
Abstract

Significance Statement
The normal sublingual gland (SLG) or sublingual lesions may pass through the defect of the mylohyoid muscle to reach the submandibular space. Although SLG herniation which is a pseudo lesion is not commonly included in the differential diagnosis of the submandibular lesion, recognition of mylohyoid muscle defect and the typical radiologic appearance of SLG herniation can allow differentiation from other pathologic lesions, and prevent unnecessary surgery.
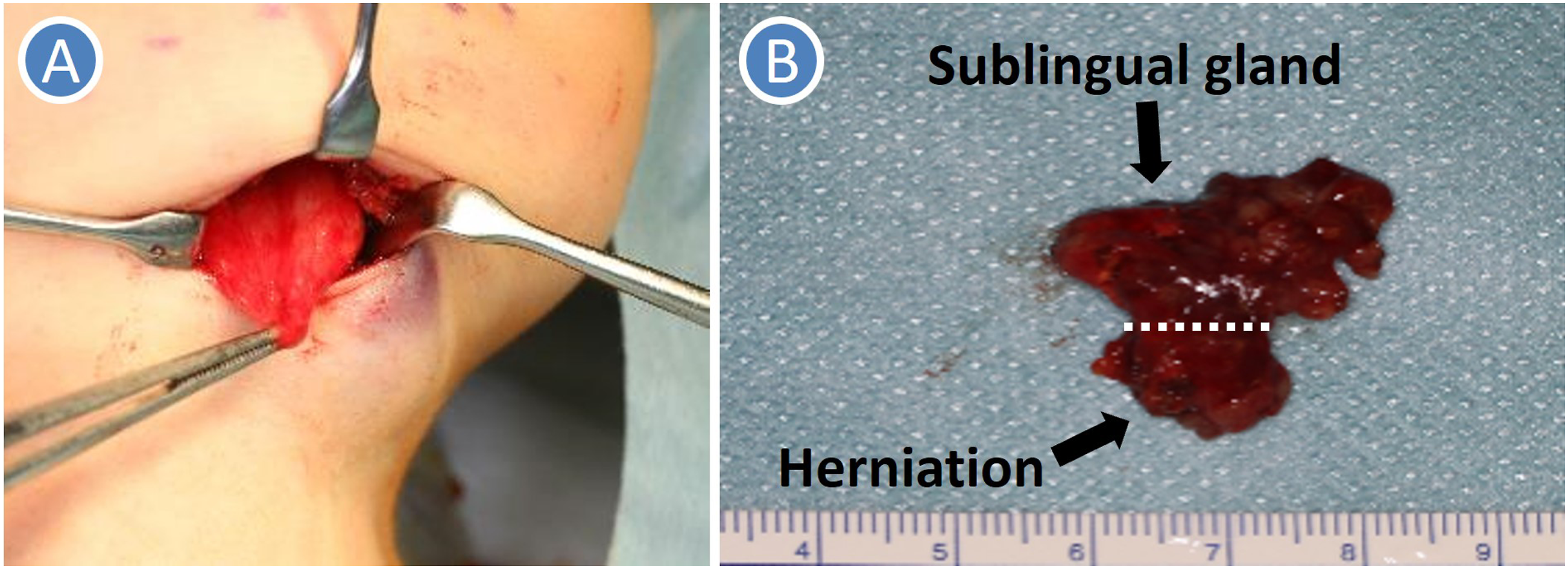
A 22-year-old woman was referred to our department with a painless swelling in the right submandibular region. The elastic hard mass was mobile in the bimanual palpation. The mucosa of the oral floor was normal. Computed tomography (CT) showed a well-circumscribed, heterogeneous lesion (33×21×17 mm) in the right submandibular region (Figures 1(A) & 1(B)). Magnetic resonance imaging (MRI) showed a right submandibular lesion with heterogeneous signal intensities in T1-weighted images (Figures 1(C) and 1(D)), homogeneous high-signal intensity in T2-weighted images (Figures 1(E) and 1(F)). Ultrasonography revealed that heterogeneous cystic lesion with blood supply and the defect of the mylohyoid muscle (Figures 1(G) and 1(H)). Fine needle aspiration cytology showed a benign tumor. The lesion was diagnosed radiologically as a benign sublingual gland (SLG) tumor with a cystic component through the defect of the mylohyoid muscle and was removed under general anesthesia. Yellow mucus leaked from the lesion during extraoral dissection in the submandibular approach. Because there was definitive continuity between the submandibular lesion and SLG, the SLG with the lesion was removed completely in the intraoral approach (Figure 2). The pathological diagnosis of the specimen was SLG inflammation. Finally, we diagnosed the lesion as SLG herniation with a cystic component (intraglandular mucous retention cyst) through the mylohyoid muscle defect. A: CT (Axial image), B: CT (Coronal image), C: MRI (T1-weighted axial image), D: MRI (T1-weighted coronal image), E: MRI (T2-weighted axial image), F: MRI (T2-weighted coronal image). G: US (B-mode), H: Doppler US. Arrow indicates lesion. Arrowhead indicates a defect of the mylohyoid muscle. A: Intraoperative view, B: The removed specimen.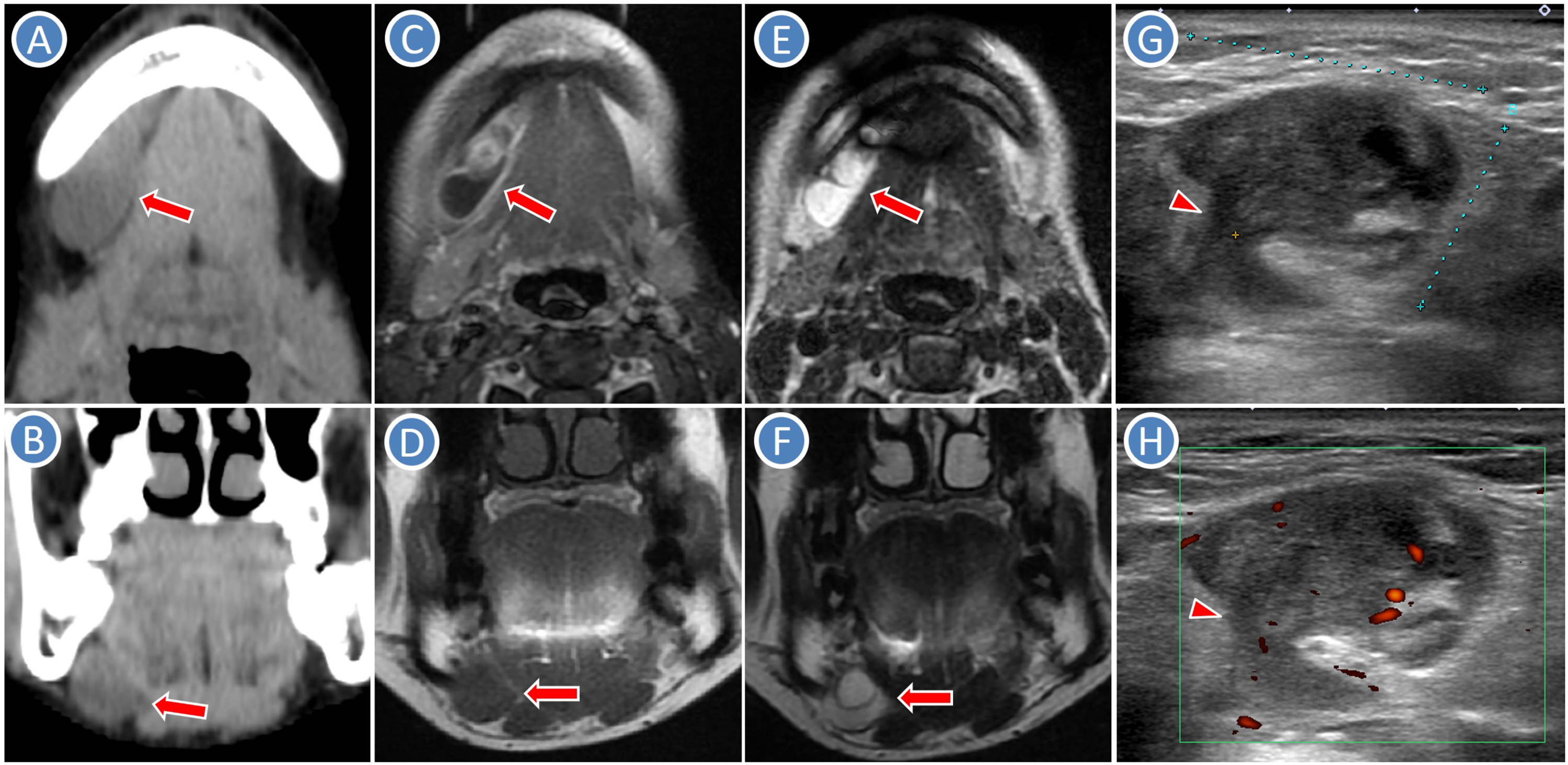
The mylohyoid muscle separates the sublingual space from the submandibular space. During embryological development, the anterior and posterior muscular sheets fail to overlap with a resultant slit, 1 and the normal SLG or sublingual lesions can pass through this defect of the mylohyoid muscle to reach the submandibular space.1,2 Also known as the mylohyoid boutonniere, the protruding SLG, fat, blood vessels or a combination of them can present as a palpable mass (pseudo lesion). 1 Most defects of the mylohyoid muscle are less than 5 mm, whereas occasionally they may be larger than 2 cm. 3 Therefore, larger herniations may be mistaken both clinically and radiologically for pathologic abnormalities. 3
A portion of the SLG is visualized in the mylohyoid muscle defect with the continuous glandular tissue passing from the sublingual space to the submandibular space on CT and MRI, especially coronal images. 2 In CT study, 3 the incidence of the mylohyoid muscle defect was 77% (bilateral in 67% and unilateral in 33%), and SLG herniation was identified in 37% of 100 patients. Of 37 patients with SLG herniation, there were bilateral in 17 (46%), right side in 12 (32%), and left side in 8 (22%). 3 Several studies showed SLG herniation was found in the anterior two-thirds of the mylohyoid muscle. 3 Furthermore, SLG herniation was seen in 73% of 41 patients with plunging ranula. 4 In the present case, SLG herniation with a cystic component (intraglandular mucous retention cyst) was seen in the anterior one-third of the right mylohyoid muscle.
The differential diagnosis of the submandibular lesion with cystic component includes plunging ranula, branchial cyst, dermoid cyst, lymphatic malformation, thymic cyst, lymphadenitis, lymph node tuberculosis, and lymph node metastasis. 5 Although SLG herniation which is a pseudo lesion is not commonly included in the differential diagnosis of the submandibular lesion, recognition of mylohyoid muscle defect and the typical radiologic appearance of SLG herniation can allow differentiation from other pathologic lesions and prevent unnecessary surgery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.