
Abstract
Objective:
To investigate the effects of the mechanical trauma to the round window, a model electrode inserted into the scala tympani on the cochlear reserve, and the efficacy of topical steroids in preventing hearing loss.
Materials and Methods:
21 male Wistar Albino rats were equally categorized into three groups. In all groups an initial mechanical injury to round window was created. Only subsequent dexamethasone injection was administrated into the cochlea in the subjects of group 2 while a multichannel cochlear implant guide inserted into the cochlea prior to dexamethasone administration for group 3. Distortion product otoacoustic emissions (DPOAEs) were obtained prior to and immediately after the surgical injury, eventually on postoperative seventh day (d 7). Mean signal/noise ratios (S/Ns) obtained at 2000, 3000, and 4000 Hz were calculated. Data sets were compared with non-parametric statistical tests.
Results:
The early intraoperative mean S/Ns were significantly less than preoperative measurements for group 1 and 2; however, preoperative and postoperative d 7 average S/Ns did not differ. There was statistically significant difference between preoperative, intraoperative and postoperative d 7 average S/Ns for group 3.
Conclusion:
We observed that hearing was restored approximately to the preoperative levels following early postoperative repair. However, an electrode insertion into the cochlea via round window subsequent to mechanical trauma seems to cause a progressive hearing loss. Therefore, a special care must be taken to avoid the injury to the round window membrane in the course of the placement of a cochlear implant electrode and surgery for the chronic otitis media.
Introduction
Hearing impairment is basically classified as conductive, sensorineural and mixed. Sensorineural hearing loss may develop due to different factors and for the rehabilitation, middle ear and cochlear implants have been increasingly used. Therefore, the round window approach is becoming more important in the rehabilitation of children and adults with severe- to-profound hearing loss due to the use of cochlear implants (1).
Some studies report that manipulations around the round window negatively affect the cochlear reserve (2,3). Use of the topical steroids has been suggested for preventing the onset of apoptosis on the cellular level following mechanical or acoustic trauma (4). The current study aimed to investigate the effects of acute trauma resulting from manipulations of the round window, and a model electrode inserted into the scala tympani on the cochlear reserve. Furthermore, the efficacy of topical steroids in preventing hearing loss was assessed.
Material and Methods
Subjects
Twenty-one Wistar Albino (SD) rats weighing about 250-330 (mean, 285 gr) gram were included for the study. The rats were randomly selected and divided into 3 groups of 7 animals, and maintained in a habitat in which background noise was less than 50 dB. All animal experiments were carried out with approval of Ethics Committee of Ege University and at experimental surgery department.
Anesthesia
General anesthesia was provided with intraperitoneal administration of 45 mg / kg ketamine hydrochloride (Ketalar, Daiichi Sanyko Co., Ltd., Tokyo, Japan) and 5 mg / kg xylazine (Rompun, Bayer Health Care, Germany). The additional 25 mg / kg ketamine hydrochloride and 5 mg / kg xylazine was administrated intraperitoneally in the case of need.
Surgical approach
In all patients a retroauricular skin incision was made in the posteroinferior part of the right ear. The muscles were divided via blunt dissections and the tympanic bulla was exposed (Figure 1). The tympanic bulla was incised with a no. 11 scalpel in order to reach the middle ear and the round window membrane was punctured using a pick. Then, a microperforation of 1-2 mm in diameter was created. The perilymph was allowed to flow for approximately 5 s. For group 2, subsequent injection of approximately 0.5 ml dexamethasone into the tympanic bulla was performed. For group 3, a Nucleus multichannel implant guide (Cochlear Ltd., Sydney, Australia) 0.4 mm in diameter and made from platinum inserted into the scala tympani to a depth of 1-2 mm, followed by dexametason injection into the tympanic bulla. After a few minutes, the round window opening was obliterated with muscle and the incision was sutured with 4-0 rapid polyglactin in all 3 groups.
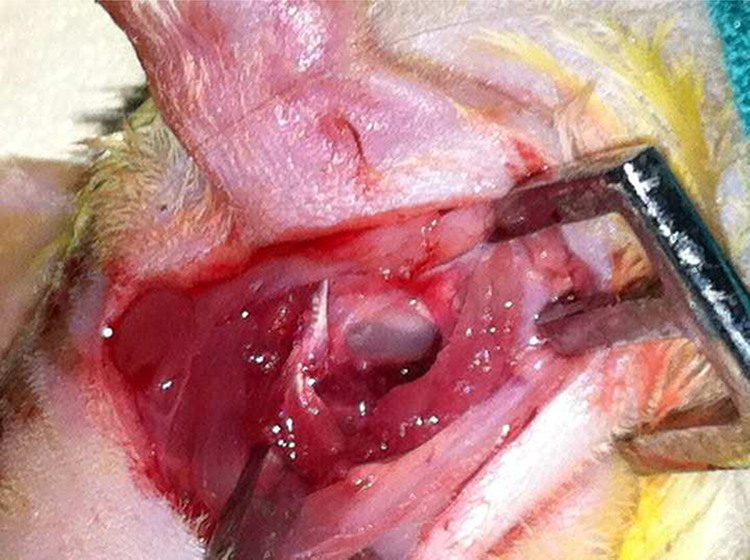
Tympanic bulla is seen.
Preoperative emissions could not be obtained in the right ear of 1 rat due to tympanic membrane rupture. 1 rat of group 1 died within the post procedure first 24 hours; cause of the death was assumed to be bleeding during the surgery. These two rats were excluded from the study and replaced with two others.
Audiological examination
We used a GSI AUDIO screen T device (Grason-Stadler, Inc.) and a probe developed for premature infants for the measurements of otoacoustic emissions in rats. DPOAEs were measured in each rat bilaterally during the preoperative period. The test began after determining that the probe indicator and stimulator waveform of the device were set to the proper measurement positions. The rats in which no emissions were obtained were excluded. The S/Ns were recorded via DPOAEs at 2000, 3000, and 4000 Hz (at 2f1-f2 frequency, with L1 = 65dB and L2 = 55dB).
Hearing levels of both ears were tested with repeated DPOAEs post surgically for two times; immediately before the animals recovered from anesthesia and 1 week later. In the latter, rats were under intraperitoneal local anesthesia with 45 mg/kg of ketamine hydrochloride during the procedure.
Statistical Analysis
Data were analyzed using Prism GraphPad software version 5.0d (La Jolla, CA). The differences in DPOAE values between and in each group were compared using Mann– Whitney U and the Kruskal-Wallis tests. Comparisons were considered significant when p<0.05.
Results
Present study revealed that there was not statistically significant difference for the preoperative average S/Ns among all groups (p=0.39). However, the mean S/Ns values were significantly less for intraoperative vs. preoperative period for group 1 and 2 (p=0.02 for both groups) (Table 1) while it did not differ on the preoperative and postoperative d 7 (p=0.25 and 0.16, respectively). There was statistically significant difference between preoperative, early post operative and postoperative d 7 average S/Ns of group 3 (p=0.01) (Table 2).
Comparison of Preoperative and Postoperative DPOAEs Results of Group 1 and 2.
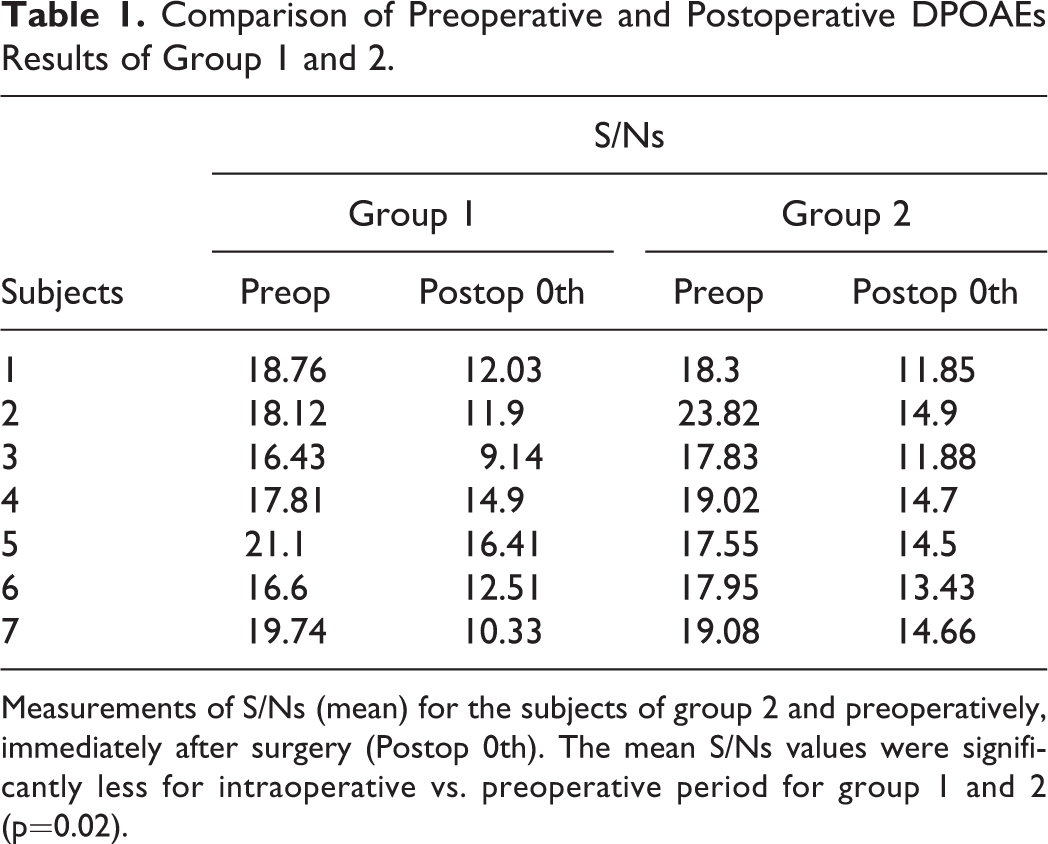
Measurements of S/Ns (mean) for the subjects of group 2 and preoperatively, immediately after surgery (Postop 0th). The mean S/Ns values were significantly less for intraoperative vs. preoperative period for group 1 and 2 (p=0.02).
DPOAEs Results of Group 3.
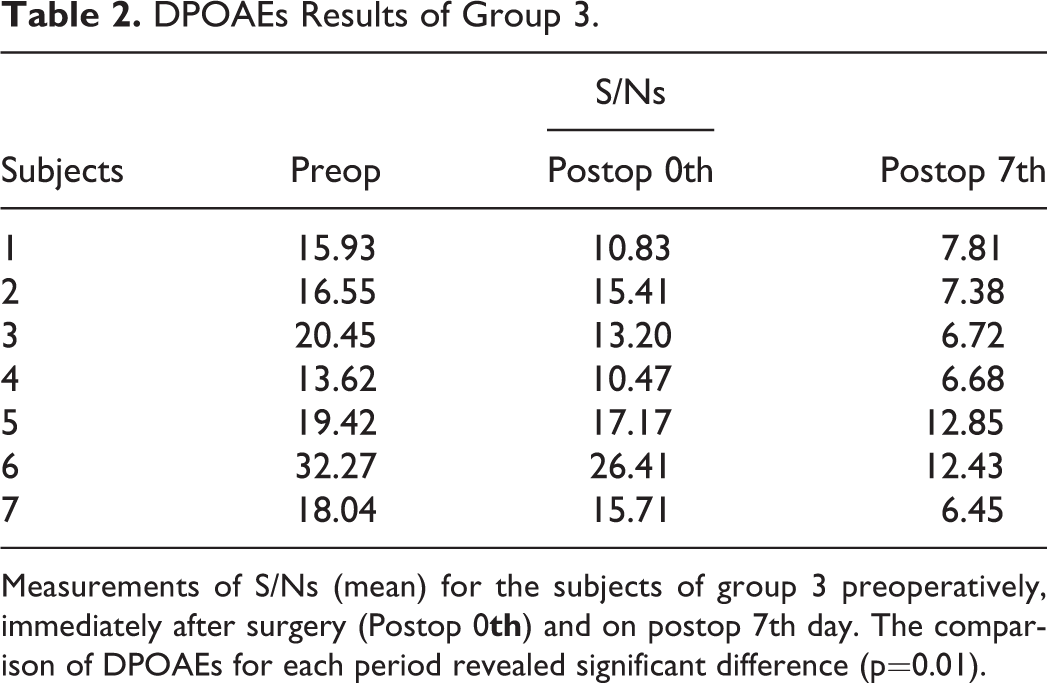
Measurements of S/Ns (mean) for the subjects of group 3 preoperatively, immediately after surgery (Postop 0
The postoperative d 7 average S/Ns of all groups were compared using Kruskal Wallis test. There was statistically significant difference among all groups (p=0.03). However, it did not differ for group 1 and 2 (p=0.71), while it was statistically less for group 3 vs. group 1 and 2 (p=0.002).
There was not statistically significant difference between preoperative, intraoperative and postoperative d 7 average S/Ns of the left ear (control group) for all the groups (p=0.85).
Discussion
Hearing loss is one of the most common complaints of patients who present to otorhinolaryngology clinics. Nowadays, for the treatment of advanced sensorineural hearing loss application of cochlear implantation has become widespread. Nevertheless, negative effects of cochlear electrode and cochlear implantation itself on residual hearing have been reported (1,2,3).
Otoacoustic emissions are low-intensity, nonlinear acoustic signals produced at the pre-neural level by cochlear hair cells. DPOAEs are measured by producing 2 pure tones at a constant frequency and intensity. In the normal cochlea, these 2 tones generate 2 different waves, and DPOAEs are formed by the otoacoustic emissions generated by the part of the cochlea in which these 2 waves overlap, which enables obtaining frequency-specific information from the cochlea (5). Round window membrane and scala tympani injury causes hair cell injury, most frequently at the basal turn of the cochlea, resulting in hearing loss. DPOAEs (2f1-f2) are important for evaluating hearing loss that originates in this region (6). In the present study hearing data were obtained using DPOAEs, and mean S/N ratios obtained at 2000, 3000, and 4000 Hz were evaluated. It has been reported that drilling during mastoidectomy and in the middle ear might cause hearing impairment due to both mechanical and acoustic trauma (7,8,9). In the present study we incised the tympanic bulla with a No. 11 scalpel in order to avoid drilling-associated acoustic trauma.
Our preliminary data showed that there was statistically significant difference between preoperative average of S/Ns and early intraoperative period data in groups 1 and 2; however, preoperative and postoperative d 7 data did not differ. It was reported that there weren’t any alterations in hearing measured using auditory brainstem response ABR after round window membrane injury, but that hearing thresholds increased when Reissner’s membrane and the stria vascularis were injured (10). In contrast, Eshraghi et al. reported that round window membrane injury alone caused hearing loss, as measured by DPOAEs and ABR, and hearing improved later (11).
In the present study round window membrane injury in groups 1 and 2 caused sensorineural hearing loss in the early period; however, the values obtained on postoperative d 7 were close to the preoperative values. In the light of these findings we think that perilymph leakage after round window membrane injury alone causes sensorineural hearing loss in the early period and that hearing returns to normal in response to simple surgical interventions that prevent perilymphatic leakage, whether or not dexamethasone is administered. The present results are similar to those reported in studies in which an experimental round window fistula was created, resulting in hearing loss in the early period (11,12,13).
The insertion of the electrode guide of Nucleus cochlear implant into the cochlea in addition to round window membrane injury for group 3, caused long-term irritation. In group 2 preoperative, intraoperative, and postoperative d 7 S/N ratios were significantly different. In contrast to groups 1 and 2, DPOAE measurement on postoperative d 7 showed that there was progressive loss of hearing.
Cochlear implants made great progress in the rehabilitation of children and adults with severe-to-profound hearing loss, and as an implantation site the use of the round window is increasing in importance. The electrode of a cochlear implant is inserted into the scala tympani through the round window, with the aim of minimal trauma and maximal neural stimulation. As the indications for use of cochlear implants expand, preservation of residual hearing, especially in the low frequencies, is increasing in importance (14). It was reported that insertion of a cochlear implant electrode causes hearing impairment via two different mechanisms (12). Acute trauma is due to the physical injury the electrode causes to the cochlea, especially the hair cells. Late trauma develops due to reactive oxygen species that appear in the environment due to oxidative stress (15).
Eshraghi et al reported the hearing loss resulted from cochlear implant electrode- related early and late trauma. This result was suggested to be due to exposure of the hair cells to oxidative stress, local inflammation and death of the outer hair and ganglion cells, rather than the mechanical effect of the electrode (11). Preventing this condition is important, especially for preserving residual hearing. In addition to round window injury in groups 1 and 2 of the present study, a cochlear implant was inserted into the scala tympani for group 3 in order to cause continuous irritation, and unlike in groups 1 and 2, progressive hearing loss was observed in group 3. Additionally, for group 3 dexamethasone was injected into the cochlea, as in group 2.
In the present study intracochlear dexamethasone administration did not reverse progressive hearing loss for group 3. The rats were retested 1week after surgery and, therefore, a conclusion regarding long-term results is not possible. Balkany et al. used special equipment to administer intracochlear dexamethasone to guinea pigs, so as to prevent late inflammatory effects associated with oxidative stress and cell death and reported that progressive hearing loss was prevented (6).
Conclusion
The present study aimed to investigate how destruction of the round window membrane and insertion of a cochlear implant into the scala tympani cause irritation effects on residual hearing, the protective effect of administration of local corticosteroid. Our preliminary results indicate that injury to the round window membrane (membrana secundaria) caused sensorineural hearing loss and hearing was restored approximately to the preoperative levels following early postoperative repair. However, chronic irritation of scala tympani with the insertion of cochlear implant guide following round membrane injury was resulted with progressive hearing loss. We think that this was due to localized inflammation and oxidative stress caused by the cochlear implant’s electrode. Additional research is required to better understand how residual hearing in cases of inner ear surgery performed with the round window approach can be preserved, especially when a cochlear implant is inserted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.