
Abstract
Cochlear implants improve the quality of life of patients with bilateral severe sensorineural hearing loss. Normally, patients with cochlear implants can continue to use the devices for years without any complications. However, equipment failure or infection at the implant site could develop in some patients, and this might often necessitate implant replacement. Although cochlear implant replacement surgery itself is not a major risk in most cases, extensive tissue resection will be required in cases involving infection, and the insertion site of the temporal bone implant will need to be changed. We encountered a case of skin necrosis at the temporal bone implant site caused by constant external irritation from the temple of an eyeglass frame. The patient underwent cochlear implant replacement surgery involving full-thickness skin grafting from the abdomen. Thereafter, the patient’s condition improved. Full-thickness skin grafting can be useful in cases of extensive skin defects encountered during cochlear implant replacement.
Introduction
Cochlear implants are a standard of care for patients with bilateral severe sensorineural hearing loss which help improve their quality of life. Generally, the device does not require replacement once it is inserted, but in some cases, such as when it is implanted in a child, it may need to be replaced after the child reaches adulthood. Other factors leading to the replacement of a cochlear implant include failure of the hard device, failure of the soft device, and trauma.
We encountered a rare case of a 66-year-old man who required cochlear implant replacement because of exposure of the temporal bone implant resulting from skin necrosis associated with persistent external irritation. We report this case and present a literature review to highlight the favorable outcomes of electrode replacement and skin grafting from the abdomen.
Case Report
A 66-year-old man underwent right cochlear implant surgery in 2005 for post-lingual deafness due to bilateral sudden sensorineural hearing loss. He was referred to our department in May 2018 for cochlear implant rehabilitation. Since then, he has been undergoing rehabilitation at our outpatient clinic. However, around March 2020, he developed skin redness in the area where the temporal bone implant was inserted. Owing to persistent pressure applied by the temple of his eyeglasses, he developed cellulitis, and the cochlear implant was partially exposed (Figure 1A). Pus deposits were found on the skin around the implant, and methicillin-resistant Staphylococcus aureus was detected in the pus. The free-field pure-tone threshold was 43 dB by average hearing level (5 frequencies: 250, 500, 1000, 2000, and 4000). Preoperative middle ear X-ray showed no deviation in the cochlear electrodes and no obvious soft shadows in the middle ear (Figure 1B). Mupirocin calcium hydrate ointment was applied, and a cushion was placed between the eyeglass temple and the area of irritation, but his condition did not improve.
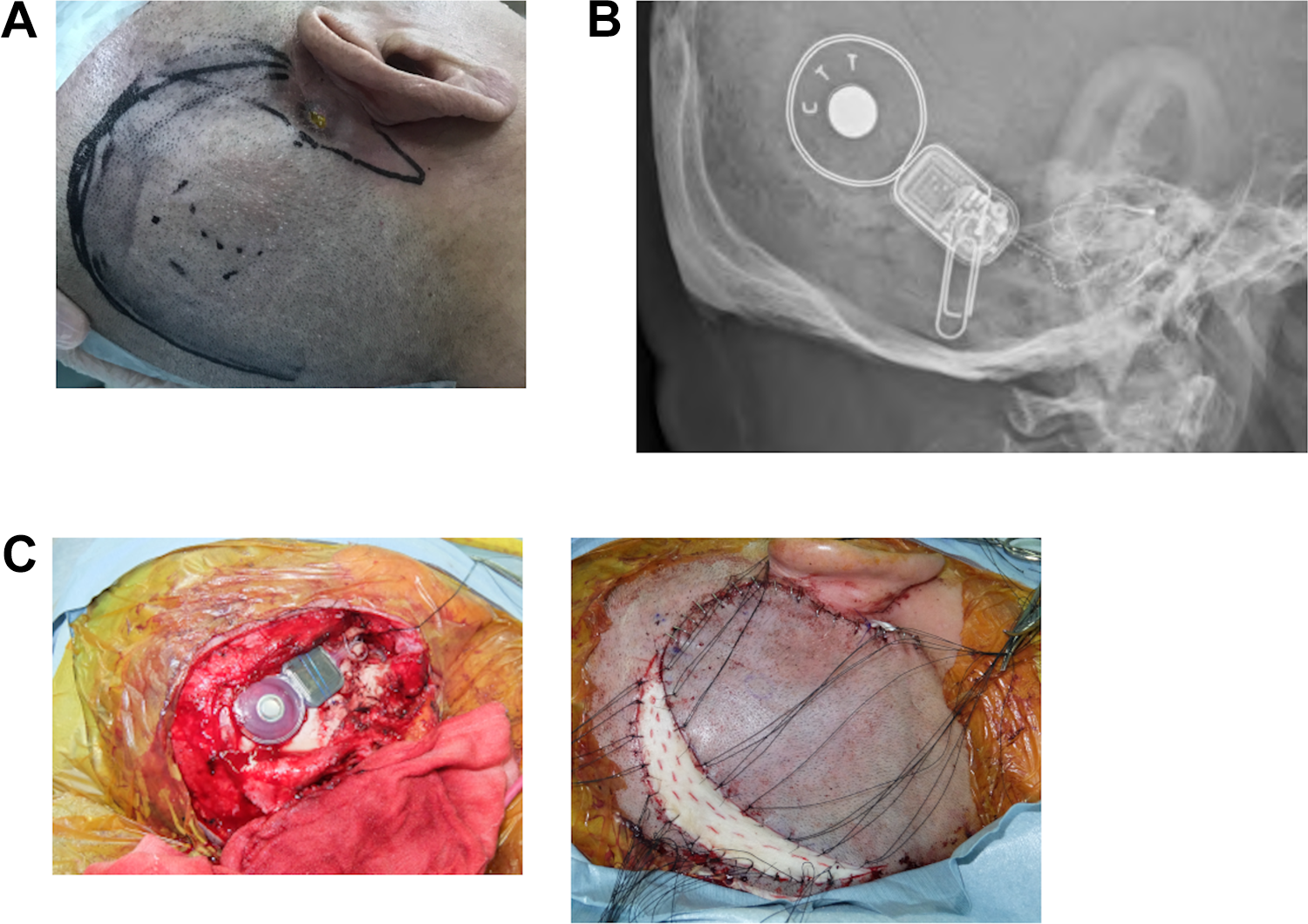
A, Preoperative local findings. A partially exposed cochlear implant in the temporal bone showing skin infection. The surrounding area is contaminated with pus. B, Preoperative middle ear X-ray imaging. Cochlear electrodes are inserted into the cochlea, and there is no deviation. C, Surgical findings. U-shaped incision at a distance of 3 cm from the temporal bone implant was made. Osteotomy was performed and a new implant was installed. A full-thickness skin graft was transplanted to the site of the defect.
Therefore, we decided to perform cochlear implant replacement. An inverted U-shaped incision at a distance of 3 cm from the temporal bone implant was made to elevate the skin valve. The cochlear electrodes were then severed, and the temporal bone implants, including the surrounding infected granulation, were excised. While performing mastoidectomy, the severed electrodes were traced and cut again at the site of the posterior thoracic opening. After excising the electrodes, a new electrode was inserted. Osteotomy was performed posteriorly and superiorly to the site where the last implant was placed, and a new implant was installed. A full-thickness skin graft was transplanted from the abdomen to the site of the defect (Figure 1C). Postoperative middle ear X-ray showed no deviation in the cochlear electrodes (Figure 2A). At 3 month after the surgery, the grafted skin had positively attached, and the hearing threshold levels showed no abnormalities (Figure 2B). The free-field pure-tone threshold was 30 dB by average hearing level (5 frequencies: 250, 500, 1000, 2000, and 4000).
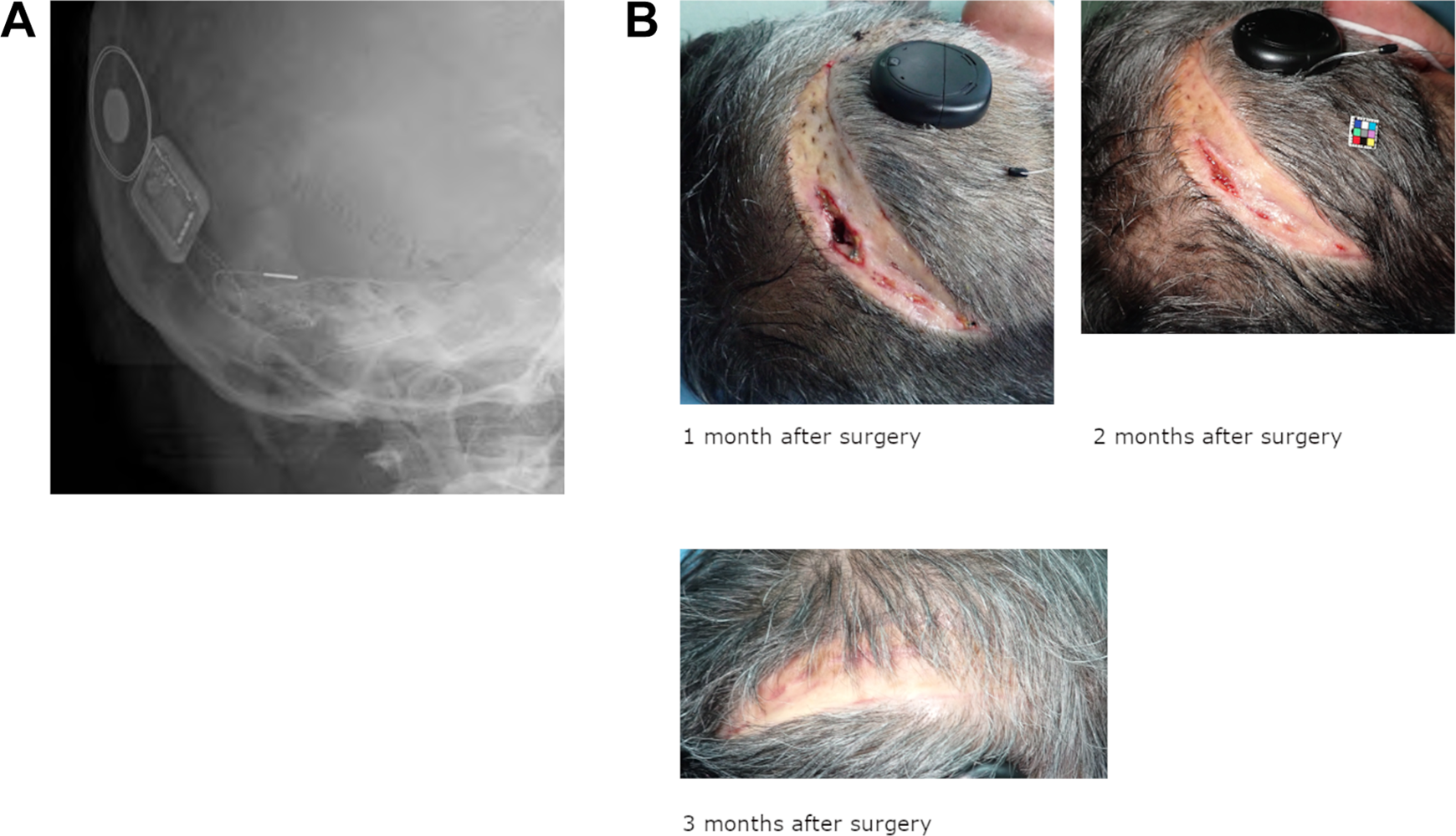
A, After cochlear implantation. The electrodes are inserted into the cochlea, and no abnormalities are observed. B, Postoperative local findings. Skin grafts are engorged and show no signs of infection.
Discussion
Cochlear implants are very useful for improving the quality of life of patients with bilateral severe sensorineural hearing loss. Although these implants generally last a lifetime, they sometimes need to be replaced when they become defective or outdated.1-4 In the present case, the cochlear implant had to be replaced because the continuous irritation caused by the eyeglass temple resulted in skin necrosis and infection at the temporal bone implant site. Previous reports suggested that the probability of cochlear implant site infections was 1.7% to 3.3%, and Staphylococcus aureus was the most commonly reported causative organism.5-10 Methicillin-resistant Staphylococcus aureus was also detected in the present case.
In contrast to cases of replacement due to equipment failure, cases of cochlear implant replacement surgery owing to infection often require the removal of the infected skin. Although the wound could be closed with normal skin sutures if the resection area was small, the skin defect in the present case was so extensive that skin graft implantation had to be performed. In this case, full-thickness skin grafting was implemented. The literature shows that a split-thickness skin graft is also effective as a treatment. 11
The risk of hearing level reduction associated with replacement surgery is considered low. Indeed, no significant changes were detected in the free-field pure-tone threshold test before and after the present surgery. However, because the device was replaced with a new one, the patient was expected to take time to adapt to the new device.
In conclusion, we encountered a case in which continuous external irritation caused an infection at the implant site that necessitated cochlear implant reimplantation. If extensive skin loss is identified during debridement of an infected wound, cochlear implantation with full-thickness skin replacement is a useful treatment option.
Footnotes
Authors’ Note
Written informed consent was obtained from the patient for using the data in this study. Our institution does not require ethical approval for reporting individual cases or case series.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.