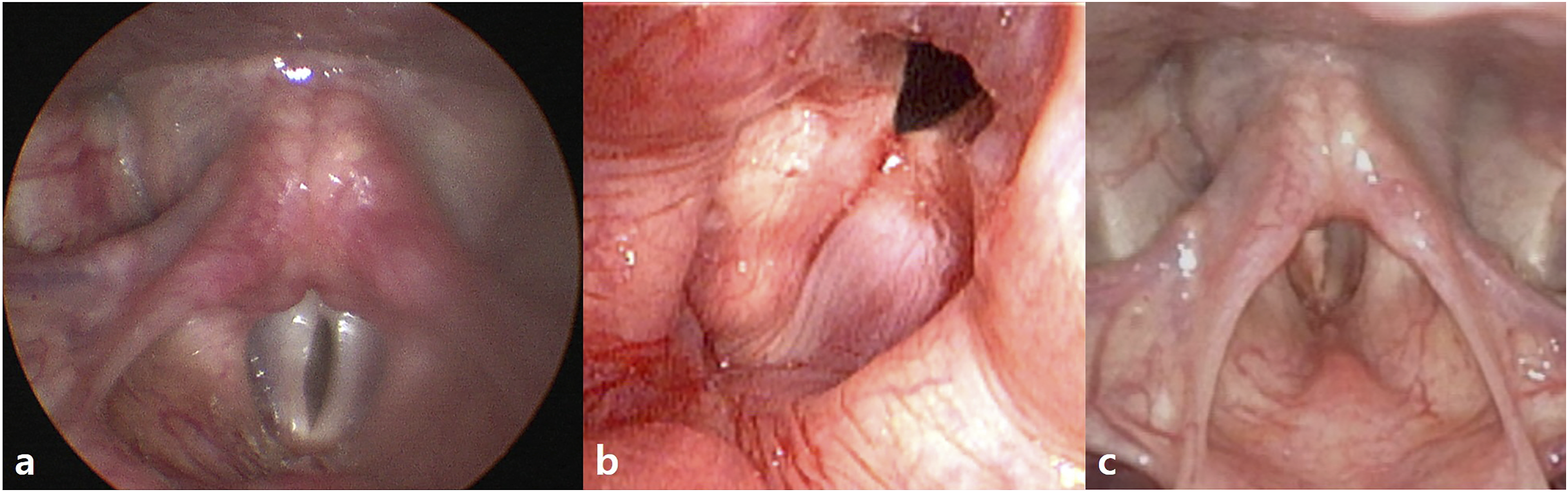
Voice analysis pre-operation and 1 month after treatment.
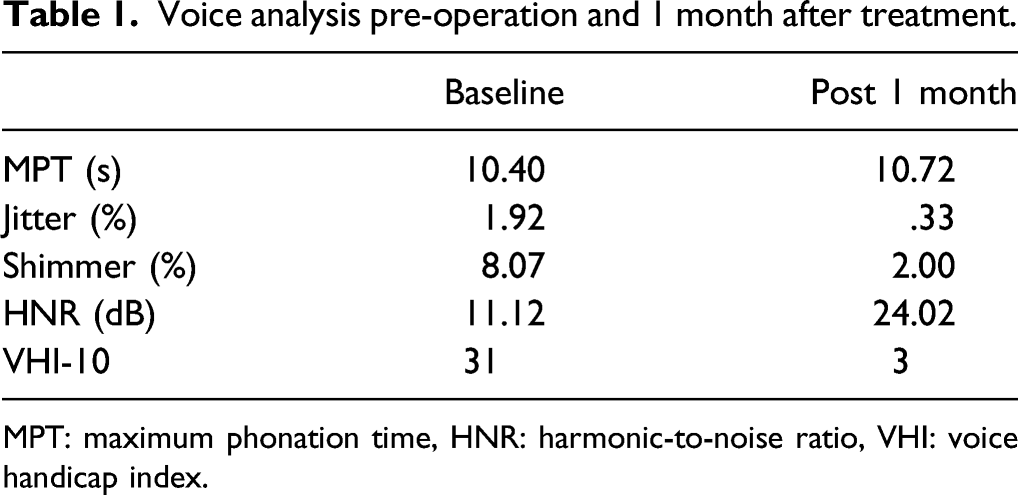
MPT: maximum phonation time, HNR: harmonic-to-noise ratio, VHI: voice handicap index.
Discussion
The neurological manifestations of COVID-19 include central nervous system (CNS), peripheral nervous system (PNS), and skeletal muscular manifestations. Mao et al. reported that taste and smell impairments as CNS manifestations were the most common neurological problems; these are well known to trigger otolaryngological complications. 2 The pathophysiology of neurological symptoms reflects penetration by the SARS-CoV-2 virus of the cribriform lamina of the ethmoid bone; the virus thus enters the nervous system. 3 Recently, Sarah K. Rapoport et al. reported a case series of vocal fold paresis and paralysis after COVID-19 infection, which was thus suggested to have caused by post viral vagal neuropathy. 4 The distinct mechanism is not yet known.
In our case, L-EMG revealed decreased interference patterns in the bilateral thyroarytenoid and cricothyroid muscles, reflecting viral invasion of the superior and recurrent laryngeal nerves, 5 triggering bilateral vagal neuropathy. Vagus nerve injury may be caused by operation, intubation, a malignancy, systemic, and autoimmune diseases and viral infections. 6 Her only relevant history was COVID-19 infection. This made it reasonable for us to presume her symptoms as neurological sequelae from a COVID-19 infection. We injected calcium hydroxyapatite into both vocalis muscles to improve glottal contact and VF tension; the dysphonia symptoms resolved.
Conclusion
Impairments of taste and smell caused by COVID-19 are well known as otolaryngological sequelae, but dysphonia by vagal neuropathy is relatively unknown. To the best of our knowledge, this is the first case report of bilateral vagal neuropathy accompanied by dysphonia after recovery from COVID-19 infection. Therefore, since there is a possibility of vagal neuropathy as neurological sequelae from a COVID-19 infection, we suggest that otolaryngologists should carefully examine and treat patients with dysphonia after recovery from COVID-19 infection. It is also recommended to consider appropriate treatment depending on the severity of symptoms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Soonchunhyang University Research Fund.