
Abstract

Ménière’s disease (MD) is characterized by attacks of two or more spontaneous episodes of vertigo, fluctuating low-to medium-frequency sensorineural hearing loss, and fluctuating aural symptoms within 24 hours of the vertigo episode. The most recent diagnostic criteria were published in 2015. 1 Vertigo can be controlled by various therapies, but fluctuating and progressive hearing loss tends to be resistant to treatment. 2 Description of the long-term hearing characteristics of MD dates back to 1967. Fluctuations were recorded in approximately half of the patients, regardless of the duration of the disease, and were more common with rising and trough curves. The average total hearing loss was 52 dB, which progressed most rapidly during the first year. 3 Subsequent follow-up revealed progressive hearing loss in 55.5% of cases of MD, with likely progression during the first five years of the disease.4,5 Few studies have also indicated that approximately 52.7% of patients have poor prognosis in hearing, 6 and there is a certain coincidence and parallelism in the clinical course of vestibular and cochlear damage.
Migraine has a close connection with MD, with substantial overlap between the symptoms and signs of the two conditions.7,8 The diagnostic criteria of vestibular migraine (VM) include episodes with vestibular symptoms, history of migraine, and migraine features with at least 50% of the vestibular episodes. 9 Hearing loss is generally not viewed as a characteristic presentation of VM. Fluctuating or progressive hearing loss can occur in up to 25% of VM cases.8,10 Patients with VM may show hearing loss, but it is mild with slow progression. 8
Over the past five years, many patients in our clinic have fulfilled the current diagnostic criteria for MD.
1
However, only a certain portion of these patients have shown progression to moderate-to-severe hearing loss. On the basis of our long-term clinical experiences, we further divided the patients with MD into the following two groups: the primary MD (pMD) group, which consisted of patients who had no clinical characteristics of migraine, and the migraine-related MD (mMD) group, which included those who had a strong association with migraine attacks or constituents. Each group comprised approximately half of the included patients (estimated 300 cases in total). With respect to the progression and outcome of hearing loss, we found that patients with pMD exhibited moderate-to-severe hearing loss within 5-10 years. We hypothesize that the underlying etiology is confinement of the disease to the inner ear and impaired homeostasis of inner ear fluids, such as in endolymphatic hydrops, which is still considered to be the main pathophysiological background for MD. Approximately 50% of our patients who were initially diagnosed with MD belonged to this group. This is consistent with the results of earlier studies.4-6 On the other hand, in patients with mMD, hearing loss tended to fluctuate for a very long time, was less severe and, in some cases, returned to normal during long-term follow-up. However, we noticed that hearing loss was irreversible in certain patients with mMD, who experienced more severe and frequent attacks, especially those with more severe hearing loss than 50 dB. The possible mechanism underlying mMD is the presence of an additional pathophysiology in which the auditory system is less affected, which could involve the trigeminovascular system and direct central activation of the vestibular centers. Only the patients with a more severe inflammation, induced by this top-down mechanism, are likely to experience irreversible damage to the hearing organs. Two examples of serial audiograms in the pMD (case 1) and mMD (case 2) are shown in Figure 1. Hearing of case 1 gradually deteriorated, and the most recent audiograms showed a moderate sensorineural hearing loss over the affected side. Hearing of case 2 kept fluctuating and returned to nearly normal level. There are few other clinical features based on our observations that differ between pMD and mMD, which could also help to predict hearing outcomes. Patients with mMD are predominantly women (female:male ratio, 4:1), tend to be younger, and affected bilaterally. High-frequency hearing was affected earlier and was more severe in patients with mMD. Serial audiograms of an example case of pMD (case 1) and mMD (case 2). Case 1 is a 62-year-old male, who was diagnosed with MD 20 years ago. His hearing gradually deteriorated in 5 years, and the most recent audiograms in 2019 show a moderate sensorineural hearing loss over the affected side. Case 2 is a 41-year-old female case of MD diagnosed 5 years ago. Her hearing kept fluctuating and returned to nearly normal level (except at high frequencies) in 2021 (red lines and symbols indicate hearing of the right ear; blue ones indicate that of the left ear. ○ : right air conduction threshold; x or □ : left air conduction threshold; < : right bone conduction threshold ; > or ] : left bone conduction threshold).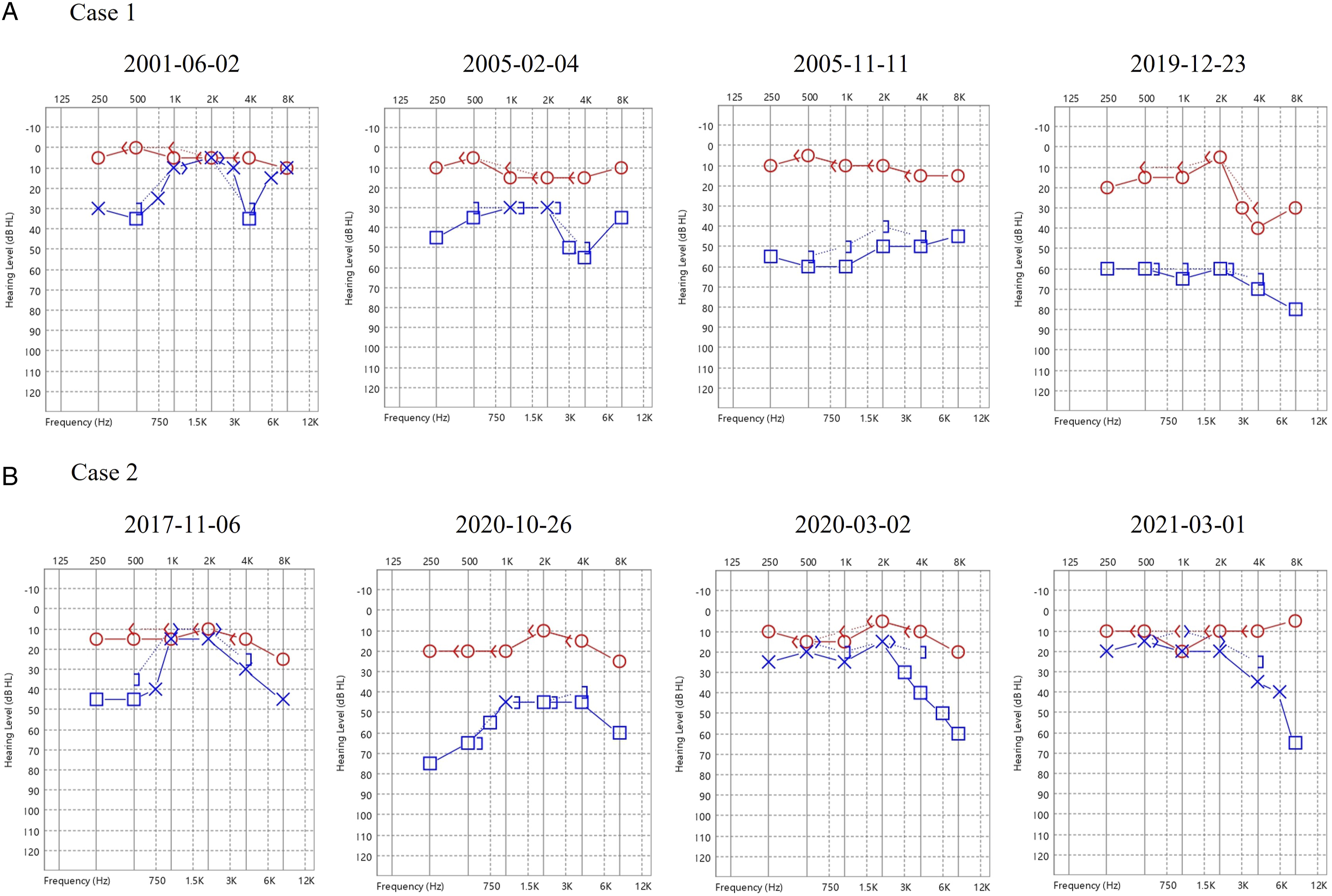
It would be beneficial if the long-term hearing outcome could be estimated or predicted for patients diagnosed with MD in the early stages. Not all patients with MD experience irreversible hearing loss. Long-term outcomes and progression of hearing loss in MD warrant further investigation. Whether lifestyle modifications or prophylactic migraine therapy can slow down or prevent the progression of hearing loss in patients with mMD requires further research.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.