
Abstract
Laryngeal tuberculosis is the most frequent granulomatous disease of the larynx and it is prone to be diagnosed as cancer. COVID-19 pandemic caused considerable disruption in tuberculosis service provisions both in the primary care and hospital settings. This report describes a rare case of life-threatening stridor in a patient who presented with an ulceroproliferative laryngeal mass later confirmed as laryngeal tuberculosis. Urgent tracheostomy was performed. The patient’s sputum and the computed tomography of the chest revealed a pulmonary, as well as laryngeal tuberculosis. The patient was commenced on a 24 week course of anti-tuberculous treatment which was interrupted because of a mild course of hospital-acquired coronavirus infection. 3 months after initial treatment for tuberculosis, his sputum cultures became negative. Flexible laryngoscopy was performed at our department 4 months after commencement of treatment, demonstrating complete regression of the lesion and symmetrical laryngeal mobility, hence the patient was successfully decannulated and discharged to be followed up to his community hospital. In the time of COVID-19 pandemic, we should never underestimate other severe infectious diseases.
Introduction
Laryngeal tuberculosis is the most frequent granulomatous disease of the larynx and represents 1–2% of extrapulmonary TB cases. 1 This disease is a great mimicker and diagnostic chameleon, so it is prone to be diagnosed as cancer. 2 The pathologic characteristic of tuberculosis is formation of caseating granulomas, structures developed by the host to eliminate the bacteria, and restrain the infection. 3 Progressive granulomatous inflammation of tissue presenting as proliferative mass may mimic laryngeal cancer.
The most frequent sites of laryngeal involvement are true vocal cords, false vocal cords, epiglottis, and posterior commisure. Still, the disease can affect any laryngeal subsite with transglottic extension. 4 Avoiding or delaying medical care due to COVID-19 pandemics is increasing complications and mortality associated with both chronic and acute health conditions. 5 This report describes a rare case of life-threatening stridor in a patient who presented with an ulceroproliferative laryngeal mass later confirmed as laryngeal tuberculosis.
Case Report
A 44-year-old male visited otorhinolaryngology emergency room on account of dyspnea, hoarseness, and significant weight loss for over 12 months. He had a history of smoking two packs of cigarettes per day for 30 years (since the age of 14) and everyday alcohol abuse for 25 years.
The patient was afebrile, dyspneic and looked cachectic. He wasn’t vaccinated against SARS Co-2 virus. Rapid antigen test was immediately performed and the patient tested negative for coronavirus. Oxygen saturations were 92% breathing room air.
Indirect laryngoscopy showed transglottic ulceroproliferative mass occupying the right hemilarynx with right vocal cord fixation, laryngeal edema, and narrowed airway. Consequently, laryngeal malignancy was initially suspected.
In the emergency setting, contrast-enhanced computed tomography (CT) of the neck was performed and it revealed ulceroproliferative laryngeal mass with airway narrowing (Figure 1A). (A) Contrast-enhanced computed tomography image of the neck reveals ulceroproliferative laryngeal mass (arrows) with airway narrowing. (B) Antero-posterior chest radiography shows mixed pattern opacity over bilateral lung fields and multiple cavitations over both lungs with tracheostomy cannula placed. (C) CT scan of the chest shows formation of central cavities in both lungs with diffuse interstitial nodular alterations.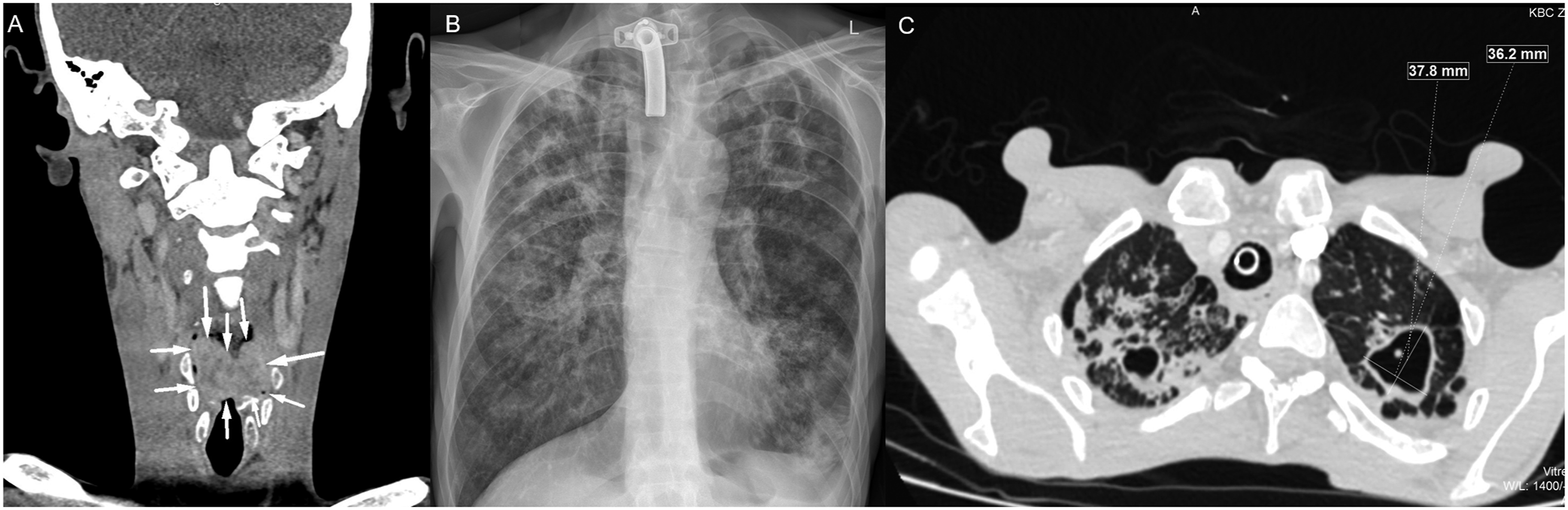
Just after receiving CT scan, the patient deteriorated, developing stridor, presented with notable suprasternal, intercostal and subcostal retractions. Hence, we performed awake surgical tracheotomy in the operating room under local anesthesia with 20 mL of lidocaine (40 mg/2 mL). After tracheotomy was performed, a tracheostomy cannula (9.0 mm) was placed. Intraoperatively and postoperatively the patient was stable respiratorily.
Blood tests revealed a raised C-reactive protein (113.8 mg/L), anaemia (Er 3.50 × 1012/L, Hgb 9.9 g/dL, HCT .301 L/L, MCHC 329 g/L), albuminaemia (26 g/L), a normal white cell count (5.9 × 109/L) with mild lymphopenia (1.2 × 109/L), and an elevated level of fibrinogen (4.2 g/L). Additional pertinent laboratory analysis included negative HIV, HBV and HCV serology testing.
Difficult intubation was predicted from the first assessment, and it was therefore decided that sample tissue for biopsy would be taken in indirect laryngoscopy.
Chest radiography revealed mixed pattern opacity over bilateral lung fields and multiple cavitations over both lungs, so we considered the possibility of tuberculosis (Figure 1B) and the sputum samples were taken.
In keeping with guidelines for management of suspected tuberculosis, the patient was admitted to an isolated side room until sputum smear status had been established.
An additional high resolution CT scan of the chest demonstrated formation of central cavities in both lungs with diffuse interstitial nodular alterations. (Figure 1C).
Four days after the initial presentation, sputum samples were found to be positive for Mycobacterium tuberculosis, so the patient was discharged from our department and admitted to a department for tuberculosis of the Special Hospital for Lung Diseases. The patient commenced with 24 week of isoniazid, rifampicin, pyrazinamide, ethambutol, and vitamin B6 antituberculotic treatment.
Laryngeal tuberculosis was confirmed on biopsy of the larynx.
Histopathological examination revealed granulomatous inflammation without signs of laryngeal malignancy (Figure 2A) and intracellular acid-fast bacilli were detected (Figure 2B). (A) Laryngeal tissue (hematoxylin-eosin staining) with granulomatous inflammation without signs of malignancy. (B) Granuloma with a Langhans type of giant cell in the center. Red stained Mycobacterium tuberculosis in Ziehl–Neelsen acid fast stain.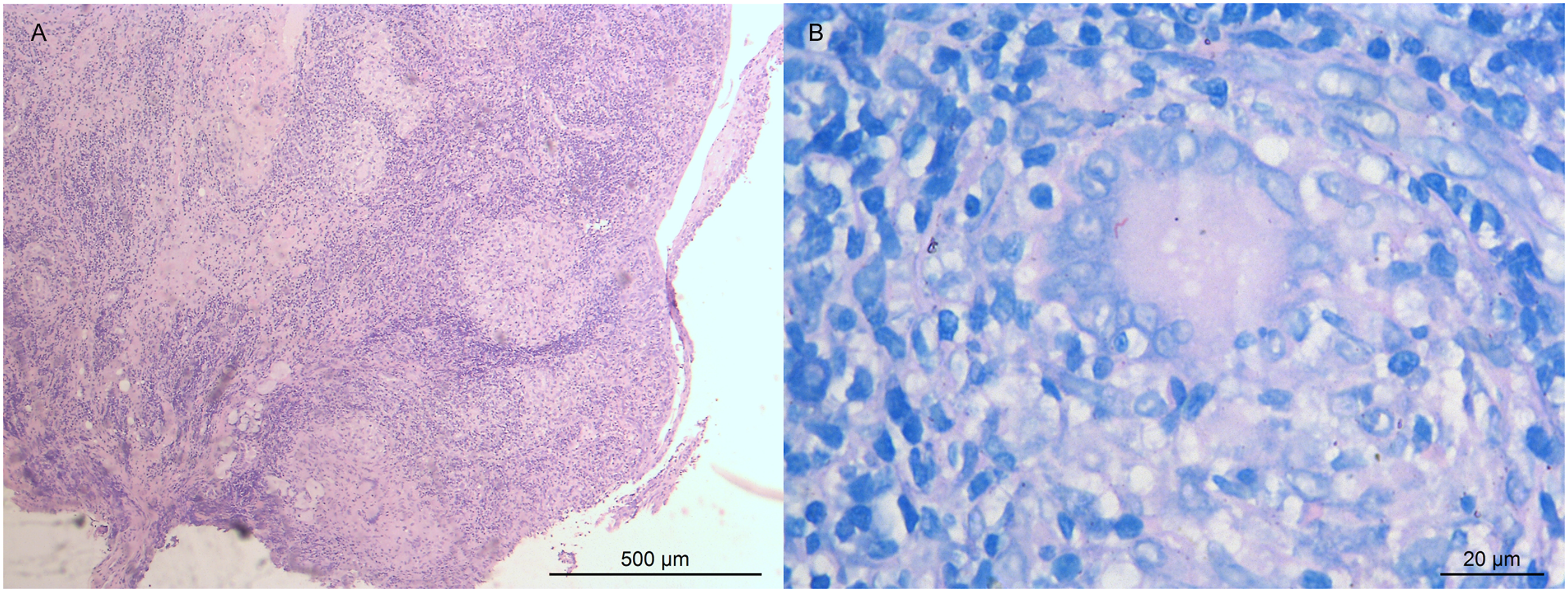
Two months later, the patient’s cough worsened, and he was tested positive for SARS-CoV-2 virus. After two weeks of symptomatic treatment, he tested negative, and then he was readmitted to a Special Hospital for Lung Diseases. Three months after initial treatment for tuberculosis, his sputum cultures became negative. Flexible laryngoscopy was performed at our department four months after commencement of treatment, demonstrating complete regression of the lesion and symmetrical laryngeal mobility, hence the patient was successfully decannulated and discharged to be followed up to his community health clinic.
Discussion
This case demonstrates laryngeal tuberculosis (LTB) and an obstruction of the airway to such an extent that tracheostomy had to be undertaken. The main symptoms presented by patients are cough and dysphonia, and the true vocal folds are the most frequently affected site. In rare cases, extensive nodular lesions and laryngeal edema may cause life threatening airway narrowing. 6
Laryngeal tuberculosis and malignancy share similar clinical features. 7 In addition, these two medical conditions have same local symptoms such as cough, hoarseness, dysphagia, odynophagia, hemoptysis, and rarely, stridor. Notably, smoking habits, alcohol consumption, and significant body weight loss may often raise the suspicion of malignancy.
Smoking is the main risk factor for developing laryngeal malignancy, but it also appears to be associated with the development of more extensive LTB lesions. 8
In the study of Agarwal, a majority of the lesions were ulceroproliferative and hence mimicked malignancy. LTB was not considered in the clinical differential diagnosis owing to its rarity. 9
Zang’s study found that in LTB patients with extensive laryngeal lesions, ulcerative lesions were the most frequent, with a higher proportion of cases with simultaneous pulmonary tuberculosis and higher positive rates of microbiologically confirmed tuberculosis. The patients with ulcerative lesions were more likely to have detected acid-fast bacilli than exophytic lesions. The histopathologic features of LTB-related ulcerative lesions included fewer granulomas and more areas with caseous necrosis. Although the efficacy of anti-tuberculotic treatment was at high level, in clinical practice, Zang’s study revealed that if patients received inadequate or irregular anti-TB treatment, LTB often recurred, and its morphology often showed exophytic lesions. 10
Various studies showed that laryngeal tuberculosis and laryngeal carcinoma was hardly distinguishable even with laryngoscopy and image surveys.4,7,11 Besides presenting complaints and the patient features suggesting malignancy in patients of laryngeal TB, even the histology findings may mimic carcinoma due to epithelial hyperplasia. 12 Nevertheless, histopathological examination and tuberculosis cultures are still the gold standards for diagnosis. 13 Several cases of concomitant carcinoma and tuberculosis have been reported in the literature, so medical practitioners must also be aware that laryngeal cancer and tuberculosis may coexist. 14 Also, in view of tuberculosis and cancer, studies suggest that one disease could facilitate the other. 15 In our report, a pathological examination revealed no signs of laryngeal malignancy.
Appropriate combination of anti-TB drugs can often cure LTB infection. 16 Notable improvement of patient symptoms usually appears within weeks. Improvement of laryngeal appearances usually returns to normal within several months. 10 Swain’s study recommends that an anti-LTB chemotherapy treatment period can be extended to 12 months when LTB is accompanied by pulmonary TB. The treatment should include 2 months of intensive treatments (rifampin, isoniazid, pyrazinamide, and ethambutol) followed by a maintenance treatment of two or three drugs. 17
Jain’s study demonstrated that COVID-19 pandemic caused considerable disruption in tuberculosis service provisions both in the primary care and hospital settings. Isolation strategies and lockdown restrictions to prevent viral transmission impacted the delivery of all aspects of tuberculosis care. The study revealed that the delay in the treatment would deteriorate the course of tuberculosis. Also, these patients may develop coronavirus superinfection, which correlates with our report. 18
In the time of COVID-19 pandemic, we should never underestimate other severe infectious diseases, even in immunocompetent hosts. 19
Environmental control and personal protection are aspects that physicians could overlook when treating patients, 20 so we should always be aware of the environment and choose the most suitable place to perform an urgent tracheostomy or laryngoscopy. 6
As a conclusion, compromised airway due to laryngeal tuberculosis is a rare condition that may require urgent tracheostomy. However, it must always be remembered to include this disease in the differential diagnosis for patients presenting with hoarseness, dyspnea, and upper airway obstruction.
Footnotes
Declaration of conflicting interests
The manuscript has not been published previously, and is not under consideration for publication elsewhere. The submission of this manuscript has been approved by all authors and tacitly or explicitly by the responsible authorities where the work was carried out, and, if accepted, it will not be published elsewhere in the same form, in English or in any other language, including electronically without the written consent of the copyright-holder.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. Written consent is available for review by the Editor-in-Chief of this journal on request. All procedures performed in studies involving human participants were in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.