
Abstract
Acquired choanal atresia is a rare complication of pharyngeal surgical interventions. Here, we report the case of a 72-year-old woman who was treated in our institution for acquired choanal atresia after failed previous treatments. We have excised the obstructing fibrotic scar tissue and then reconstructed the area using a mucosal local flap and free radial forearm flap transfer. Choanal stenosis caused by abnormal granulation was identified in the months after surgery; however, this was treated with endoscopic dilatation and steroid injections in the outpatient setting. No restenosis was identified 1 year after the operation. Postoperative evaluation of speech was satisfactory. Free flap transfer could be an option for refractory choanal atresia, and endoscopic dilatation with local steroid injections may be an effective method to treat postoperative restenosis.
Introduction
Choanal atresia is hereditary in most cases, while acquired choanal atresia is extremely rare. 1 There are various treatment methods for this condition, but the use of free flaps has not been reported previously. Here, we report a case of acquired choanal atresia which reoccurred following multiple surgeries carried out in other institutions.
A 72-year-old woman patient who suffered from respiratory difficulty due to choanal atresia was referred to our clinic for surgical treatment. It was found out by the referring physician that the patient had developed choanal atresia due to a pharyngoplasty procedure she underwent for the treatment of snoring at 20 years old. The patient started having mild breathing difficulty at 63 years old and began seeing the referring doctor at 66 years old. She underwent reconstructive surgery for the soft palate with a buccal mucosa flap; however, this treatment was unsuccessful, and the patient was referred to our institution. On the initial examination, the nasopharyngeal fiberscope identified complete obstruction of the choana by fibrotic scar tissue (Figure 1). We have excised the fibrotic scar tissue to open a pathway between the nasal cavity and the pharynx. A mucosal flap from the posterior pharyngeal wall was created with the left side as the stem. Elevation of the flap was then carried out mainly from the right side, extending toward the epipharynx. The mucosal flap donor site was covered using a free radial forearm flap, and the side wall of the soft palate was reconstructed based on the jump method
2
for reconstruction following oropharyngeal cancer resection (Figure 2). Videofluoroscopic examination on postoperative day (POD) 8 revealed satisfactory swallowing function and the patient started to have meals on POD 9. Subsequently, the nasal airway which was implanted immediately after the operation was removed on POD 21. The patient was discharged on POD 29. Choanal stenosis caused by abnormal granulation tissue formation was identified 2, 3, and 4 months postoperatively, and endoscopic dilatation using a Foley catheter and steroid injection for the abnormal granulation were implemented each time. One year postoperatively, no restenosis was identified, and the patient’s prognosis was favorable. Conversational intelligibility (Taguchi method)
3
and speech articulation (100 syllables)
4
were used for speech evaluation before surgery and 4 months after surgery to evaluate vocal function. Although there were no changes found in conversational intelligibility before and after surgery, the patient’s speech articulation score improved from 70.3 before surgery to 82.3 after surgery. Postoperative examination revealed good velopharyngeal function with no nasal voice, consonant distortion from nasal exhale leakage, or nasal exhale leakage during blowing.

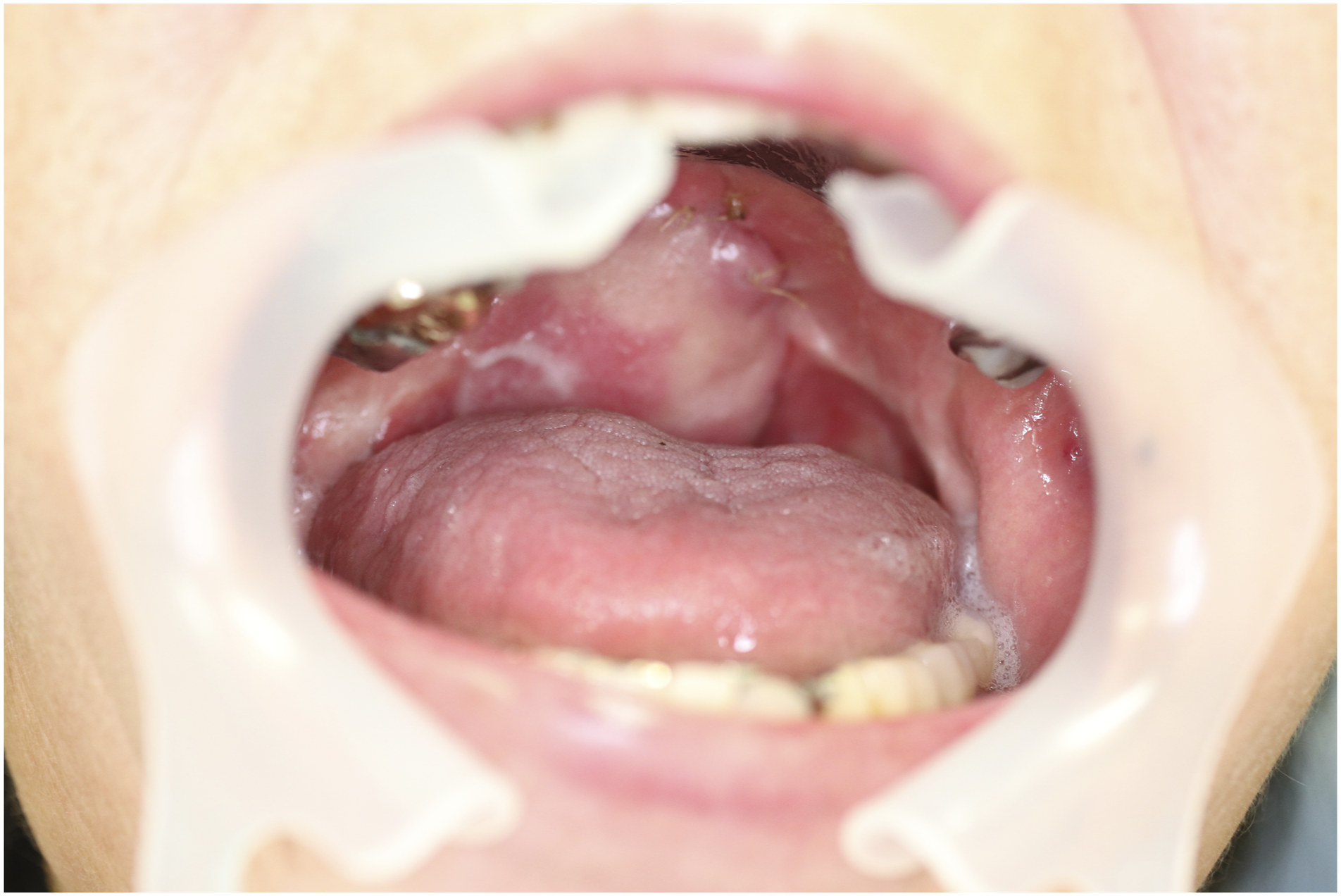
Nasopharyngeal fiberscope findings at the initial examination; choanal complete obstruction is visible.
We have excised the obstructing fibrotic scar tissue and then carried out reconstruction using a pharyngeal mucosal flap and free radial forearm flap transfer.
Discussion
Choanal atresia is a rare condition occurring in 1 out of 5000–8000 people, and acquired choanal atresia is even less common. 1 Surgery, radiation therapy, syphilis, diphtheria, and trauma can cause acquired choanal atresia, and related cicatricial stenosis is generally the underlying factor.5-7 The main symptoms are nasal congestion and rhinorrhea, with secretory otitis media, which can cause ear fullness and deafness, occurring as a complication in some cases. 7
Surgical approaches for this condition include the oral lid method, nasopharyngeal cavity method, trans-septal method, and trans-maxillary sinus method, with the oral lid and nasopharyngeal cavity methods being the most commonly used. 8 Postoperative restenosis and reclosure occur frequently. Although various methods for prevention of complications have been reported, there is no current consensus. Several materials are used as stents to prevent restenosis, but there is no established theory regarding the retention period.
Since lesion excision performed alone leads to additional scarring which results in postoperative restenosis and reclosure, using flaps as a replacement for the lesion area after excision may lead to more effective and satisfactory results. However, our case had suffered from reclosure after previous reconstruction by a local mucosal flap. We have also found out that there was not enough tissue around the lesion to completely reconstruct the area. We have therefore considered free flap transfer to provide sufficient tissue volume for wide-ranging replacement, and the thin free radial forearm flap was selected.
In addition to endoscopic dilatation for postoperative restenosis, 9 the use of steroid nasal drops to prevent granulation tissue growth has been reported. 10 This treatment is also considered effective for postoperative restenosis. In this case, endoscopic dilatation and steroidal injection for abnormal granulation were implemented thrice for the gradually progressing restenosis, which occurred after removing the nasal airway. The patient’s prognosis was favorable 1 year postoperatively.
This case suggests that free flap and endoscopic dilatation surgery combined with local steroid injections could be an effective treatment method for recurring choanal atresia.
Summary
We reported a case of acquired choanal atresia which recurred multiple times. Free flap transfer may be a treatment option for refractory choanal atresia. Balloon catheter endoscopic dilatation and local steroid injection may be effective for treating postoperative restenosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and material
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Ethical approval
Ethics approval from IRB is not required for a Case Report in my facility. Consent to participate. Written informed consent was obtained from the patient. Consent for publication. Consent for publication was obtained from the patient.