
Abstract

Significance Statement
Temporal bone fractures are a common clinical entity in a busy accident and emergency department. They account for about 18% of all skull fractures and most probably their management demands multidisciplinary treatment. We are aiming to present a vestibular fracture with a deceiving presentation, the diagnostic pathway we followed and the management plan that the patient was offered.
Case Presentation
A 65-year-old male patient was referred to our ear, nose, and throat (ENT) department after sustaining a mechanical fall from 1.5 m height. The result was a head injury on the right side, over the temporal area. Initially, the patient was investigated for brain injury, and underwent an urgent brain computed tomography (CT) that revealed frontal lobe contusions and subdural hematoma. On examination, he complained about hearing loss and tinnitus in the right ear, continuous rotatory vertigo, severe nausea and vomiting, and instability while walking. Otoscopy did not reveal any pathology, the patient had second-degree spontaneous horizontal nystagmus with the fast phase pointing toward the left side. Free field testing revealed right-sided deafness, Weber lateralized to the left ear while Rinne was positive on both sides. Unterberger test was positive, with the patient turning toward the right side. Head thrust test was positive on the right side. Pneumatic otoscopy did not reveal nystagmus. The rest of the clinical examination was unremarkable. Clinical tests were followed by pure tone audiometry (Figure 1) and CT scan of the temporal bones (Figure 2). Pure tone audiometry showed total deafness on the right and high-frequency hearing loss on the left. The CT scan depicted a transverse, otic capsule violating temporal bone fracture on the right side.
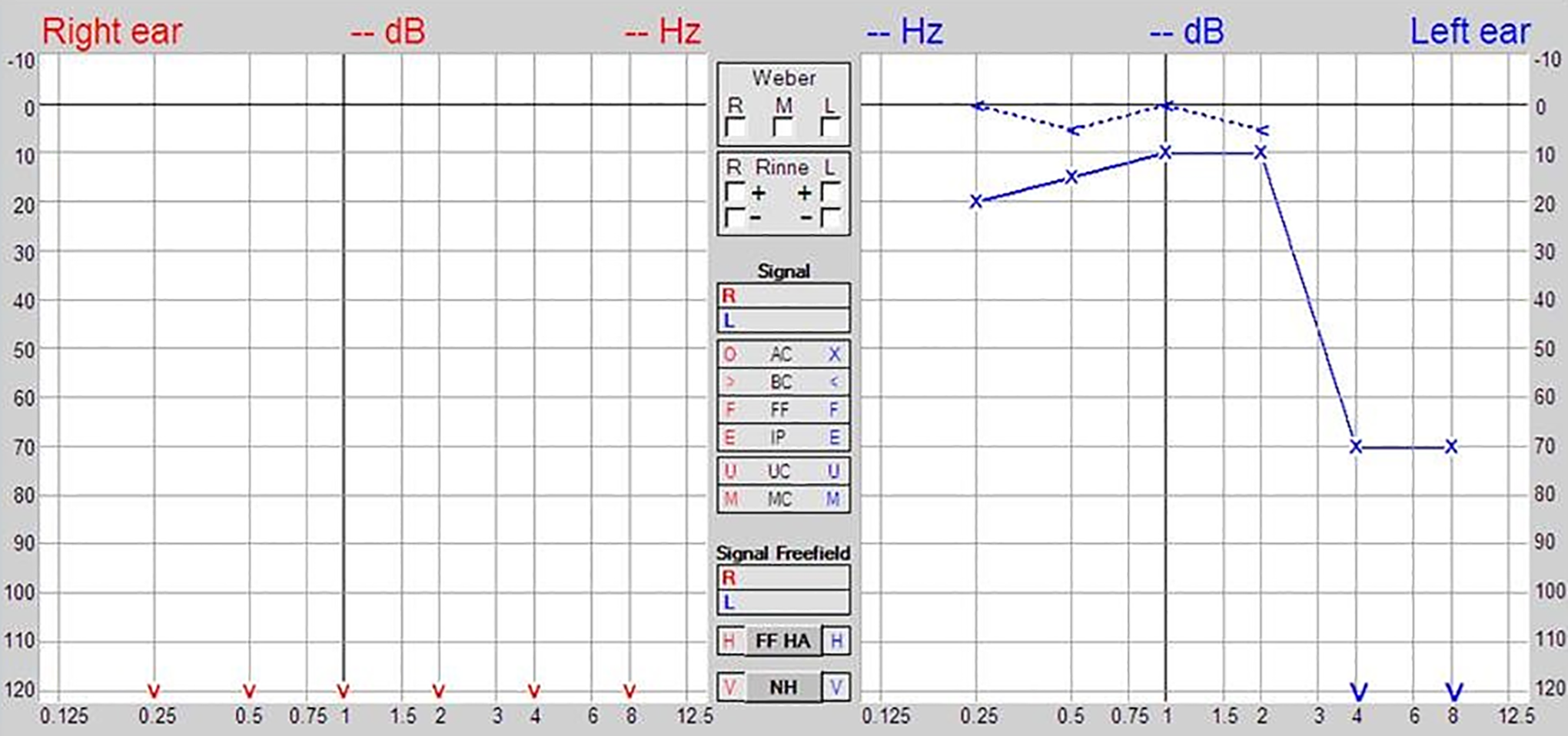
Pure tone audiogram, depicting total deafness on the affected side.

Transverse, otic capsule violating fracture of the right temporal bone.
He was initially treated with a 10-day course of steroids and a 3-day course of antiemetics (Dimenhydrinate). The symptoms did not completely resolve after one month so he was encouraged to do vestibular rehabilitation exercises and started on Betahistine tablets. Three months after the incident, he appeared clinically improved. There was no spontaneous nystagmus and the head thrust test remained positive for the right labyrinth. Although central compensation has not been achieved yet, it was essential to observe that the patient is back to his normal activities.
Discussion
Around 99% of temporal bone fractures are the consequence of a blunt trauma and 80% of them are combined with an intracranial injury. 1 Vestibular fracture is most commonly a result of a transverse temporal bone fracture. According to the traditional classification, temporal bone fractures are grouped into transverse, longitudinal, or mixed according to their relations to the petrous pyramid. 2 Longitudinal fractures appear more frequently than transverse fractures with an incidence of 70% to 90% and 10% to 30%, respectively.3,4 Signs and symptoms vary and depend on the structures affected by the fracture line. With regard to hearing loss, transverse fractures are mainly associated with sensorineural hearing loss (SNHL), while longitudinal fractures are associated with conductive hearing loss. Sensorineural hearing loss may occur due to membranous labyrinth disruption, cochlear nerve injury, obstructed cochlear blood supply, perilymphatic fistulas, and obstruction of the endolymphatic duct caused by the temporal bone fracture. 2
A more recent classification of temporal bone fractures is based on the integrity of the otic capsule. Thus, fractures are categorized into otic capsule sparing and otic capsule violating fractures. The later run through the labyrinth and cause a series of manifestations such as SNHL, facial nerve injury, or cerebrospinal fluid fistula. This classification is of higher value, as it allows the clinician to stratify the severity and give an idea of the outcomes.1,5
Johnson et al reported that vertigo due to temporal bone trauma is self-limiting, with a duration of 6 to 12 months. 6 There are only a few studies in the literature related to post-traumatic vertigo due to vestibular injury. In our case, in addition to the SNHL, the patient presented with vestibular neuronitis-like symptoms such as spontaneous nystagmus, positive Unterberger test, and nausea/vomiting that could be attributed to the vestibular failure.
A vestibular fracture should be differentiated from acute labyrinthitis, ischemic attack, and perilymph fistula. Complete ENT examination is necessary and will guide the doctor to the required investigations and the right diagnosis. Acute labyrinthitis may have similar symptoms but the CT scan will show no pathological signs. A perilymph fistula would give a positive fistula test during the initial assessment. An ischemic attack can be excluded after careful neurological examination and a CT scan of the brain.
It is of paramount importance to diagnose the extent of the transverse temporal bone fracture complications by paying attention to the structures affected. Early diagnosis and specialist ENT referral for further management, treatment and rehabilitation is necessary. A fracture line running through the vestibule can deceive the clinician doing the initial assessment, who may suspect a brain injury instead of posterior labyrinth fracture. Ear, nose, and throat surgeons and radiologists should be aware of these details when reporting a scan in correlation with the presenting signs and symptoms.
Footnotes
Authors’ Note
The authors declare that written informed consent for patient information and images to be published was provided by the patient.
Marios Stavrakas is also affiliated with 1st Academic Department of Otorhinolaryngology-Head and Neck Surgery, AHEPA Hospital, Aristotle University of Thessaloniki, Greece.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.