
Abstract
COVID-19 also known as severe acute respiratory syndrome coronavirus 2 is the result of a highly transmissible coronavirus which can result in severe infection of the respiratory tract. The global pandemic which began in early 2020 has created a number of challenges for the medical community to contain the rate of transmission, especially to health care workers. A minority of the infected population will progress toward severe respiratory distress ultimately requiring mechanical ventilator assistance. Although preliminary data suggest a poor prognosis for those requiring ventilation support, there is a subgroup who will eventually be weaned off. As the pandemic evolves, this cohort of infected, chronically intubated and ventilated individuals will become more prevalent and may require tracheostomy to aid in recovery. Unfortunately, tracheostomy is an aerosol-generating procedure which poses high risks to all members within the operating room, as described by previous authors. There is an urgent need to explore and develop methods to maximize the safety of tracheostomy and other aerosol-generating procedures in order to reduce intraoperative transmission. In the present article, we present a modified technique for negative pressure enclosure in patients with COVID-19 who underwent tracheostomy.
Introduction
In December 2019, a novel betacoronavirus termed severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was first reported to outbreak in Wuhan, Hubei province, China. Patients infected with this virus typically develop an ensuing respiratory illness, referred to as COVID-19. The high transmissibility of SARS-CoV-2 has resulted in a global crisis, prompting official declaration as a pandemic by the World Health Organization on March 11, 2020. 1 Transmission typically occurs through the spread of aerosolized respiratory droplets or through contract with infected surfaces. 2 The clinical spectrum of COVID-19 ranges from mild, self-limited respiratory infection to severe pneumonia with respiratory distress syndrome, multi-organ failure, hypercoagulability, and even death.3-5 According to early data from Wuhan, China, approximately 9.8% to 15.2% of patients ultimately require intubation and mechanical ventilation or extracorporeal membranous oxygenation.3,4,6 Prolonged ventilatory support is often required secondary to virus-mediated diffuse alveolar damage from cellular fibromyxoid exudate and hyaline membrane formation that compromise oxygenation. 7 Data also suggest that the prognosis of patients with COVID-19 who require intubation is extremely poor at less than 20%.8-11 Individuals at highest risk—and most likely to require intubation—include the elderly (>70 years of age) and those with comorbidities (eg, diabetes, and immunocompromise) and have an estimated mortality from 14% to 49%.6,8,10,11
As the number of patients with COVID-19 continues to rise, a growing population of patients who require long-term intubation and mechanical ventilation will exist. Typical management principles for these individuals may include tracheostomy as this step can enhance nursing care, improve patient comfort, and reduce the need for prolonged sedation and associated delirium. 12 However, this population in particular presents a unique challenge, as tracheostomy is an aerosol-generating procedure that inherently increases the risk of transmission to health care providers and subsequent nosocomial spread. 13 Nevertheless, there has been a shift among some surgeons to modify techniques as an extension of personal protective equipment (PPE) to minimize transmission to health care providers.
At the time of this publication, current professional otolaryngology societies published guidelines for performing tracheostomy in this population.14-16 These guidelines also recommend against tracheostomy in COVID-19-positive patients and suggest waiting until a patient tests negative. However, this is controversial given the poor reliability of testing methods with variable rates of false negatives as high as nearly 30%,17-19 as well as the unclear correlation between detectable viral RNA load measured in most widely available tests and the isolation of infectious virus. 20 These guidelines do not reference any methods of draping or room setup other than using negative pressure operating theaters to supplement standard PEE in mitigating the spread of aerosolized virus.
Recently, there have been reports of creative attempts to address this gap in both practice and knowledge for those performing tracheostomies in patients with COVID-19.21,22 Specifically, surgeons have constructed a negative pressure space immediately surrounding the patient using a clear protective covering over the surgical field in conjunction with both high-efficiency particulate air (HEPA) filters and a smoke evacuator.21,22 In the present article, we demonstrated the use of a modified technique for negative pressure enclosure during tracheostomy in 4 intubated patients infected with SARS-CoV-2.
Protocol and Setup
Patient Selection
Patient selection was determined with multidisciplinary input from pulmonary, critical care, and surgical services at both institutions. FiO2 and PEEP demands,
Methods
All procedures were performed in designated infectious control operating rooms with negative pressure configuration for patients with COVID-19. Specifically, these rooms interfaced with the remaining facility via a negative pressure area for donning and doffing.
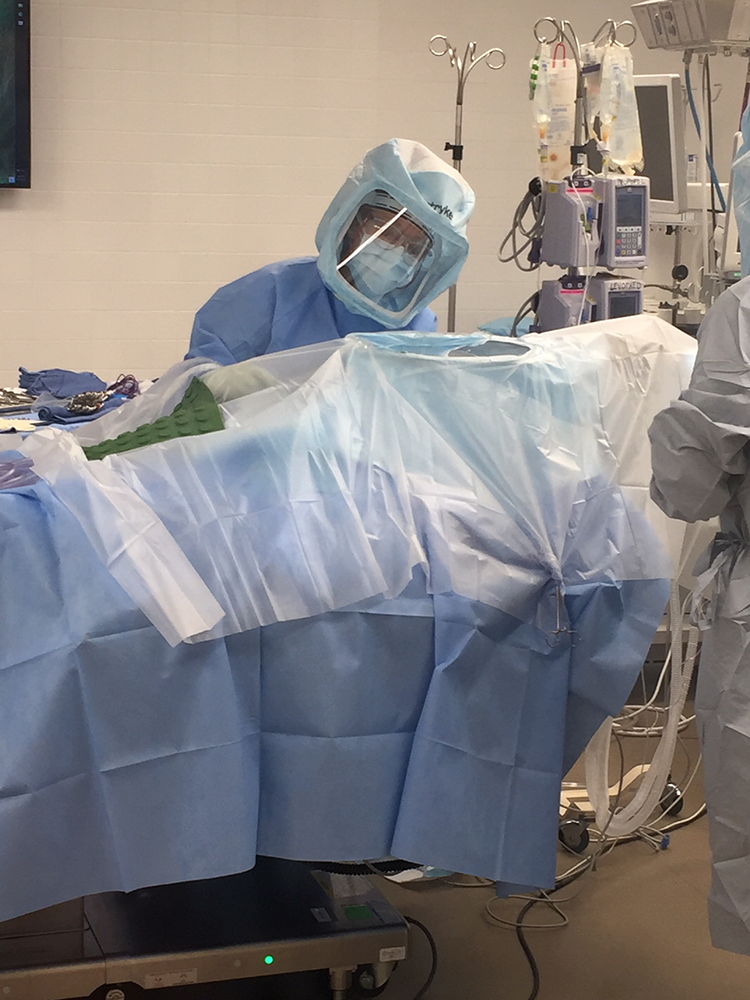
In addition to standard tracheostomy setup, an additional draping phase was performed as follows: a Bookwalter post (Symmetry Surgical) with associated self-retaining retractor ring was centered over the surgical field (Figure 1A); a visor from a large orthopedic operating hood was placed over the ring to act as the visible window (Figure 1B). Enclosure was achieved with numerous adhesive 1015 Steri-Drape U-Drapes (3M) surrounding the field and attached to the perimeter of the visor (Figure 1C). This enabled clear visualization of the surgical field (Figure 2). The area within the enclosure was limited from the mid-chest to the top of the head by placing the instrument magnet on top of the clear drapes (Figure 3). Negative pressure was achieved by connecting large tubing to a HEPA filter with a high-flow external vacuum and placing the open end of the tubing within the enclosed space (Figure 4). Pairs of hand ports were created on 3 sides through the plastic drapes to provide access for the surgeon, assistant, and anesthesia provider (Figure 5).
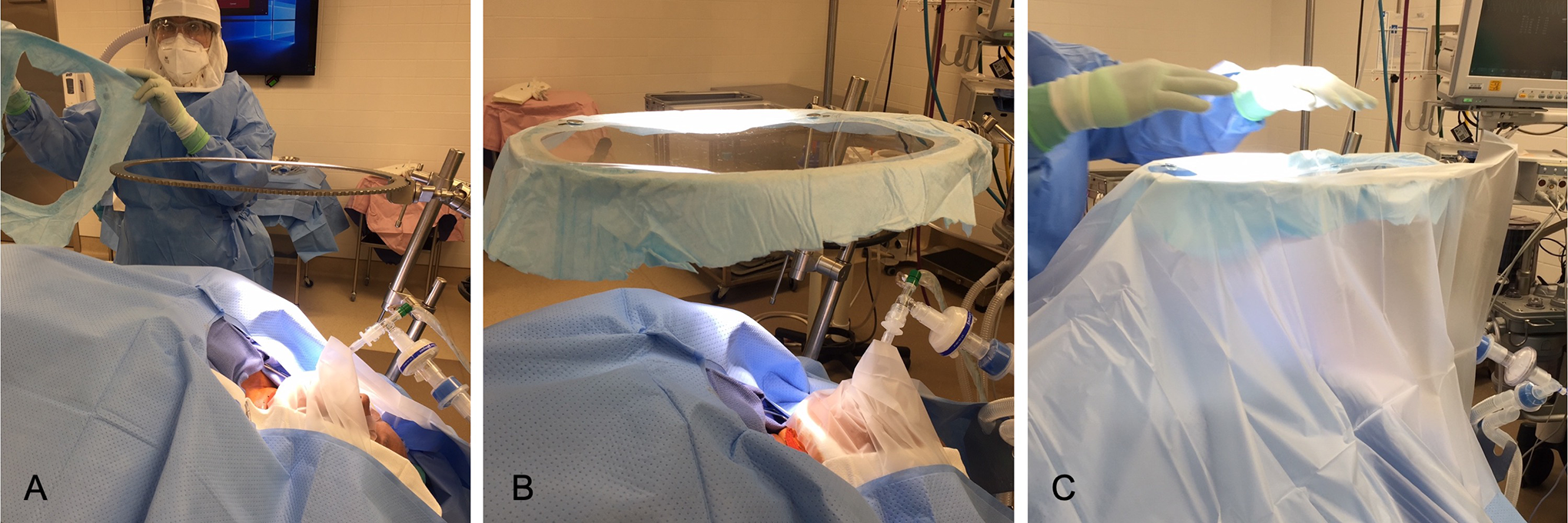
Assembly of the visor window. A book walter post with associated self-retaining retractor ring was centered over the surgical field (A) and a large orthopedic hood visor was positioned on top to create the window (B). Enclosure was achieved with numerous adhesive drapes surrounding the field and attached to the perimeter of the visor (C).
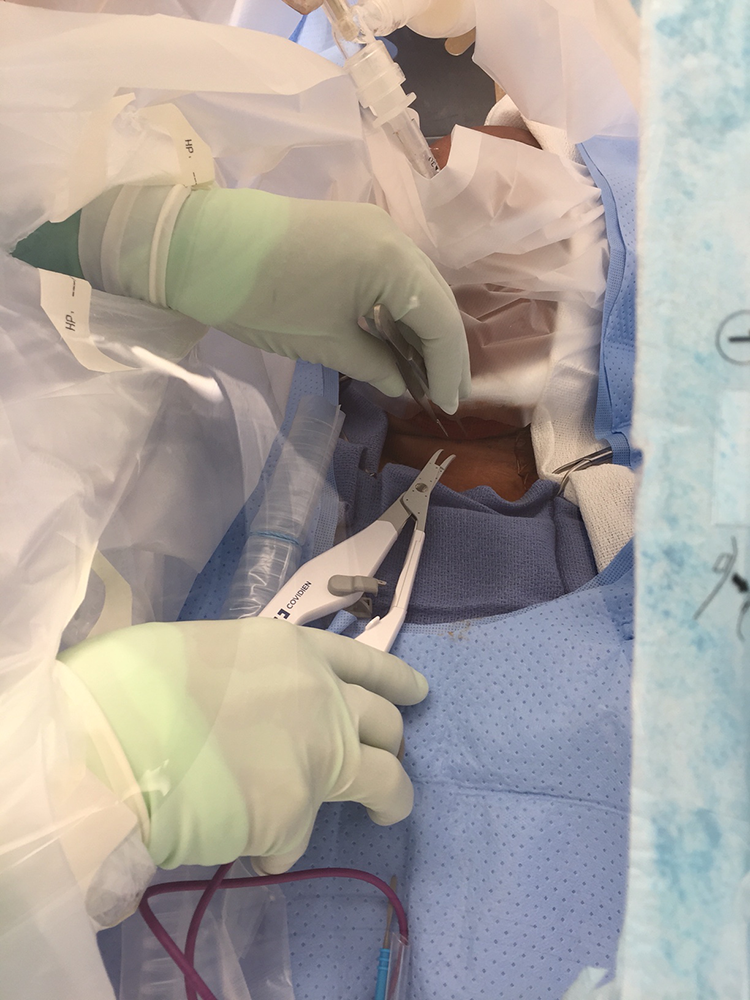
Visualization of the surgical field through the visor window.
The volume of the enclosure is limited by placing the magnetic mat on top of the adhesive surgical drapes inferior to the surgical site.
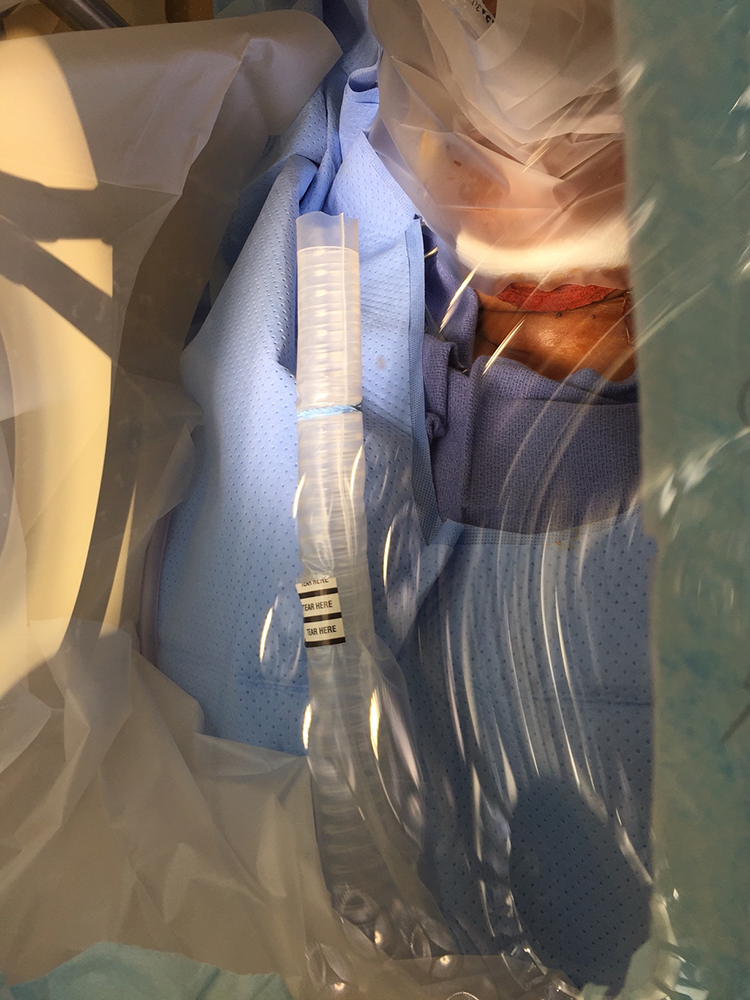
Negative pressure was created within the enclosed space by placing large tubing adjacent to the surgical field and connecting it to a high-efficiency particulate air (HEPA) filter with a high flow external vacuum.

Pairs of hand ports were created on 3 sides through the plastic drapes to accommodate access by surgeon, assistant, and anesthesiologist.
Tracheostomy was performed with ligature (Medtronic) technique as the main energy device in association with monopolar cautery. Ventilation was held during tracheal fenestration and during tube exchange. After performing tracheostomy with tube exchange, negative pressure remained in place for 5 minutes before the setup was taken down. This duration was based on the approximate time it would take for complete air filtration based on estimated enclosure volume and the specified rate of filtered cubic feet per minute of our specific filtration device.
The technique described herein was considered an extension of PPE and was therefore determined to be exempt from review by our institutional review board.
Discussion
We present a modified version of a negative pressure enclosure constructed from widely available standard operating room materials. This technique modifies previous reports on tracheostomy in this population by enhancing visualization through the use of a visor “window.” This visor enables clear visualization of the surgical field without obstruction from overlapping of material and subsequent glare. 21 Furthermore, we improve upon previous strategies by reducing enclosed volume of the negatively pressurized space through air filtration. Reducing overall tented volume may improve negative pressure distribution and reduce dead space pockets for aerosolized viral pockets to develop, although this has yet to be proven.
There were no issues with fogging of the visor encountered during these cases. Visualization is crucial during tracheostomy, especially for obese patients who often have deep stomal wounds due to excessive soft tissue. The height of the visor from the wound can also be adjusted to accommodate instrument maneuverability. The second objective was to decrease dead space volume from previous techniques within the negatively pressurized space, thus maximizing air filtration efficiency. Reducing dead space volume may theoretically reduce viral accumulation and possible oxygen pocket formation which may evade the negative pressure apparatus with previous techniques.
The authors prefer using electric cauterization energy devices despite preliminary guidelines discouraging this practice to reduce the likelihood of viral aerosolization with cauterization of respiratory mucosa.15,23-25 Our preference addresses the fact that many patients with advanced COVID-19 respiratory failure are managed with anticoagulation therapy, which can complicate intraoperative hemostasis. The authors utilized monopolar cautery with ligature to address small vessel bleeds in subcutaneous fat, as well as during thyroid division and airway fenestration. Furthermore, the propensity for persistent postoperative bloody secretions resulting from suboptimal intraoperative hemostasis may present a greater delayed risk of viral transmission to critical care supporting staff.
Tantamount to procedural setup is the thoughtful consideration of patient candidacy for tracheostomy. Thorough assessment of pulmonary stability should be performed, ensuring that eligible patients can safely tolerate an apneic pause of 30 to 45 seconds—as this emulates the paused ventilation period during tracheostomy tube exchange essential for reducing aerosolization.14-16,26 In addition, potential candidates should demonstrate tolerance to periods of reduced Fi
We recommend that the decision on timing should be made in the context of currently available resources and in collaboration with the family and intensive care team. In addition to the aforementioned benefits of tracheostomy, transition from endotracheal intubation may also help address critical ventilator shortages.
Until therapeutic closure and or protective immunity exist, providers will continue to face the unprecedented challenge of providing care for their patients while minimizing transmission risk to themselves and other health care personnel. More than ever, providers must lean on resourceful thinking and interdisciplinary collaboration. As COVID-19 cases continue to permeate hospitals globally, it is paramount that patients who may benefit from tracheostomy can receive proper care with attention to maximize PPE. With transmission occurring predominately through respiratory secretions, all health care personnel that manage aerodigestive tract issues (otolaryngologist-head and neck surgeons, dentists, maxillofacial surgeons, gastroenterologists, pulmonologists, and anesthesia providers) are most susceptible27,28 and should continue to develop innovative ways to deliver safe care to their patients.
Although this procedure has been safely demonstrated without complication in 4 patients, this technique has inherent limitations. Although the visor is essential to improving visualization, translucency of this surface can be compromised from inadvertent spray of blood intraoperatively. If encountered, the operative room technician can wipe the visor from within the protective covering. Furthermore, it is imperative that standard precautions be taken to reduce high concentration oxygen from accumulating within the enclosure. Theoretically, the small volume within the negative pressure cover could permit pockets of oxygen in high concentration, thus increasing fire risk, highlighting the importance of an efficient air turnover system. Nevertheless, this modified technique is a safe approach to promote extended personal protection of operating room personnel with COVID-19 patients who undergo tracheostomy.
Conclusions
COVID-19 can result in acute respiratory distress and require prolonged intubation with mechanical ventilation. In select patients who achieve pulmonary stability, tracheostomy can be performed using this modified negative pressure enclosure that does not compromise visualization of the surgical field. The aforementioned technique is safe and cost-effective which modifies the use of readily available surgical instruments and supplies that extend PPE to operating room personnel. Until therapeutic closure of COVID-19 exists, surgeons will need to continue to adapt and find ways to safely deliver appropriate care to their patients, regardless of COVID-19 status.
Footnotes
Authors' Note
Howard P. Boey is also affiliated with Frank H. Netter MD School of Medicine at Quinnipiac University, North Haven, CT, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.