
Abstract
Objective:
Benign paroxysmal positional vertigo (BPPV) is characterized by recurrent attacks of vertigo caused by head movements. It occurs as a result of otoconia falling into the semicircular canal. Calcium and 25 hydroxyvitamin D [25(OH)D] metabolism in the inner ear play an important role in otoconia formation and degeneration. Our aim in this study was to investigate the relationship between 25(OH)D levels and BPPV.
Methods:
This retrospective, case–controlled study included 52 patients with posterior canal BPPV and 52 controls aged 18 to 80 years. Age, sex, serum calcium, corrected calcium, and 25(OH)D levels of the BPPV and control group were compared.
Results:
Twenty-three of the patients were male (44.2%) and 29 were female (55.8%). The average age was 55.6 years. The 25(OH)D level was 15.3 ng/mL in the BPPV group and 20.2 ng/mL in controls. There was no significant difference in 25(OH)D and albumin-corrected calcium values (P = .394; P = .084, respectively). In 80.7% of the BPPV group and 61.5% of the controls, 25(OH)D levels were 20 ng/mL and below. 25 hydroxyvitamin D deficiency was found statistically significantly more frequently in patients with BPPV (P = .030).
Conclusion:
In our study, serum 25(OH)D levels were found to be lower in patients with BPPV, and the rate of vitamin D deficiency was higher in these patients. Based on these results, it is recommended to examine the 25(OH)D levels of patients with BPPV at the time of diagnosis.
Introduction
Benign paroxysmal positional vertigo (BPPV) causes dizziness, nausea-vomiting, and nystagmus, which occur with head movements. It is the most common vestibular disease. Prevalence increases with age, from 0.5% at age 18 to 39 years, increasing to 3.4% after age 60 years. The lifetime cumulative incidence of the disease rises to 10% at age 80 years.1,2 It is more common in females and most cases are idiopathic. The posterior canal is affected in 90% of cases. The Dix–Hallpike provocation test is used in the diagnosis of posterior canal BPPV, and the Epley repositioning maneuver is mainly used in the treatment of the disease. 3
In BPPV, otoconia, which are broken from the utricular macula and are composed of calcium carbonate, fall into the semicircular canals and change the endolymph flow dynamics, sometimes sticking to the cupula and causing symptoms. Calcium metabolism in the endolymph is an important part of the synthesis and absorption of otoconia. Recently, studies investigating the relation between 25-hydroxy vitamin D [25(OH)D], bone metabolism, calcium, and BPPV have been conducted. 4 Although some studies have shown a relation between idiopathic BPPV formation and recurrence and low 25(OH)D, a few studies found no correlation.5,6 We investigated serum 25(OH)D, calcium, and calcium values corrected according to albumin in patients with posterior canal BPPV.
Material Method
The Erzincan Binali Yıldırım University Local Ethics Committee approved the study, which was conducted in accordance with the Declaration of Helsinki. The medical records of patients with BPPV who were diagnosed between January 2018 and February 2019 were analyzed retrospectively. The study included 52 patients with posterior canal BPPV aged 18 to 80 years. The control group was formed by investigating individuals who were examined in our clinic and on whom blood tests were performed. The Dix–Hallpike test was performed for the diagnosis of all patients and controls. Patients and controls were excluded if they had horizontal or anterior canal BPPV, a history of ear surgery, Meniere’s disease, vestibular neuritis, chronic otitis media, diagnosed osteoporosis, or vitamin D treatment at the time of BPPV diagnosis.
The patient group and control group were compared retrospectively in respect of age, sex, serum calcium, albumin, and 25(OH)D concentrations. Plasma 25(OH)D was measured using a liquid chromatography-tandem mass spectrometer (LC-MS; Agilent Technologies 6440 TripleQuad LC-MS/MS). 25 hydroxyvitamin D levels ≤20 ng/mL were classified as deficient. Calcium and albumin were measured from serum using spectrophotometry (Beckman Coulter Olympus AU2700 Plus Chemistry Analyzer). The corrected calcium level was calculated using the following formula: Corrected calcium (mg/dL) = measured total Ca (mg/dL) + 0.8 (4.0 − serum albumin [g/dL]).
Statistical Analysis
Data were analyzed statistically using the Statistical Package for the Social Sciences for Windows version 22.0 software (SPSS Inc). Descriptive statistics are stated as mean ± standard deviation (SD), or median (minimum-maximum) values, frequency distribution (n), and percentage (%). The χ2 test or Fisher exact test was used to compare categorical variables. The conformity of the data to normal distribution was examined using visual and analytical methods. Independent groups of variables with normal distribution were compared using the t test, and the Mann-Whitney U test was used for variables that did not show normal distribution. A value of P < .05 was accepted as statistically significant.
Results
Fifty-two patients with BPPV and 52 healthy control cases were included in the study. The patient group comprised 23 (44%) males and 29 (56%) females. The average age of the patient group was 55.6 (median, 60; range, 18-80) years. The control group comprised 18 (34.6%) males and 34 (65.4%) females. The average age of the controls was 51.1 (median, 54; range 22-87) years. There was no significant difference between the patients and the controls in terms of age and sex (P = .055, P = .316, respectively; Table 1).
Characteristics of Patient and Control Groups.
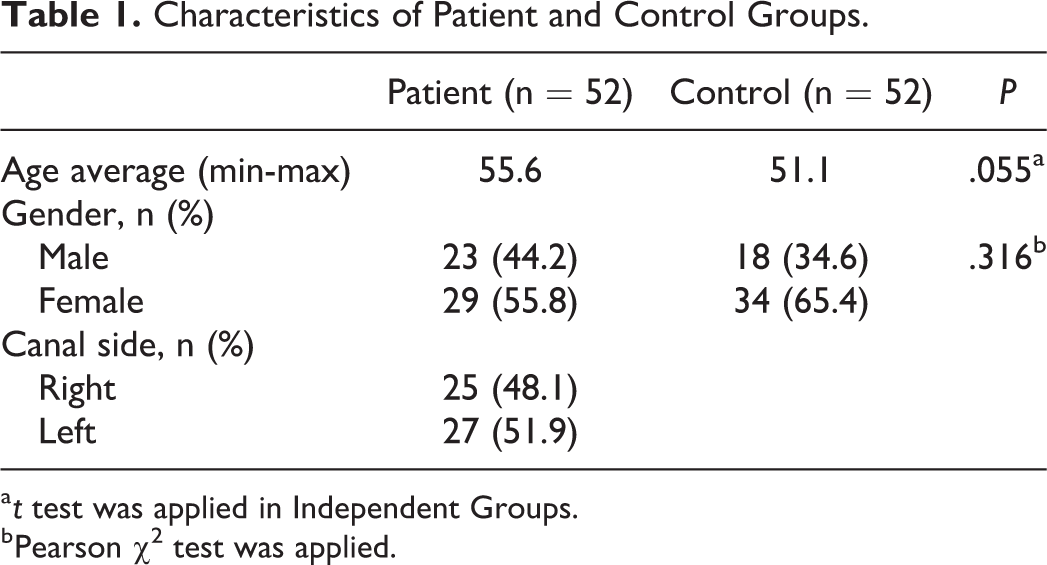
a t test was applied in Independent Groups.
b Pearson χ2 test was applied.
There was no significant difference between the BPPV and control groups in respect of the 25(OH)D and corrected calcium values (P = .394, P = .084, respectively). The average 25(OH)D level was 15.3 ng/mL in the patients with BPPV and 20.2 ng/mL in the control group. The 25(OH)D level was ≤20 ng/mL and below in 80.7% of the BPPV group and 61.5% of the controls. The rate of 25(OH)D deficiency was statistically significantly higher in patients with BPPV (P = .030; Table 2).
Comparison of Blood Values of Groups.
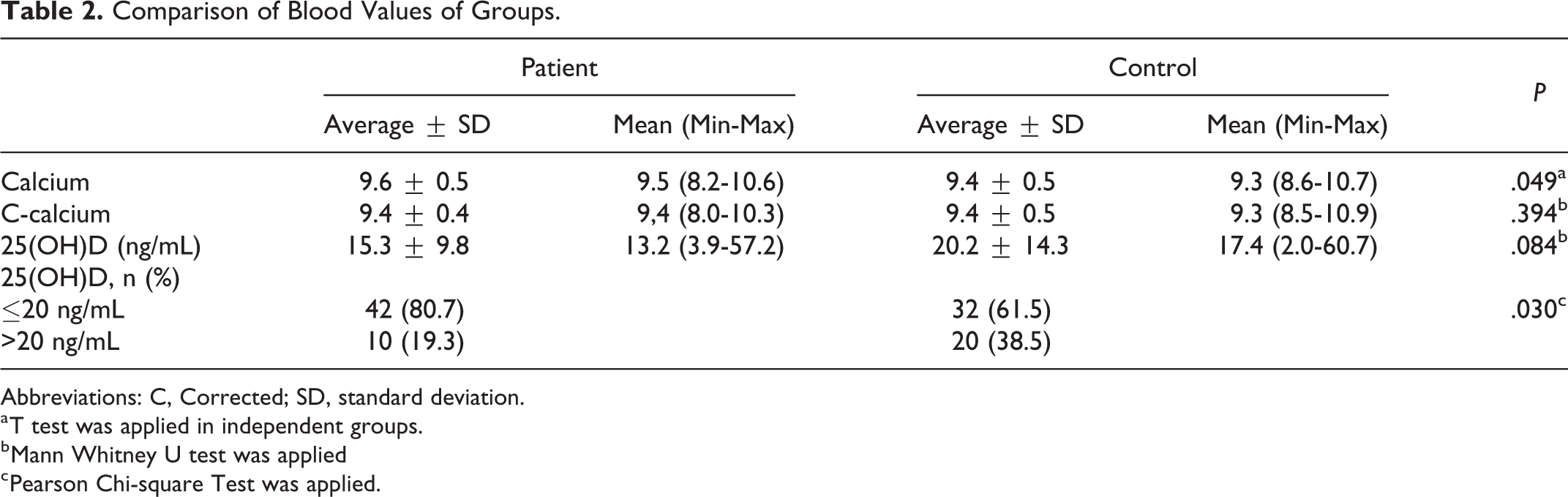
Abbreviations: C, Corrected; SD, standard deviation.
a T test was applied in independent groups.
b Mann Whitney U test was applied
c Pearson Chi-square Test was applied.
Discussion
Otoconia are formed as a result of calcium carbonate precipitation on a glycoprotein core. The formation, development, and degeneration stages of otoconia occur as a result of active calcium metabolism in otolith vestibular organs. 7 Impaired Ca2+ metabolism in osteoporosis and osteopenia has been shown to cause BPPV. 5 25 hydroxyvitamin D organizes the expression of some Ca2+ binding proteins and receptors in the inner ear. 8 A shift in acidic pH in the endolymph and the change in Ca2+ levels may lead to a decrease in the size of otoconia and deformity. 9 Therefore, it has been suggested that vitamin D disorders might affect calcium metabolism in the inner ear, leading to the development of BPPV. 10 Lee et al 11 reported that patients with vitamin D deficiency and high osteoporotic bone destruction had a higher prevalence of BPPV, which might have developed as a result of deterioration in calcium hemostasis, which is known to be effective in the formation of otolith in the inner ear.
In a study of 80 patients with idiopathic BPPV, decreased serum 25(OH)D levels in patients with BPPV were reported, which was similar to that of our study. Moreover, 25(OH)D levels were significantly lower in the recurrent BPPV group compared with the nonrecurrent BPPV group. 12 All these findings support our study, in which only patients with posterior canal BPPV were included to provide a homogeneous group. In another study, bone mineral density and 25(OH)D levels of 130 patients with idiopathic BPPV and 130 age and sex-matched controls were compared. Low 25(OH)D levels in males were shown to be associated with the occurrence of BPPV. 8 Parham et al 13 studied postmenopausal females in 2 groups, 16 patients in the BPPV group and 13 patients in the osteoporosis group. Serum levels of serum ionized calcium and 25(OH)D were compared and they found a negative correlation with serum vitamin D levels and BPPV.
Some studies reported that deficiency of vitamin D could cause recurrence as well as BPPV formation. Rhim et al 14 retrospectively reviewed 232 patients with BPPV, separating the patients into 2 groups as recurrent and nonrecurrent. Age, sex, follow-up time, BPPV type, and 25(OH) D levels were investigated. Recurrence was detected in 41 patients (17.7%). The average concentration of 25(OH)D in the nonrecurrent group was 16.63 ng/mL, whereas in the recurrent group it was 13.64 ng/mL. The difference was statistically significant. Similar to our study, the frequency of vitamin D deficiency in the BPPV group was statistically significantly higher compared with the control group. However, unlike the previous study, only patients with posterior canal BPPV were included in our study. In another study that compared 25(OH)D levels of 174 patients with BPPV and 348 controls, a relation was found between decreased serum 25(OH)D levels and the formation and recurrence of BPPV. 15 In our study, we found serum 25(OH)D levels 15.3 ng/mL in the BPPV patients and 20.2 ng/mL in the control group. Although there was no significant difference in 25(OH) D levels, it was lower in BPPV patients (P = .084). This may be due to relatively small number of study population. Another factor may be that low 25(OH)D levels can also be seen in the normal population.
Recently, it has been recommended that 25(OH)D should be measured in patients with BPPV and vitamin D supplementation should be administered as necessary. Vitamin D deficiency treatment has been reported to reduce recurrence and the severity of the disease. In a study evaluating patients with idiopathic posterior canal BPPV and 25(OH)D levels of <10 ng/mL, all patients were given 25(OH)D treatment; 25(OH)D levels were measured at diagnosis and 3 months after the treatment. In the third month, the patients were divided into 2 groups, group 1 comprised 28 patients with 25(OH)D levels >10 ng/mL and group 2 constituted 65 patients with serum 25(OH)D levels <10 ng/mL. These groups were followed up for 18 months to observe BPPV recurrence, which was seen to occur in 4 (14%) patients in group 1 and 28 (43%) in group 2. It was concluded that increasing 25(OH)D levels with vitamin D treatment would decrease the number of recurrence attacks in patients with BPPV. 16 Sheikhzadeh et al 17 examined the effect of 25(OH)D deficiency (<20 ng/mL) treatment on healing time in BPPV and showed an additional benefit to the Epley maneuver. It was also recommended that serum 25(OH)D should be measured in patients with recurrent BPPV.
Vestibular disorders negatively affect the daily life of patients and can lead to workforce losses. Clarification of the causes leading to the development and recurrence of BPPV, the most common peripheral vestibular disorder, is very important for treatment and follow-up.
A limitation of this study was the retrospective design. However, the results of this study demonstrated low vitamin D levels in patients with posterior canal BPPV, which was consistent with the findings of some other studies in the literature. In patients with BPPV with vitamin D deficiency, the recurrence and severity of the disease can be reduced with the use of drugs containing vitamin D. Nevertheless, there is a need for further prospective studies with more patients to clarify this subject.
Footnotes
Authors’ Note
Concept—H.C.İ, C.M..; Design—H.C.İ., C.M.; Supervision—H.C.İ.; Resources—H.C.İ., C.M.; Materials—H.C.İ., C.M.; Data Collection and/or Processing—H.C.İ., C.M.; Analysis and/or Interpretation—H.C.İ., C.M., Z.B.E.; Literature Search—H.C.İ., C.M., Z.B.E.; Writing Manuscript—H.C.İ., C.M., Z.B.E.; Critical Review—H.C.İ., C.M., Z.B.E. Erzincan Binali Yıldırım University Ethical committee 12.02.2019(33216249-604.01.02/E.9068).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.