
Abstract
Hodgkin lymphoma (HL) is an uncommon B-cell malignant disease. It usually presents with mediastinal and/or laterocervical lymph node localization, while primary extranodal HL is a rare entity giving rise to diagnostic and therapeutic challenges. It rarely presents as just extranodal localization, so its presence within the maxillary sinus without any lymphadenopathy is exceptional. Given the rarity of this localization, there is no standard treatment for maxillary sinus HL. We present a case of a patient with extranodal HL of the right maxillary sinus treated with primary surgery followed by adjuvant sequential chemoradiation therapy.
Introduction
Hodgkin lymphoma (HL) is an uncommon B-cell malignant disease characterized by a bimodal distribution, with an increased incidence in patients in their early 20s and with a similar peak in patients older than 55 years of age. 1 According to the WHO classification, there are 2 main types of HL: the classical subtype (nodular sclerosis, lymphocyte-rich, mixed cellularity, lymphocyte-depleted) and the nodular lymphocyte-predominant subtype. 2
At the time of diagnosis, the most frequent presentation is supradiaphragmatic lymphadenopathy. The most typical localization is as a mediastinal mass that can reach considerable size before becoming symptomatic; it is defined as bulky if larger than 10 cm. 3
Extranodal sites can occasionally be involved by direct invasion or hematogenous spread, commonly to the spleen, liver, lungs, or bone marrow. Primary extranodal HL is a rare entity causing diagnostic and therapeutic challenges. In the literature, there are few reported cases of extranodal HL of the maxillary sinus. We describe a case of a 66-year-old man with primary extranodal HL of the right maxillary sinus, accompanied by a brief review of the literature.
Case Report
A 66-year-old man presented with a 3-month history of nasal obstruction and painless soft tissue swelling of his right cheek, accompanied by typical B symptoms: fever, night sweats, and weight loss (5 kg in the previous 3 months). His comorbidities were hypertension, chronic obstructive pulmonary disease, previous colic perforation, hepatitis B virus (HBV) core positivity, dyslipidemia, and previous anterior ST-elevation myocardial infarction treated 7 months earlier with percutaneous coronary intervention on interventricular anterior coronary and medicated stent.
Physical examination showed an ulceroproliferative lesion in the right hemipalate (Figure 1)

Ulceroproliferative lesion in the right hemipalate.
A transoral biopsy was performed, and the histological examination was consistent with classical HL (Figure 2).
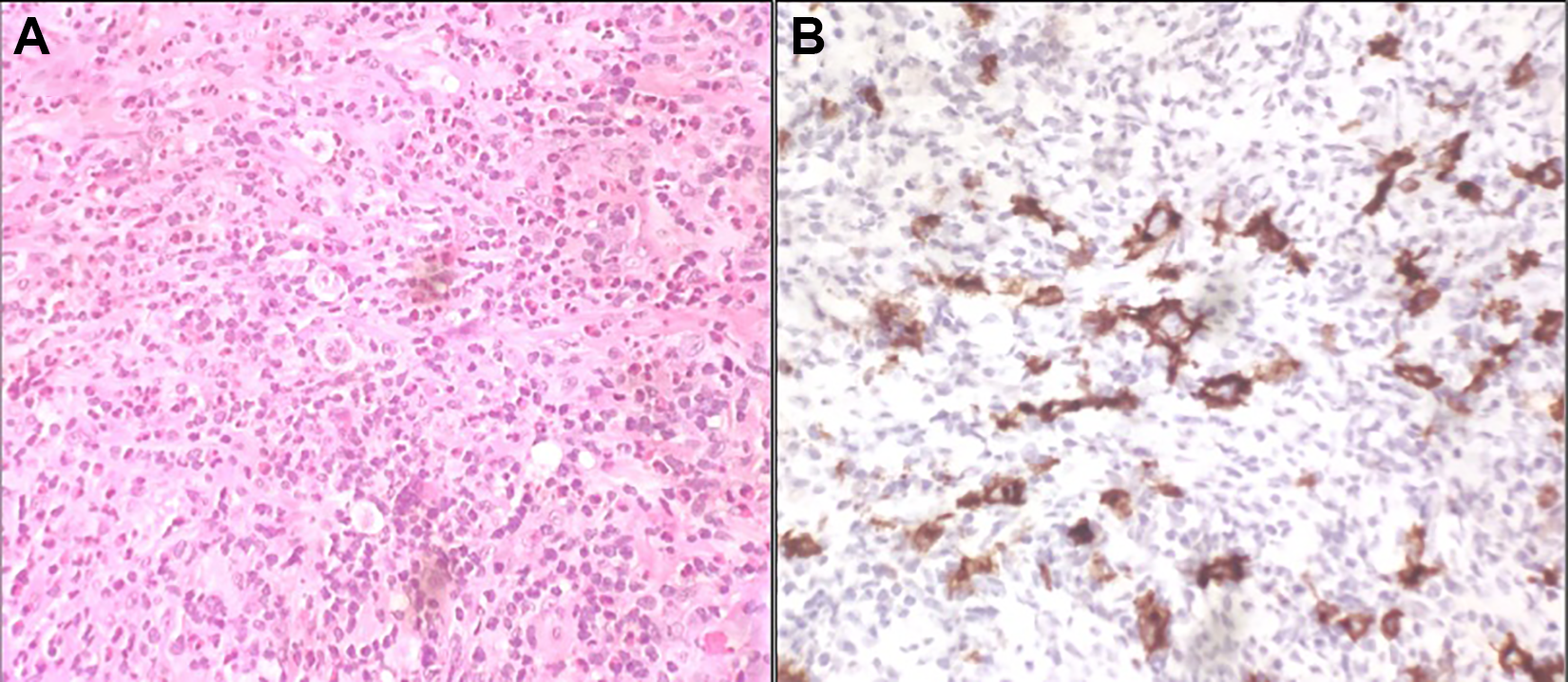
A, Hematoxylin and eosin staining (×40): infiltration by lymphoproliferative disease composed of several neoplastic cells with Reed-Sternberg morphology in an inflammatory background rich in eosinophils. B, CD30 staining: intense cytoplasmic and membrane positivity in large neoplastic cells.
Laboratory workup showed only a slight increase in erythrocyte sedimentation rate (ESR) (44 mm).
Total body computed tomography (CT) with contrast and magnetic resonance imaging (MRI) revealed hypodense material invading a large portion of the maxillary sinuses with bone erosion of the sinus floor (Figure 3)
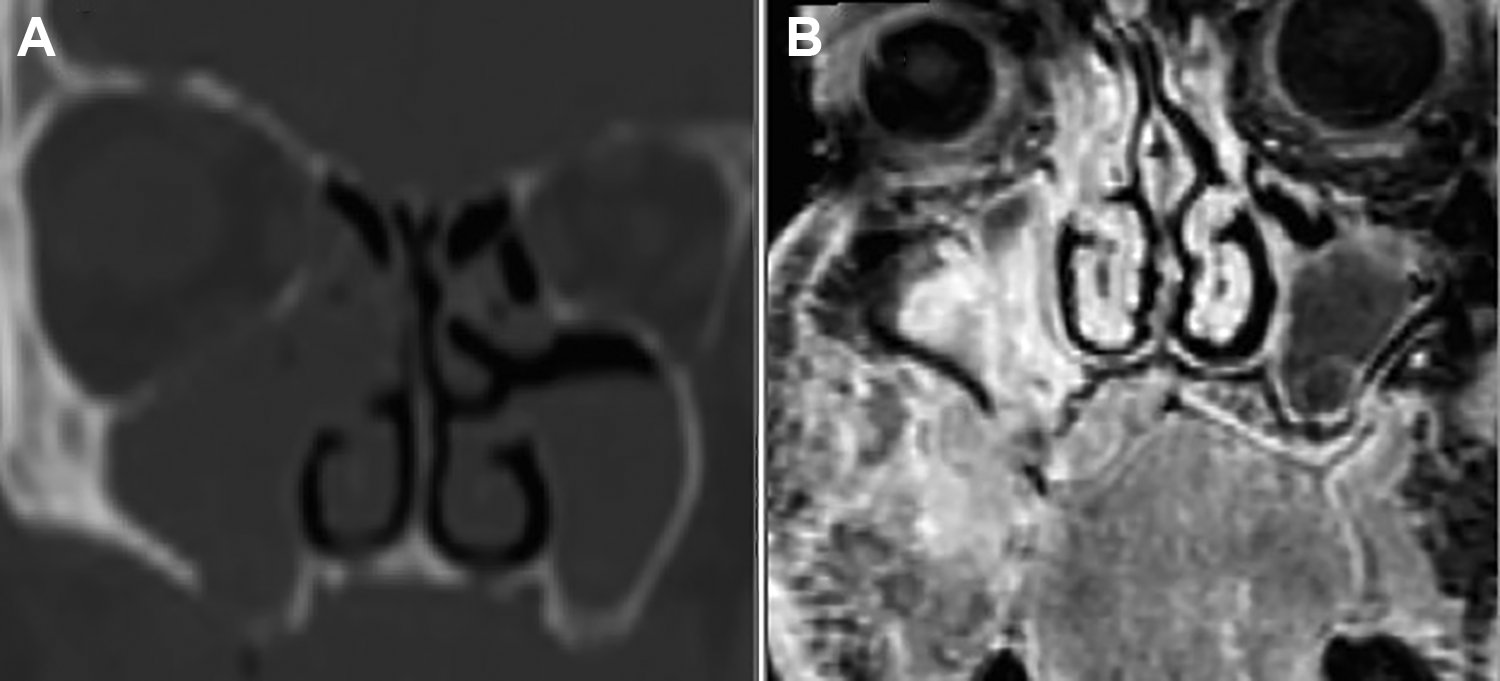
Maxillofacial (A) coronal CT scan with contrast and (B) coronal MRI revealed hypodense material invading a large portion of the right maxillary sinuses and ethmoidal cells with bone erosion of the maxillary sinus floor. MRI also showed irregular tissue at the right hemipalate level, with involvement of ipsilateral buccal mucosa and infiltration of the masticatory space, temporal muscle, buccinator muscle and buccal space. CT indicates computed tomography; MRI, magnetic resonance imaging.
No significant lymphadenopathies were found at either the supradiaphragmatic or subdiaphragmatic level. Positron emission tomography (PET) documented the presence of an area of abnormal hypermetabolism localized in the right portion of the palate, with cranial erosion of the bone and maxillary sinus (SUVmax 11.6). There were no other significant findings. The disease was then staged as IB E. 4
Analyzing the prognostic factors that have been associated with early-stage disease in the literature, 5 it can be seen that our patient presented with increased ESR (44), extranodal involvement, and age over 50 years. 6
He underwent partial resection of the lesion through an endoscopic endonasal approach, and the final pathologic findings confirmed the diagnosis of classical HL, the nodular sclerosis variant.
The patient was referred to the hematology division of our hospital where his therapy was set up according to the chemotherapy scheme MBVD 7 (Myocet (TM) or liposomal doxorubicin 38 mg, bleomycin 15 mg, vinblastine 9 mg, and dacarbazine 550 mg). Supportive care included lamivudine 100 mg daily. After the first cycle, the patient experienced hyperthermia, which was treated with intravenous ceftriaxone for 5 days; the dose of chemotherapy was reduced to liposomal doxorubicin 30 mg, bleomycin 10 mg, vinblastine 8 mg, and dacarbazine 500 mg.
A second MRI demonstrated a marked reduction in neoplastic tissue. A few days before the start of the third cycle, the patient arrived at our emergency department with dyspnea and hyperthermia. Following hospitalization in the emergency medicine department, therapy with levofloxacin and fluconazole was started. Noninvasive mechanical ventilation was necessary because of worsening gas exchange. Due to the isolation of methicillin-sensitive Staphylococcus aureus on bronchoalveolar lavage, continued monotherapy with Linezolid was started. The suspicion of an SARS-CoV-2 infection was ruled out by performing a viral RNA search on a preserved bronchial sample. After 10 days of orotracheal intubation, the patient was extubated and subsequently underwent continuous positive airway pressure cycles alternating with high-flow nasal cannula ventilation.
Positron emission tomography reassessment, performed 3 months after the last administration of chemotherapy, showed complete resolution of the abnormal hypercaptation previously observed corresponding with the right hemipalate. Radiotherapy consolidation treatment was performed on the areas initially affected by the lesion, with a total dose of 30 Gy fractionated in 10 sessions using the volumetric modulated arc therapy–image-guided radiation therapy technique with daily core beam CT. 8 Computed tomography and PET scans indicated complete remission. No HBV reactivation occurred.
The patient was placed in follow-up and after 12 months has no signs of recurrence (Figure 4).

Patient’s right hemipalate 12 months after treatment.
Discussion
Hodgkin lymphoma represents about 4% of all lymphoma cases in the head and neck region, mostly arising at a lymph node. 9 The majority of patients with head and neck involvement present with an indolent cervical lymphadenopathy and about one-third of them also have constitutional symptoms (high fever, drenching night sweats, weight loss, and chronic pruritis). 10
Hodgkin lymphoma cannot be distinguished from non-Hodgkin lymphoma using imaging techniques (ultrasound, CT scan, MRI, and PET). 11 A definitive diagnosis can only be made by biopsy 4 with identification of Reed-Stemberg cells that are usually CD15- and CD30-positive, surrounded by a rich cellular environment of lymphocytes, eosinophils, and histiocytes. 10
Currently, due to advances in radiation therapy and its combination with chemotherapy, most patients newly diagnosed with HL have an excellent prognosis. 4 Hodgkin lymphoma with extranodal involvement occurs rarely, mostly in the lymphatic tissue of Waldeyer’s ring. A recent study on head and neck lymphoma identified just one case of extranodal involvement of the tonsils among 28 patients affected by HL. 12 At the time of writing, there are 7 cases of extranodal HL of the maxillary sinus reported in the literature (Table 1).13-19
Cases describing in literature about extranodal HL of the maxillary sinus.
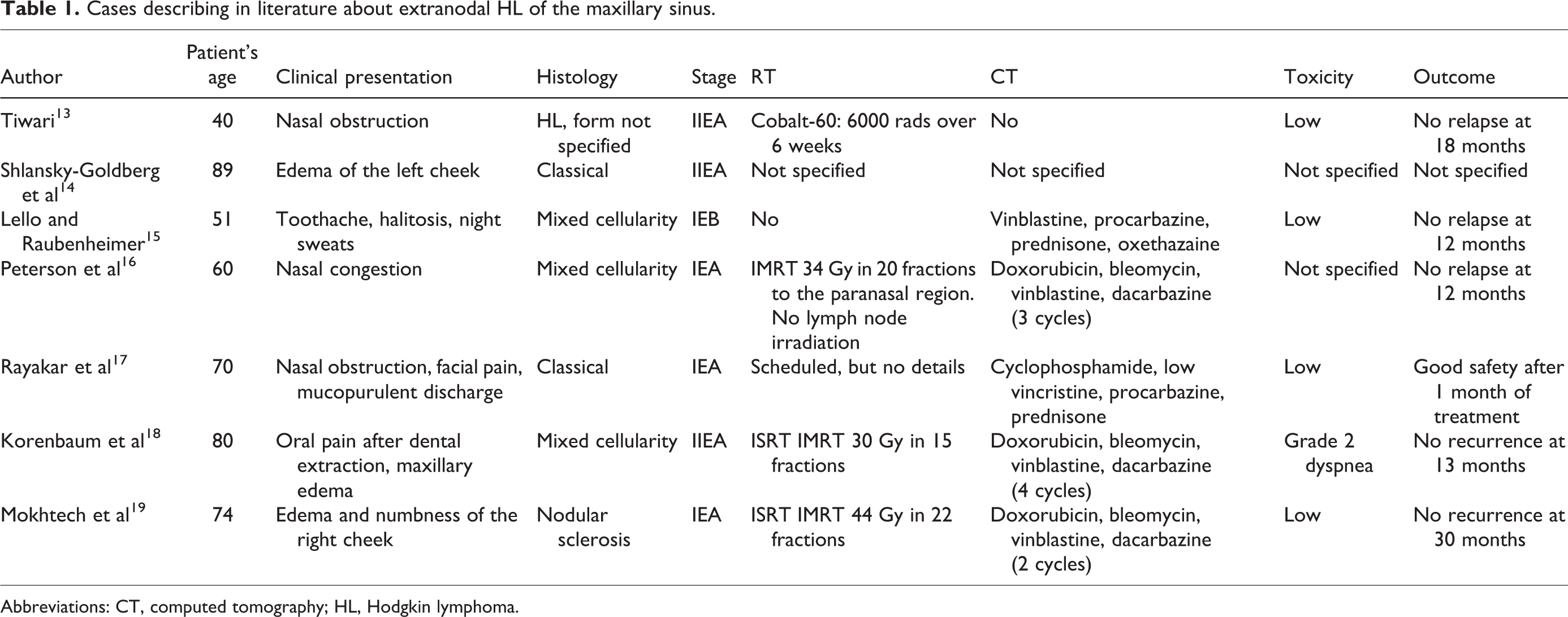
Abbreviations: CT, computed tomography; HL, Hodgkin lymphoma.
Given the rarity of this localization, there is no standard treatment for maxillary sinus HL. The cases reported in the literature are quite varied, but they suggest that this disease has a good therapeutic response and a good prognosis.
Our case confirms that, despite the particular characteristics of the localization, it is possible to successfully treat patients with disease limited to certain anatomic sites. This is by administering chemotherapy regimens followed by radiotherapy consolidation, in accordance with current international indications for HL. However, particular attention must always be paid to the patient’s comorbidities, which in our case contributed to complicate the outcome in the short term. It is therefore always necessary to adapt the therapy to the individual case, carefully choosing the dosage of drugs to maximize the risk/benefit ratio.
In this setting, consolidation radiotherapy proved to be an effective and safe tool to reduce the risk of recurrence in the long term. In addition, lymphoproliferative diseases have a marked tendency to spread systemically, so chemotherapy can rarely be avoided apart from at very early stages. However, in some cases, a surgical and/or endoscopic approach can, by reducing the initial mass, improve the long-term outcome and make both treatment and consolidation radiotherapy even more effective. Further investigation is therefore necessary to accurately identify the best possible treatment options for patients who have extralymphatic disease involvement in very rare sites.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.