
Abstract
Arytenoid edema is not a well-described complication of thyroplasty. We report a case of exuberant arytenoid edema following thyroplasty in a 33-year-old female. The diagnosis was made post-operative day 1, the patient was immediately started on a 6-day course of methylprednisone with voice rest. The arytenoid edema completely resolved within 1 week.
Significance Statement
This case report demonstrates a case of exuberant arytenoid edema following thyroplasty. This is not a known complication of thyroplasty and there are currently no treatment guidelines for this. We successfully treated this edema in the clinic by giving a short steroid dose of Medrol, with complete resolution of the arytenoid edema.
Laryngoscopic Clinic
A 33-year-old female presented to the clinic with a chief complaint of dysphonia. The patient had a history of seasonal allergies, subglottic insufficiency, endoscopic sinus surgery, and Nissen fundoplication. She also had a history of bilateral vocal fold pseudocysts that had been previously removed as well as Amniofix injection (MiMedx, Marietta, Georgia) to both true vocal folds, mini micro flap, and mass excision with dexamethasone injection and bilateral blue laser vaporization of vessels. She described her residual dysphonia as airiness when singing and sometimes when speaking, strained voice, and voice fatigue. The patient was a classical singer (Opera and musical theater) and a voice and piano teacher. She had undergone voice therapy without significant improvement. She denied dysphagia, odynophagia, throat pain, and otalgia.
Strobovideolaryngoscopy showed incomplete glottic closure, evidence of amniofix collection on the left true vocal folds with minimal contact on the right true vocal fold at the site of mass excision, R VF paresis, bilateral vocal fold pseudocysts, and scar, right vocal fold ectasia, and glottic insufficiency (Figure 1). The risks and benefits of type I thyroplasty were discussed with the patient, she was agreeable with the plan and elected to perform the procedure. Preoperative laryngeal examination with glottic insufficiency.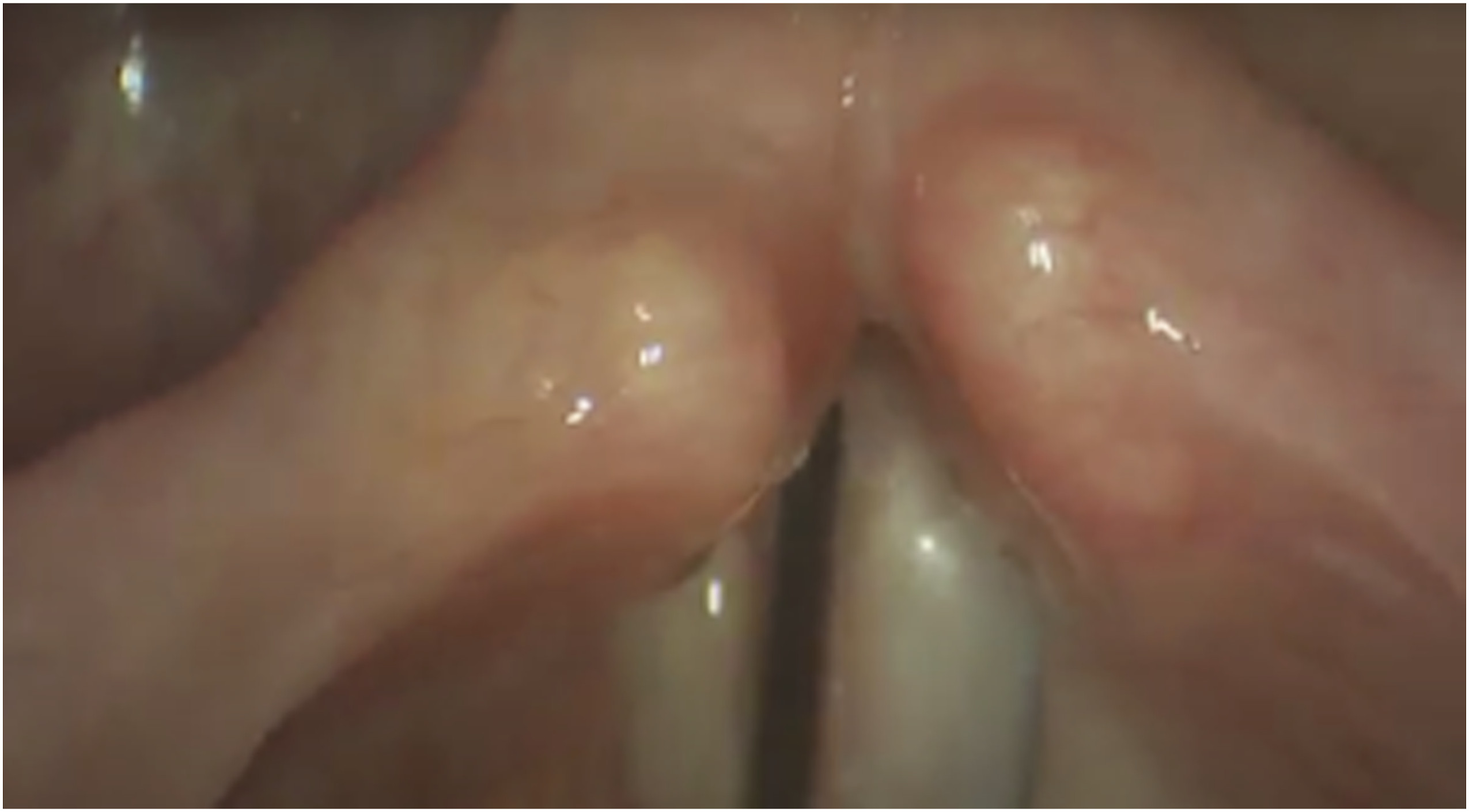
The patient underwent right thyroplasty through a 5-mm circular thyrotomy, the internal perichondrium was not violated. Only 3 cm of Gore-Tex were implanted and—improvement was excellent. Flexible laryngoscopy was performed to ensure proper positioning of the Gore-Tex implant. There was no evidence of malfunction, hemorrhage, or edema.
The patient was seen 1 day postoperatively. Her strobovideolaryngoscopy showed substantial improvement. However, the right arytenoid region was noted to be edematous and erythematous. (Figure 2). Post-operative day 1: hemorrhagic and polypoidal edema of the right arytenoids.
A 6-day steroid prescription for methylprednisone (Medrol Dose Pak, Pfizer, New York City, New York) 4 mg tablets was given and voice rest was prescribed.
Strobovideolaryngoscopy 1 week later showed that the right arytenoid edema had resolved completely. (Figure 3) Post-operative day 7: complete resolution of the right arytenoid edema.
Discussion
Reported complications of type 1 thyroplasty include infection, hemorrhage, airway obstruction, prosthesis extrusion, and vocal fold edema/hematoma.1,2 Arytenoid edema is a well-described complication of radiotherapy treatment of vocal fold and other head and neck cancers.3,4 Arytenoid edema also can be caused by infection, surgical trauma, nasogastric tube, and gastroesophageal reflux.5-8 Although uncommon, arytenoid edema after thyroplasty occurs.9,10 Intravenous administration of a single shot of prednisone preoperatively during type I thyroplasty was previously shown to reduce the occurrence of post-operative arytenoid edema. 10 However, the post-operative management of arytenoid edema after thyroplasty has not been addressed widely in the literature.
Although arytenoid edema is not a common complication of thyroplasty, this condition may result in hoarseness, dyspnea, dysphagia, and reduced quality of life with delayed improvement in voice outcomes. Several treatment options have been described in the literature for the treatment of arytenoid edema post radiation therapy. They include antibiotics and/or steroids, 11 arytenoid resection 12 using monopolar microelectrodes and radiofrequency, 5 erbium laser, 13 and transoral CO2 laser. 14 It is important to consider steroid intolerance and rule out diabetes or other metabolic disorders before steroid administration. In this case, we treated the arytenoid edema conservatively. We cannot say with certainty whether the steroids were causally related to the rapid recovery, and further investigation is encouraged.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.