
Abstract
Objective:
The purpose of this study is to review the differences between continuous wave (CW) and UltraPulse (UP) on thermal damage of the laser with different power.
Methods:
Four adult beagle dogs underwent transoral laser microsurgery (TLM) using CO2 laser. The laser emission mode and power was CW (3 W, 5 W, and 8 W) and UP (3 W and 5 W), respectively. The tissue from 4 animals was evaluated histologically on postoperative days 1 and 3. The thermal damage of the laser was measured using slide scan system via SlideViewer version 1.5.5.2 software.
Results:
All dogs underwent TLM uneventfully. Under microscope examined, the laser damage area was composed of 2 parts: the vaporized zone (VPZ) and thermal damage area. The thermal damage area can be divided into thermal coagulative necrosis area (TCN) and hydropic degeneration area. The width of VPZ and TCN in UP mode was less than that in CW mode (P < .01). The data indicate that lower laser power created less thermal damage (P < .01). In addition, the width of VPZ on postoperative day 3 was less than that on postoperative day 1 (P < .01).
Conclusion:
CO2 laser with UP and lower power could decrease the laser thermal damage and may offer more prompt wound healing.
Introduction
Since 1972 when Strong and Jako 1 first applied transoral laser microsurgery (TLM) in the treatment of early laryngeal cancer, the TLM surgical technique has gradually developed. Today, TLM is used in the treatment of not only early laryngeal cancer but also laryngeal benign lesions such as polyps, cysts, Reinke space edema, as well as potentially malignant disorders such as leukoplakias. 2
CO2 laser with a wavelength of 10.6 µm is absorbed by the water of the tissue. The energy of CO2 laser could vaporize the water and result in the ablation of tissue. In addition, residual laser energy is absorbed by the surrounding tissue, causing thermal damage zone. The lateral thermal damage delays the activation of inflammatory cells and prolongs wound healing.3-6 Therefore, the researchers improved the CO2 laser emission mode in order to reduce thermal damage. Studies demonstrated that pulsed-laser beam could reduce the thermal damage zone compared to the traditional continuous wave (CW) mode.7-11
With the gradual advancement of CO2 laser technique, UltraPulse (UP)-mode CO2 laser developed and is widely applied in different departments.12-15 UltraPulse is a pulse wave with a high peak power delivered in millisecond pulses or less and is considered to reduce thermal damage. Although research 15 is done on the differences in phonosurgery between UP and SuperPulse, none of the studies compare UP with traditional CW mode on vocal fold. The objective of this study is to specifically review the differences between CW and UP on thermal damage of canine vocal fold with different power.
Materials and Methods
CO2 Laser
The CO2 laser used in this study is the DEKA SmartXide2 C60. For the purpose of this study, the laser emission mode and power was CW (3 W, 5 W, and 8 W) and UP (3 W and 5 W), respectively. During the experiment, the following settings were included: (1) Laser spot size diameter was 0.143 mm; (2) the laser acting time was 0.4 seconds; and (3) the laser exposure mode is single. These settings were used with both laser emission modes.
Animal Vocal Fold Studies
Four adult beagle dogs weighing 10 to 15 kg were used in our experiment. Four dogs fasted for 8 hours before anesthesia. The dogs were anesthetized with intravenous injection of 3% pentobarbital sodium (1 mL/kg) and supplemented as needed during the operation. After anesthesia, each dog was supine on the operating table, and mandible was restricted with rope.
The operation was performed under surgery microscope (MOELLER Hi-R1000) coupled with the CO2 laser. Suspension laryngoscopy was used to expose the vocal fold of dogs. Both vocal folds were carefully examined to ensure the absence of disorders. The secretion on the vocal fold was removed by the suction device to avoid interference with the CO2 laser effect.
Two laser ablation points were made, one on each side of the vocal fold, using each of different CO2 laser emission mode and power: CW (3 W, 5 W, 8 W) and UP (3 W, 5 W; Figure 1A). Thus, each animal had 5 laser ablation points on each side of the vocal fold, with a total of 10 laser ablation points per animal.
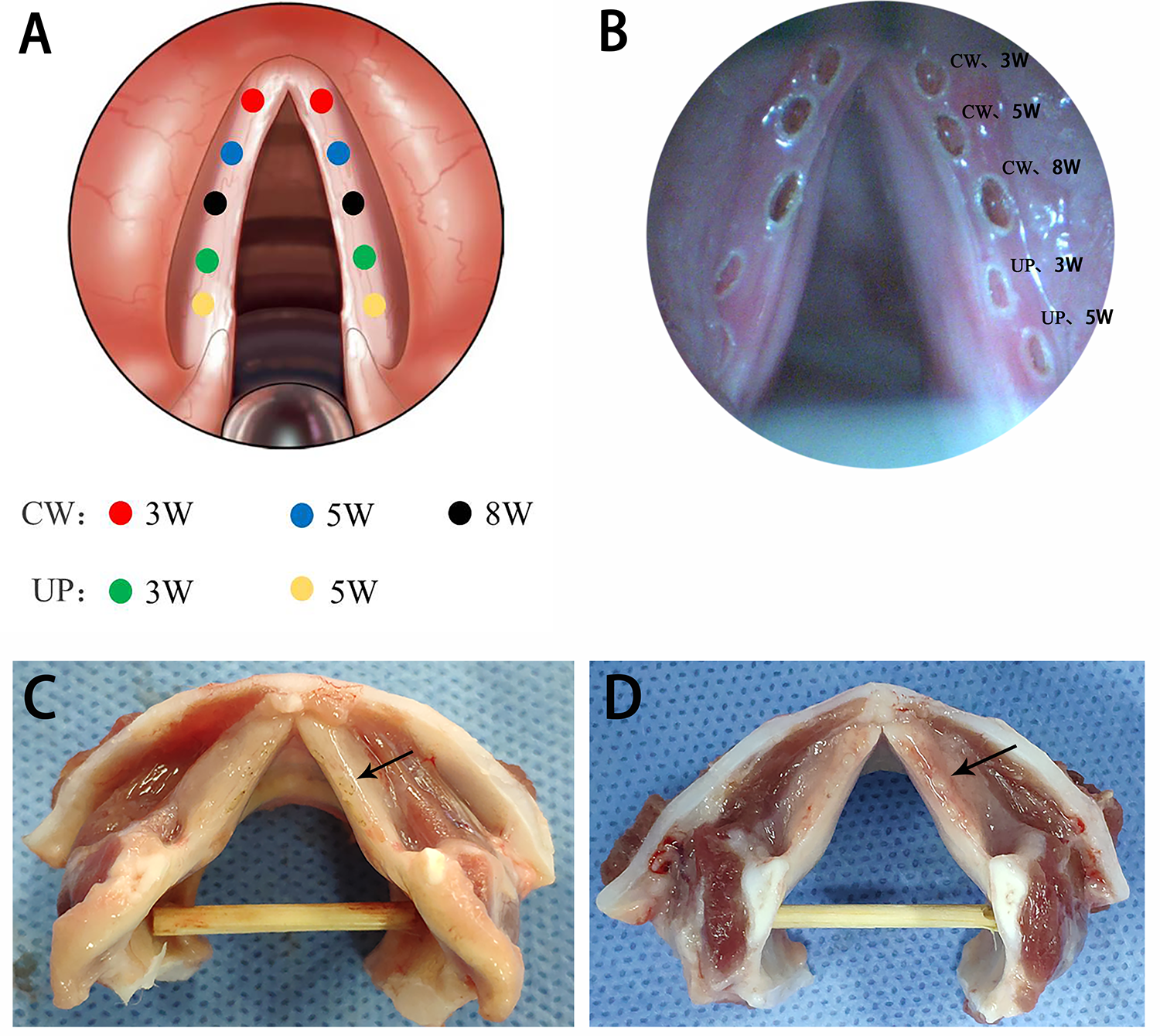
A, Laser ablation points distribution on vocal folds. B, Laser ablation points during the operation. C, D, Laryngeal specimens on days 1 and 3. Black arrow indicates laser ablation points.
The animals were housed individually and allowed access to water and regular dog chow until their respective sacrifice dates. Each animal was sacrificed with potassium chloride intravenously on postoperative days 1 and 3. The larynx of the animals was harvested. Each laser ablation point was divided along the coronal position of the vocal fold. The laser ablation point was preserved in 10% neutral-buffered formalin for 24 hours, embedded in paraffin, and sectioned perpendicular to the middle of laser ablation point with 6 consecutive slices (3-µm thick). The slices were stained with hematoxylin and eosin. The slides were examined under Leica DM1000 LED microscope. The thermal injury range was measured using slide scan system KF-PRO-120 via SlideViewer version 1.5.5.2 software.
Statistical Analysis
Data analyses were performed using the SPSS Statistics 20.0 software package. First, normality test (Shapiro-Wilk test) and homogeneity test (Levene test) were performed. If the data conform to the normal distribution and homogeneity of variance, t test or 1-way analysis of variance was used to compare the thermal damage of canine vocal fold by CO2 laser under different laser emission modes and power. Otherwise, Wilcoxon test or Kruskal-Wallis test was used.
Results
All animals underwent TLM uneventfully, and none died during the operation and postoperative period. In addition, no complications occurred.
During the operation, the vocal fold mucosa was directly vaporized by CO2 laser, and the vaporized zone (VPZ) was carbonized (Figure 1B). There was a white circle around the VPZ. In addition, the carbonization in CW mode was more obvious than that in UP mode. Granulation-like tissue was observed in the laser damage area of the larynx on postoperative day 3 (Figure 1C and D).
Histologic Morphology
Microscopic examination of the laser ablation points on day 1 revealed that the laser damage area was composed of 2 parts: VPZ and thermal damage area. The thermal damage area can be further divided into thermal coagulative necrosis area (TCN) and hydropic degeneration area (Figure 2). On day 3, fibrinous exudation was observed, especially in VPZ. Moreover, fibrinous exudation was more obvious in CW mode than that in UP mode. In addition, the TCN area almost disappeared. The laser ablation points’ representative photomicrographs at different time points are shown in Figure 3.
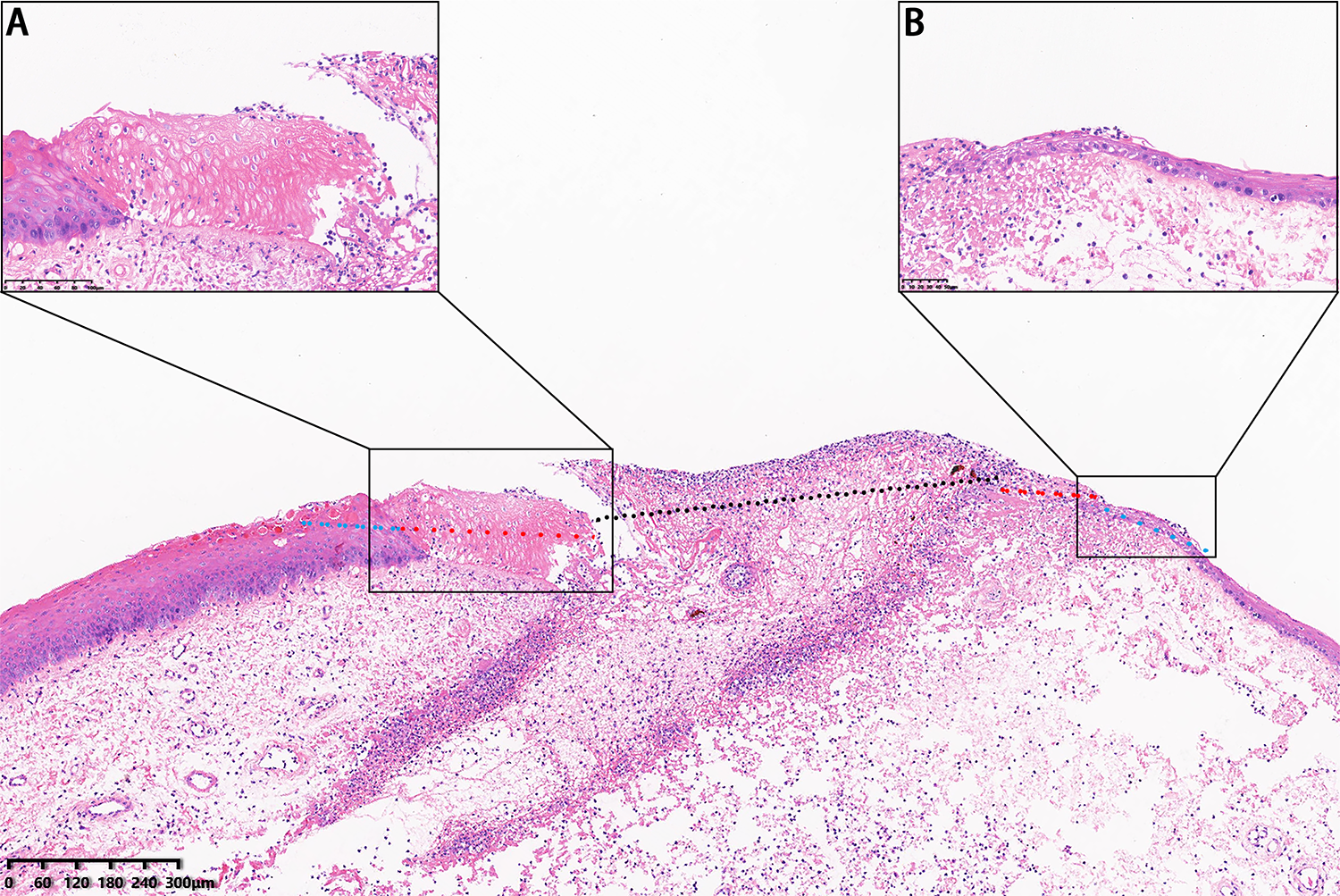
Histopathology examination of continuous wave mode and 8 W on day 1 (hematoxylin and eosin [HE], ×6): (A) Coagulative necrosis area (HE, ×30), and (B) hydropic degeneration area (HE, ×30). Black dotted line indicates vaporized zone; red dotted line: coagulative necrosis area; and blue dotted line: hydropic degeneration area.
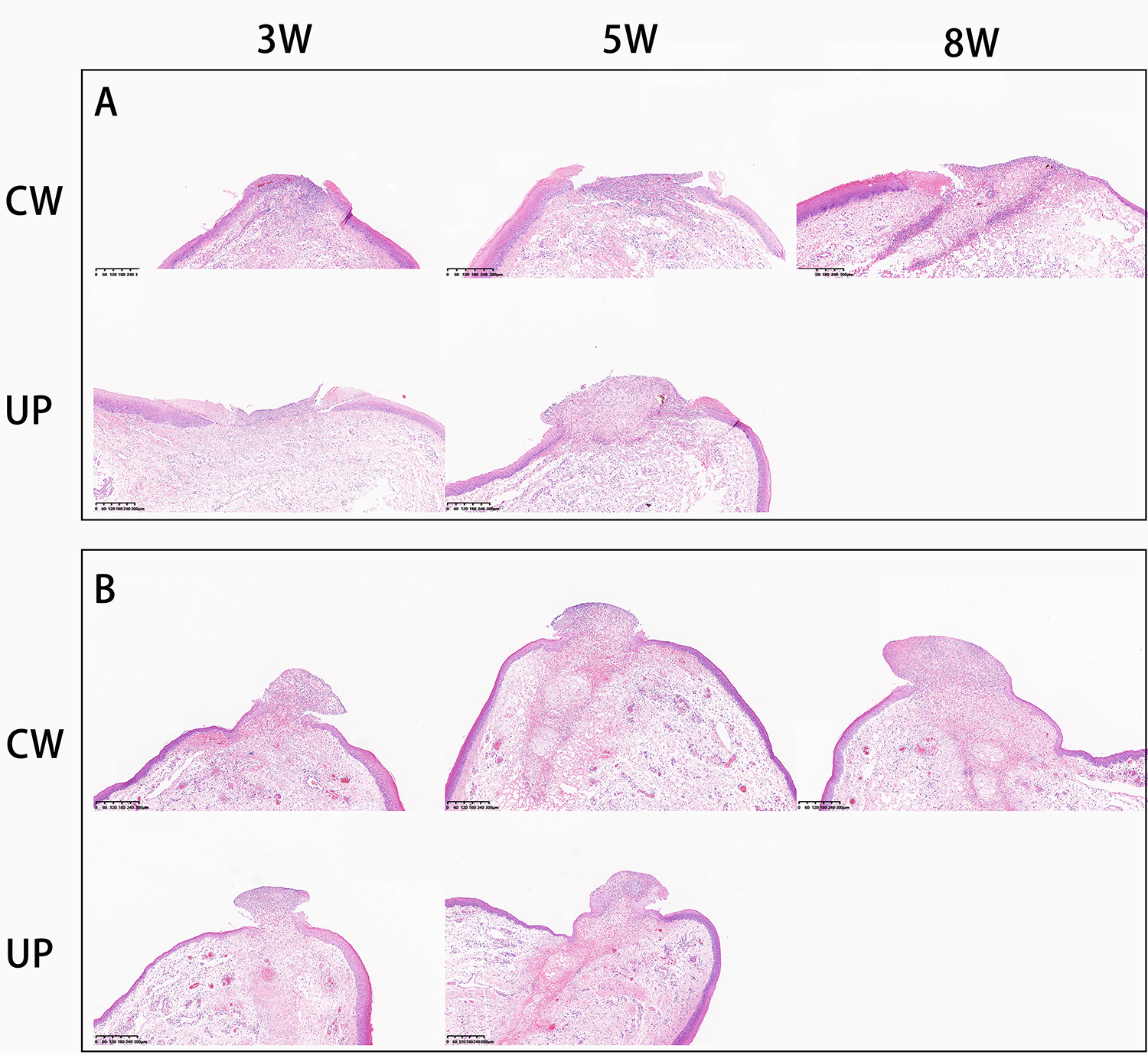
Histopathology examination of each laser emission mode and power (hematoxylin and eosin, ×6): (A) Day 1 and (B) day 3.
Laser Thermal Damage
The width of VPZ was measured on postoperative days 1 and 3. Because TCN almost disappeared on day 3, the width of TCN was measured only on postoperative day 1. The mean values for the width of VPZ and TCN are provided in Table 1. There was less width of VPZ under UP as compared with CW on days 1 and 3, and width of TCN under UP was less than that in CW on day 1 (P < .01; Figure 4A-C). The data indicate that lower laser power created less thermal damage (P < .01; Figure 4D-F). In addition, the width of VPZ on postoperative day 3 was less than that on postoperative day 1 (P < .01; Figure 5).
Width of VPZ and TCN.a
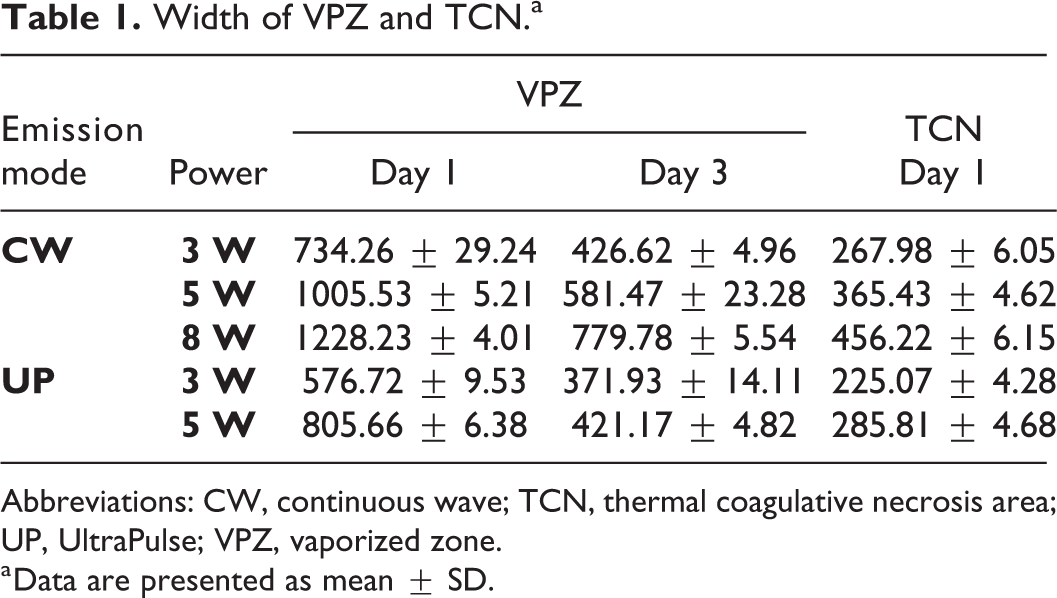
Abbreviations: CW, continuous wave; TCN, thermal coagulative necrosis area; UP, UltraPulse; VPZ, vaporized zone.
a Data are presented as mean ± SD.
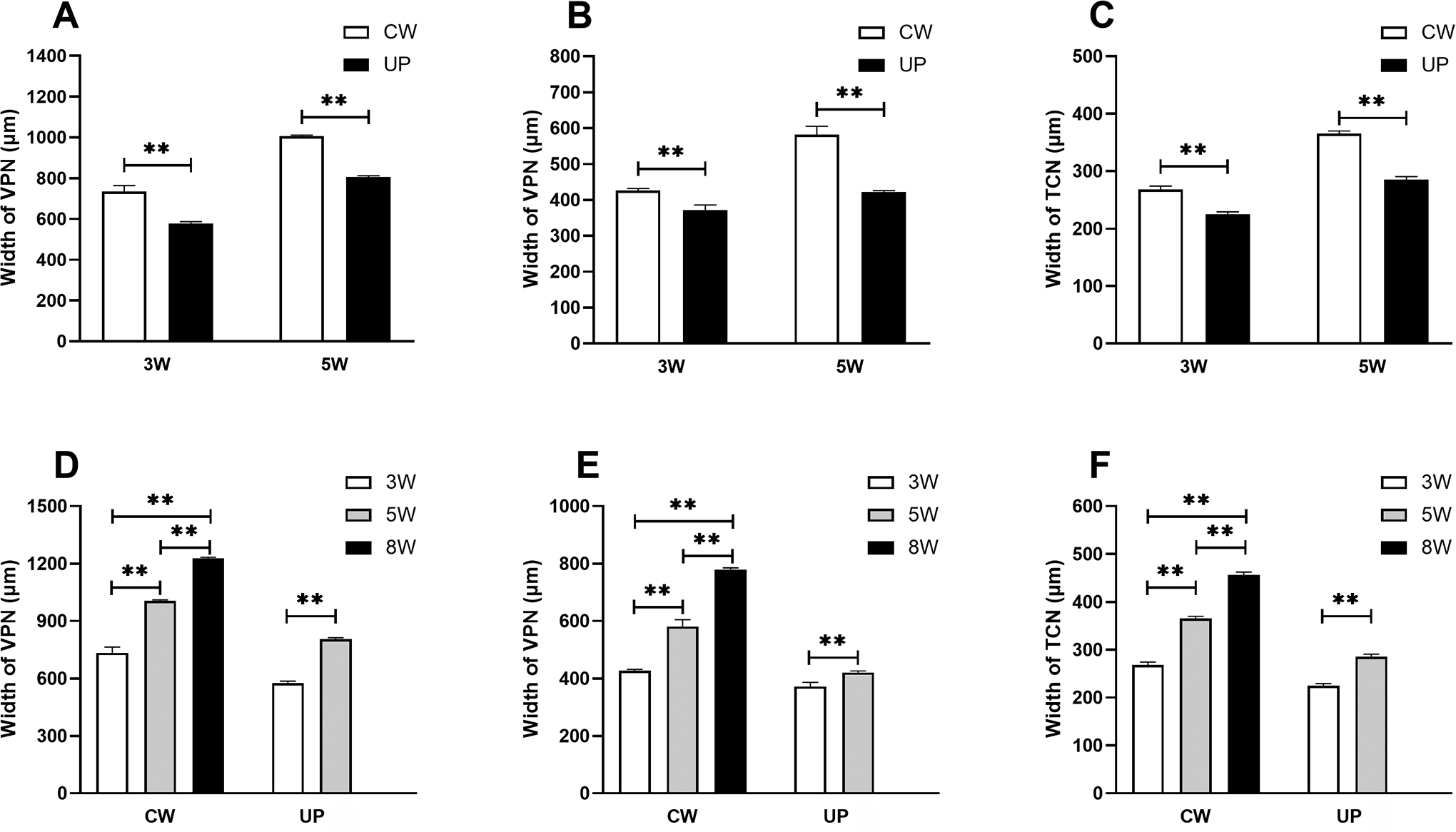
A, Width of VPZ with different power on day 1. B, Width of VPZ with different power on day 3. C, Width of TCN with different emission mode on day 1. D, Width of VPZ with different power on day 1 . E, Width of VPZ with different power on day 3. F, Width of TCN with different power on day 1. **P < .01. TCN indicates thermal coagulative necrosis area; VPZ, vaporized zone.
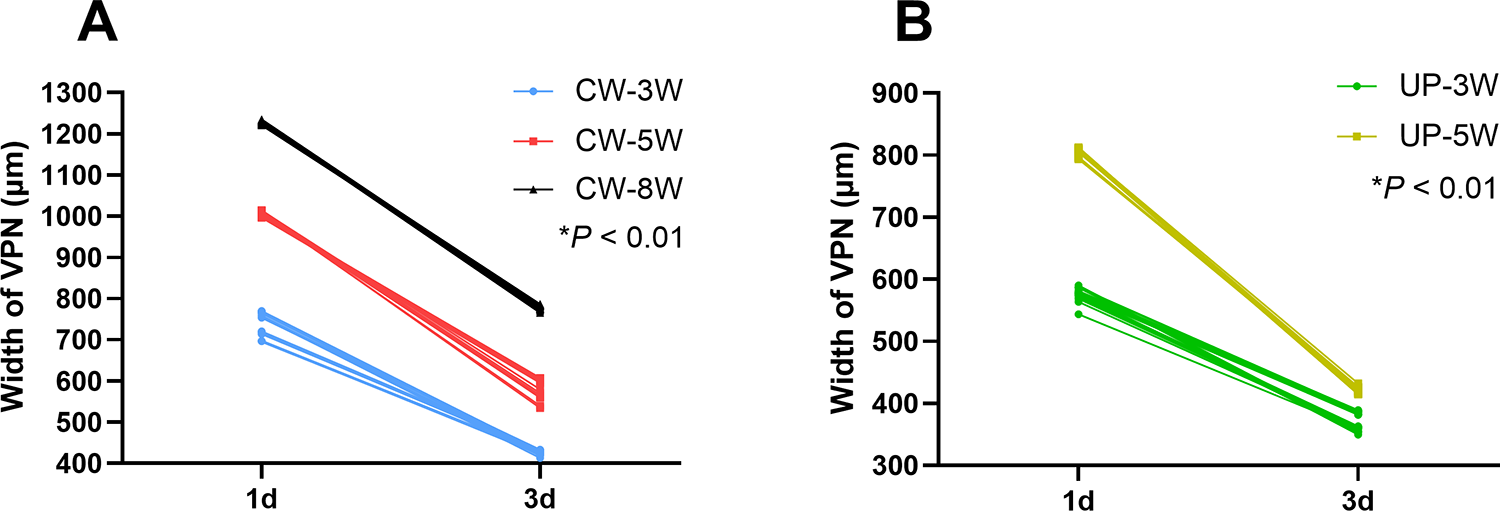
A, Width of vaporized zone (VPZ) on days 1 and 3 with continuous wave. B, Width of VPZ on days 1 and 3 with UltraPulse.
Discussion
Vocal folds are extremely important for vocalization. Vocal fold is a delicate and complex tissue consisting of 2 parts: the cover layer (epithelium and superficial layer of the lamina propria, also known as Reinke space) and the body layer (intermediate and deep layers of the lamina propria and thyroarytenoid muscle). 16 Voice quality depends on the integrity of vocal folds’ structure and the mucous wave vibration. It is very important for the treatment of benign vocal fold lesions by laser to reduce laser thermal damage. Several studies have shown that lateral thermal injury of laser has a negative influence on wound healing. 3 During the development of laser technique, researchers have made great effort to constantly improve the laser technique to reduce later thermal injury, including smaller spot size of the focused laser beam and computer control of the laser beam.17,18
Walsh and Fortune7,10 have demonstrated that using pulsed laser can create less lateral thermal damage compared to the traditional CW laser emission mode. Although these researches were not directly conducted on the vocal fold, it was found that pulsed laser may reduce tissue damage during laryngeal surgery. This study demonstrated that UP laser emission mode created less lateral thermal damage than CW laser emission mode, and lower laser power created less thermal damage. Therefore, UP mode and lower power help reduce thermal damage, thus promoting wound healing and voice recovery.
Early glottic cancer (squamous cell carcinoma, Tis-T2N0), a highly treatable disease, can be treated with surgery or radiotherapy. 19 The surgeries include open partial surgery and TLM. Some researchers concluded that no one treatment is more effective than the other.20-22 Today, TLM represents one of the main options in larynx preservation protocols. Advantages of TLM are shorter hospitalization, lower morbidity, and superior functional outcomes compared to open partial surgery and shorter treatment time and less damage to healthy tissue compared to radiotherapy. 23 Positive resection margin has been identified as prognostic for poorer outcome. 24 Resection margin has not been clearly identified, and 1 to 2 mm is considered an adequate margin by most researchers.25-27
During the research, we found that the laser damage area was composed of VPZ, TCN, and hydropic degeneration area. It inspired us that the actual resection margin consists of resection margin (1-2 mm) and half of VPZ and TCN. For example, VPZ and TCN created by CO2 laser with CW mode and 8 W were 1.22 and 0.46 mm, respectively. During TLM for early glottic cancer, if 2 mm is selected as resection margin, CO2 laser emission mode as CW, and power as 8 W, the actual resection margin is 2.84 mm. The study also showed that the width of VPZ on postoperative day 3 was less than that on postoperative day 1 (P < .05). This means that epithelial cells may begin to migrate to the VPZ and the wound begins to heal on day 3, which was consistent with other study. 10
Many types of animal models have been used to study the larynx or vocal fold, such as mouse, rat, rabbit, pig, and canine. The type of animal model used depends on the nature of the experiment and outcomes of interest. 28 In our study, the canines were chosen as experimental animals due to the size of the lamina propria, ability to phonate, and the amount of tissue it provides. 29 Thus, our experimental results can provide certain reference for clinical practice.
The results of this study have several important implications for TLM in vocal fold diseases: (1) CO2 laser with UP emission mode and 3 W (or lower) created less lateral thermal injury and can be used in benign lesions. (2) In TLM for early glottic cancer, CO2 laser with CW emission mode and 8 W (or higher) can be used to expand resection margin in order to ensure negative margins. There is a limitation to this study that only data from postoperative days 1 to 3 were studied. Therefore, whether CO2 laser with UP mode and lower power could prompt wound healing is unknown.
Conclusion
To our knowledge, our study appears to be the first research to review the thermal damage of vocal fold by CO2 laser under different laser emission modes (CW vs UP). According to the results, the laser damage area was composed of VPZ, TCN, and hydropic degeneration area. In addition, CO2 laser with UP emission mode and lower power created less lateral thermal injury than CW mode and higher power. Further studies are necessary to investigate whether CO2 laser with UP mode and lower power could prompt wound healing.
Footnotes
Authors’ Note
Xumao Li and Jiaying Li contributed equally to this study.
Acknowledgments
The authors thank Ms Leichen Li, an anesthetist, for her help.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.