
Abstract

Significance Statement
Postoperative wound dehiscence following Weber-Ferguson or lateral rhinotomy incisions can produce sinocutaneous or nasocutaneous fistulas (NC-SCFs). We present a technique in addressing these defects, utilizing a turn-in flap followed by a 2-stage paramedian forehead flap to close NC-SCF in the periorbital region. NC-SCFs present reconstructive challenges following maxillectomy with postoperative wound dehiscence. The utilization of multiple local flaps in a double-layer soft tissue closure obliterates NC-SCFs while providing satisfactory cosmetic outcomes.
Clinical Case
Patients with a classic postoperative late wound dehiscence and subsequent through-and-through NC-SCF defect with healed edges of the lateral nasal wall and periorbita presented to the clinic (Figure 1a). Risks vs benefits of double-layer local flap closure were discussed at length, and both patients agreed to proceed forward with intervention. Under general anesthesia, a turn-in flap is then designed immediately adjacent to the defect and opposite to the orbit in a region of healthy cutaneous tissue, taking into account inevitable minor tissue shrinkage with flap elevation. All edges of the fistula are then freshened with the 15-blade scalpel with the exception of the edge adjacent to the designed flap as to avoid jeopardizing the blood supply along the base of the flap. The turn-in flap is then incised sharply and elevated in a subcutaneous plane, exercising caution to maintain the blood supply along the base of the flap; bipolar cautery is judiciously used for hemostasis (Figure 1b). The flap is then folded into the fistulous defect, with the cutaneous side facing into the sinus or nasal cavity, and subsequently seated into place, utilizing resorbable sutures (4-0 vicryl is our preference). This inherently creates an external defect approximately twice the size in surface area of the initial fistula, which must now be addressed (Figure 1c). As such, the newly created wound bed is measured, and a paramedian forehead flap is subsequently designed and elevated in standard fashion.
1
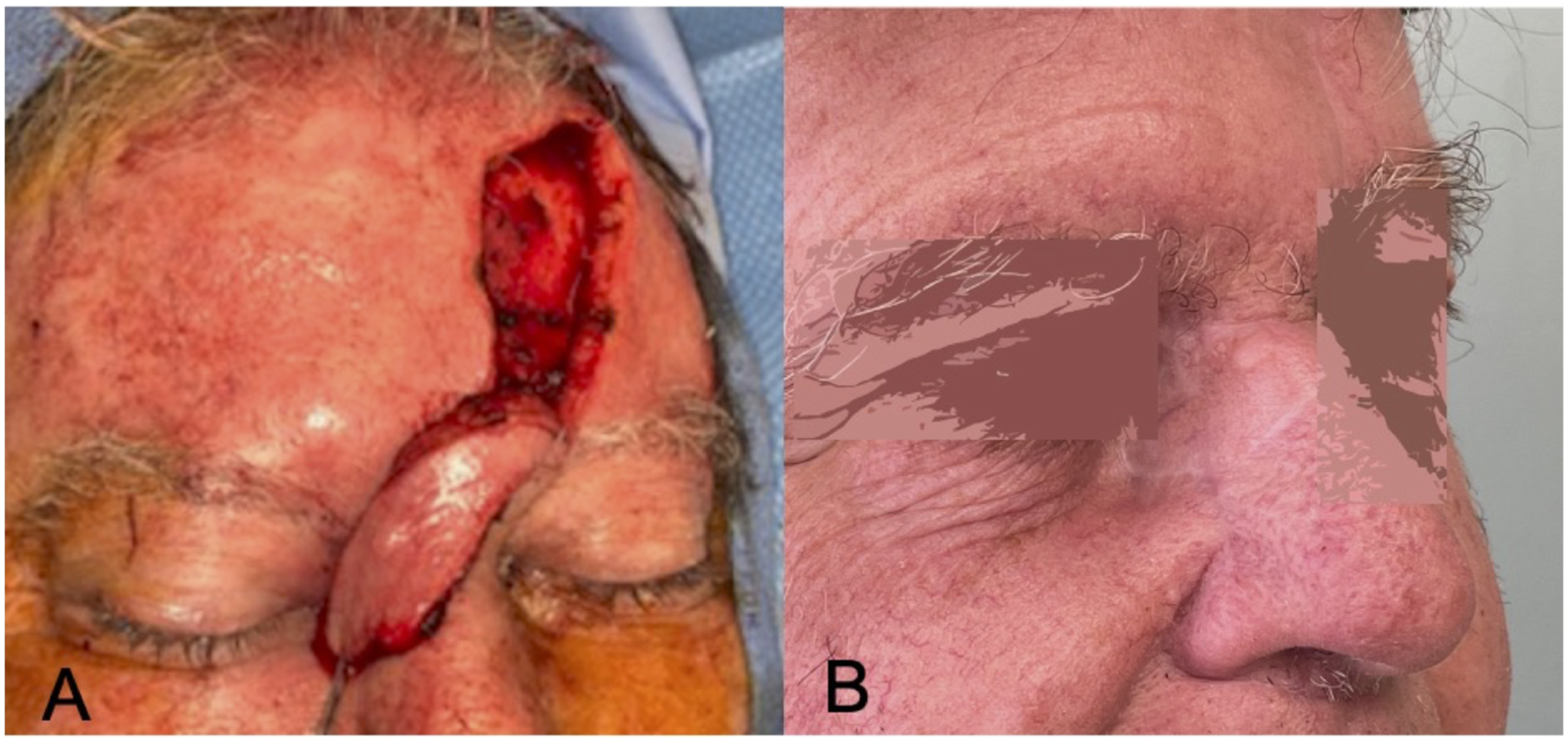
We prefer to base the flap on the contralateral supratrochlear artery for repair of these defects as it decreases the axis of rotation and thus, torsion of the flap pedicle. Additionally, the close proximity of the defect to the flap base enables the flap to reach its distal aspect with ease. The paramedian forehead flap is rotated into the defect and subsequently seated into place in a 2-layer closure (Figure 2a). The donor site for the forehead flap is then closed primarily as much as possible; if the donor site is unable to be closed completely, a xeroform bolster is placed over the remaining wound bed to facilitate granulation and healing. The patient is brought back to clinic at 1 week postoperatively for a wound check and gentle reinforcement of postoperative recommendations, which included avoiding nose-blowing and sneezing with the mouth open; patients are then subsequently brought back to the operating room approximately 3 weeks following initial intervention for pedicle division, takedown, and flap contouring. Follow-up in clinic is arranged to ensure that the flap remains viable after pedicle division (Figure 2b). The contour and healing of the donor and recipient sites are also assessed at this time. (A) Through-and-through defect from previous lateral rhinotomy incisional dehiscence communicating to the sinonasal cavity. (B) Full thickness incision shown with tissue flap being prepared for transposition into the posterior aspect of the defect. Obliteration of the communication to the sinonasal cavity is achieved with this tissue rearrangement. (C) Local tissue flap reflected along its base, closing the defect. (A) Paramedian forehead flap from the contralateral side was designed and elevated in a superior to inferior manner with the pedicle based in the approximate region of the supratrochlear artery’s origin from the orbit. The paramedian forehead flap is rotated counter clockwise along its pedicle to cover the entire cutaneous defect. (B) Follow-up after the paramedian forehead flap pedicle division indicating healed donor and recipient sites.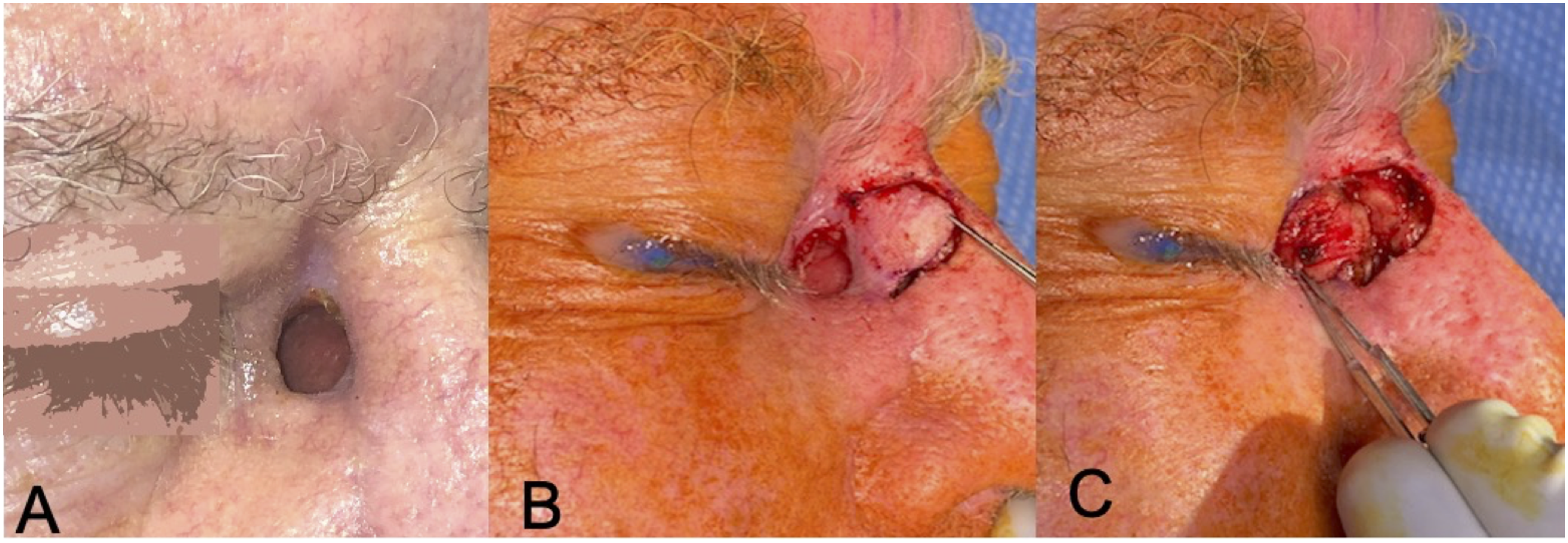
Discussion
Maxillectomy has been and continues to be the gold standard for extirpation of advanced sinonasal malignancies of the maxillary sinus, and is generally performed via Weber-Ferguson incision or lateral rhinotomy incision with or without supraorbital extension for increased lateral exposure.2-4 Reconstruction of maxillectomy defects is known to be complex in nature and as such carries a number of complications. 5 Of these complications, development of postoperative nasocutaneous or sinocutaneous fistulas (NC-SCF) is particularly difficult to treat and known to occur in an estimated 5-15% of patients, regardless of mechanism of reconstruction.6,7 The defect ubiquitously occurs in close proximity to the orbit, produces a readily noticeable and undesirable cosmetic appearance, and often causes discomfort in the adjacent eye—if preserved during the ablation—during sneezing and breathing. The absence of underlying bony support and high rate of adjuvant radiation therapy (XRT) seen in this patient population not only puts these patients at increased risk for development of NC-SCF but also prevents spontaneous healing, with definitive defect closure often requiring free tissue transfer.8,9 We present the above simple technique utilizing two local flaps for internal mucosal lining and external skin reconstruction with bi-layered closure for definitive repair of postoperative NC-SCF following maxillectomy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent for patient information and images to be published was provided by the patient.