
Abstract

Significant Statement
The anterior compartment of the lower neck is considered as a safe region to approach the thyroid gland, larynx, trachea and esophagus. Incisions in the midline are preferred due to their remoteness from the carotid artery and the internal jugular vein (IJV). A common misconception is that neck devoid of superficial large vessels in the midline and formal bleeding does not pose a major risk at this region. We present an interesting anatomic variation of an arteriosus jugular arch in a cadaveric specimen.
Case Description
An arteriosus jugular arch of the neck was observed during the dissection of a 72-year-old Caucasian male formalin-embalmed cadaver, from Northern Greece. The cadaver was donated to the Department of Anatomy, Aristotle University of Thessaloniki. Lung cancer was documented as the cause of death.
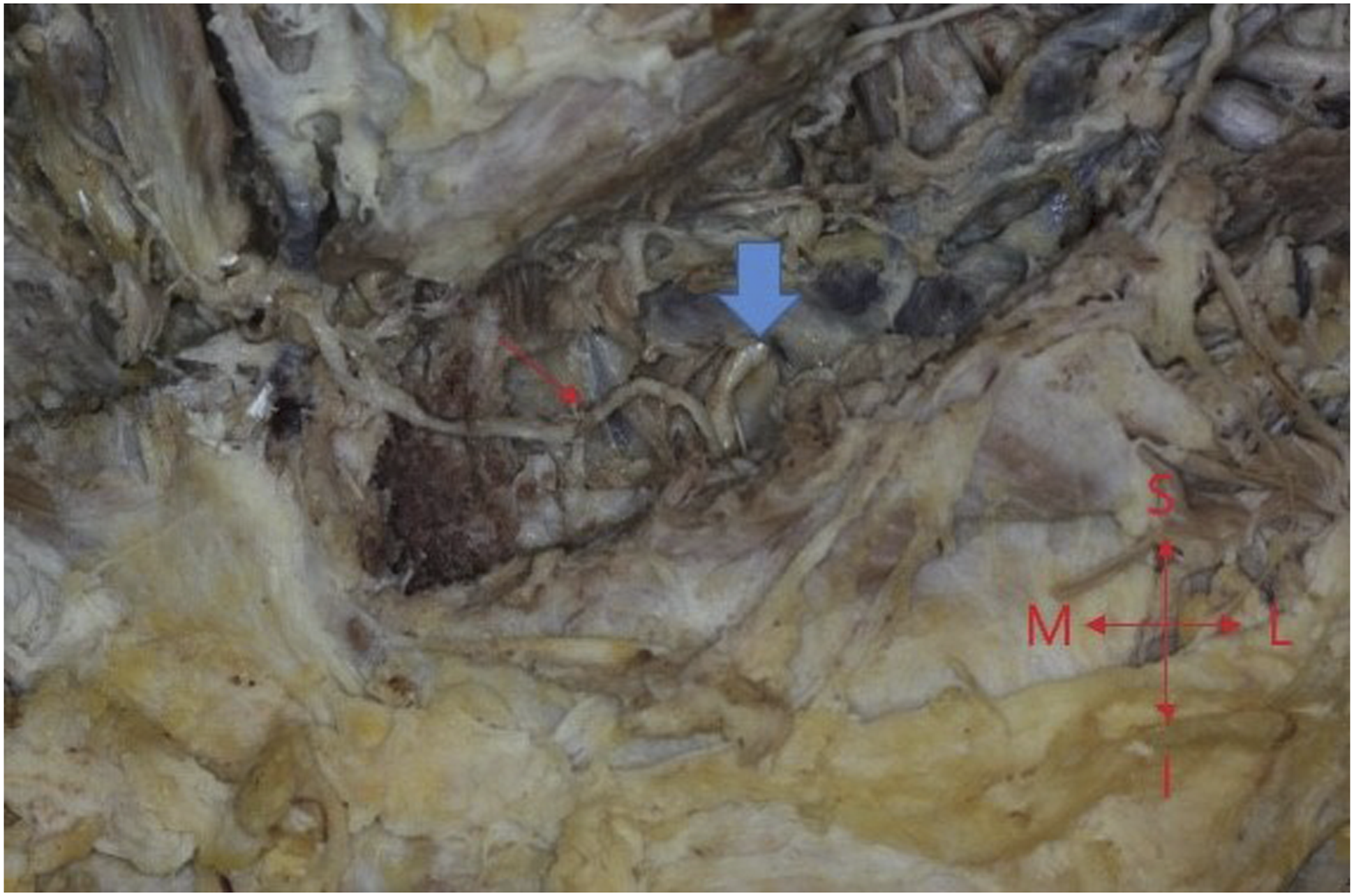
Dissection of the cadaver did not detect any gross pathology in the head and neck region. However, an interesting anatomic variation was observed in the central compartment of the neck. An arteriosus arch, the so-called arteriosus jugular arch was identified and dissected meticulously. That arch was formed by the contribution of 2 arterial branches. On the right side, an arterial stem of the thyrocervical trunk subdivided into the ipsilateral suprascapular artery and the right arterial segment of the arteriosus arch (Figure 1). On the left side, the arterial component of the arteriosus jugular arch was originated from the left internal thoracic artery (Figure 2). Both branches crossed horizontally the midline beneath the investing layer of the deep cervical fascia. The total length of the arch was 5 cm and the arterial diameter was .5 cm. Anterior jugular veins were observed and dissected, but no communication between them as it was occurred with the arteriosus arch was detected. To the best of our knowledge, this is a very rare anatomical variation and no other similar cases of arteriosus jugular arch have been mentioned in the relative literature. Right side of the arteriosus arch. SCM, Sternoclidomastoid muscle; purple arrow, Thyrocervical trunk; green arrow, Suprascapular artery; Blue arrow, Arteriosus arch; M, Medial; L, Lateral; S, Superior; I, Inferior. Left side of the arteriosus arch. blue arrow, Left internal thoracic artery; red arrow, Arteriosus arch; M, Medial; L, Lateral; S, Superior, I, Inferior.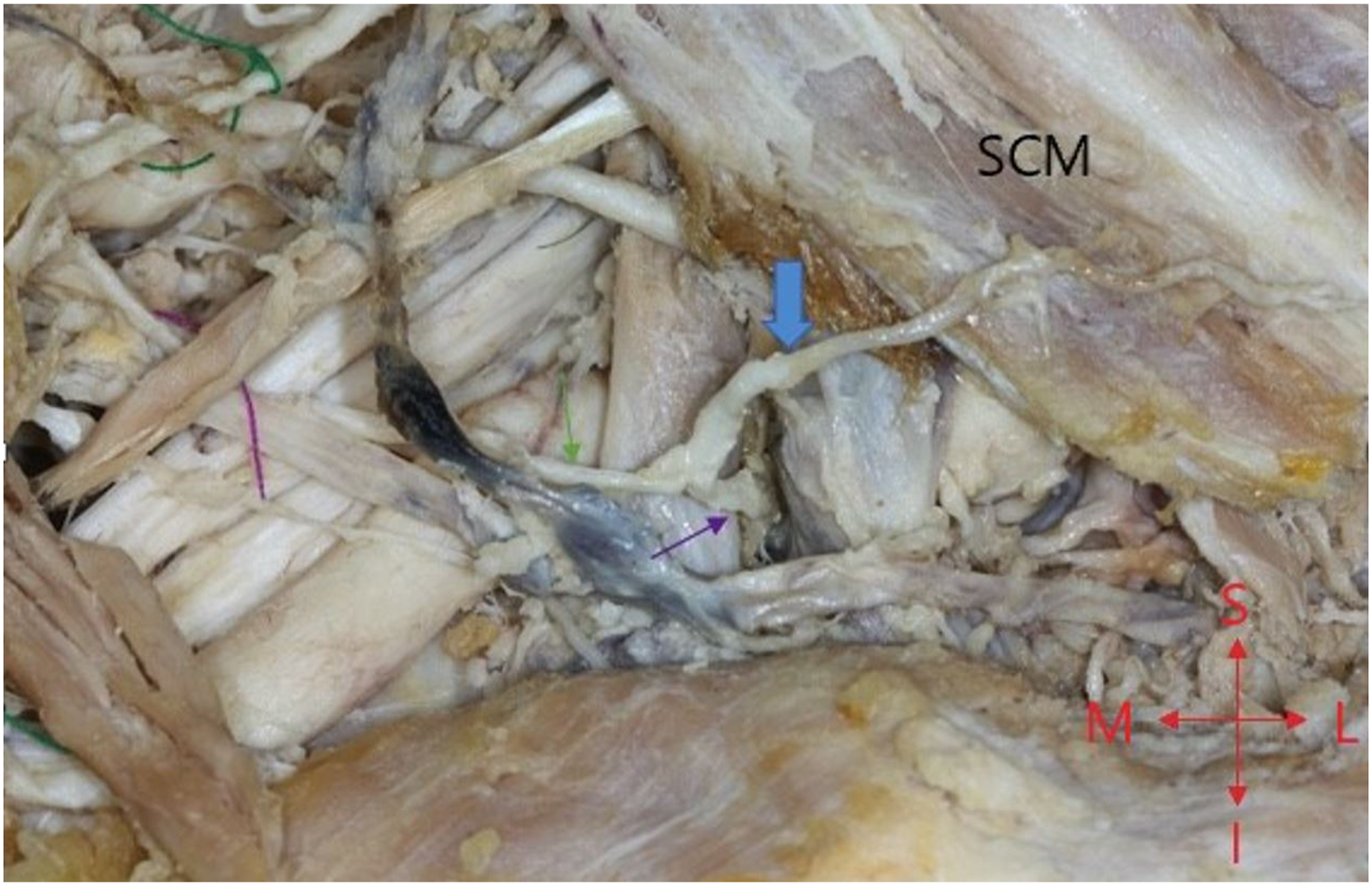
The presence of a jugular venous arch is well documented. 1 Most individuals have 2 anterior jugular veins with no valves. They originate as a confluence of small superficial veins in submandibular area and descend vertically in the midline, to end in the inferior path of the sternocleidomastoid muscle, medial to its anterior border. In the suprasternal area occasionally, a communication via a transverse vein known as the jugular venous arch may be present.1,2
Dissection of the central compartment of the lower neck is considered safe because it lacks major blood vessels. The cervical segment of common carotid arteries follows an oblique course upwards. The 2 common carotid arteries have no branches and are separated by the trachea. The vertebral arteries are beneath the deep cervical fascia and do not affect the operations in the central compartment of the neck. Ultimately, the thyrocervical trunk lies deep and lateral to the trachea.3,4 Therefore, surgeons only consider the anterior jugulars veins as the possible foci of bleeding.
However, there are multiple reports of anatomic arterial variations that may lead to lethal complications. An aberrant course of a common carotid artery just in front of trachea is a variation that has been described by many authors.5-7 Even though it is only reported in case reports, surgeons should be aware of this variation in order to prevent the hemorrhage. Careful palpation of the area of the dissection is enough to exclude it.
The presence of an arteriosus jugular arch makes the surgical approaches more challenging, especially in irradiated patients with extended tissue damage. Ligation of this transverse artery is imperative to avoid hemorrhage. Our morphometric measurements exhibited the risk of major bleeding in case of an accidental tearing. Knowledge of every possible variation like that will improve the surgical outcome and will help head and neck surgeons to explore the area with minimum blood loss.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.