
Abstract
Introduction
With the global COVID-19 pandemic, nasopharyngeal swabbing has become commonplace and can occasionally cause discomfort, tearing, and anxiety.
Objective
To evaluate whether using a neural distraction device during nasopharyngeal swabbing can mitigate patient discomfort.
Methods
Participants were randomized into nasal swab with vibration first (treatment-control or Tc) or nasal swab without vibration first (control-treatment or Ct). Then the swab was repeated with the opposite technique. The vibration device was used to stimulate the infraorbital nerve at the midpupillary line, while a nasopharyngeal swab was performed according to CDC protocol. After each swab, participants filled out a survey to assess pain, discomfort, and tearing. This procedure was replicated on the contralateral nostril for a total of 4 swabs and 4 surveys.
Results
Thirty-four subjects were included in the analysis. In the Ct group, there was a median 1.0-point decrease in pain with the use of vibration (95% CI [−1.8, −0.3]
Conclusion
Vibratory stimulation of the infraorbital nerve is safe and effectively reduced pain, discomfort, and tearing during nasopharyngeal swab. Vibration is a reasonable option to minimize patient discomfort during COVID-19 or other microbiological testing.
Introduction
Pain and discomfort have always been an important concern for patients undergoing clinical interventions and for the providers administering them. With the global COVID-19 pandemic, a historically uncomfortable intervention—nasopharyngeal swabbing for microbiologic testing—has become increasingly common. Nasopharyngeal swabbing (NPS) testing can cause pain, discomfort, tearing, and increased distress and anxiety. Unfortunately, alternate testing methods such as saliva testing and nasal, oral, and oropharyngeal swabs that may be more comfortable tend to be less accurate. 1,2 As long as nasopharyngeal swabbing remains the gold standard for COVID-19 testing, the discomfort and distress associated with this testing method may potentially discourage asymptomatic or mildly symptomatic patients from seeking testing, compromising the detection of COVID-19 cases. While no studies have documented NPS testing avoidance and attrition, this remains an important theoretical concern. 1,3 As such, it continues to be in clinicians’ best interest to make NPS testing as comfortable as possible for patients.
This study seeks to evaluate whether using a neural distraction device during nasopharyngeal swabbing can mitigate patient discomfort. Neural distraction involves the use of a tactile, non-nociceptive sensory stimulus simultaneously with a nociceptive stimulus to alleviate the pain experienced by the patient. Neural distraction is proposed to work according to the gate control theory of pain that was first postulated in a 1965 paper by Melzack and Wall. Gate control theory proposes that the simultaneous stimulation of slow-transmitting C fibers (pain transmission) and fast A-β fibers (pressure/vibration) will result in activation of an inhibitory interneuron by the A-β fibers. Activation of this inhibitory interneuron will close the pain “gate,” thereby interrupting nociceptive signals and reducing the perception of pain. 4 -6 This theory is the basis for the use of neural distraction devices such as a vibration anesthetic device, a device commonly used in painful procedures such as laser therapy, local anesthetic injections (including dental anesthetic), cosmetic filler injections, and Botulinum toxin injections in the face. While neural distraction has demonstrated efficacy in these areas, to the best of our knowledge there has not been any study investigating the use of neural distraction to stimulate the infraorbital nerve during NPS testing. 4,7 -10
Our hypothesis is that stimulation of the infraorbital nerve (V2) through cutaneous application of a vibrating device will alleviate pain, discomfort, and tearing that may be experienced with nasopharyngeal swab testing. If this hypothesis is correct, the use of neural distraction may be applied to minimize pain and discomfort and maximize patient experience during important microbiological testing for COVID-19 and other viruses.
Methods
This study was conducted under approval from Thomas Jefferson University’s Institutional Review Board (IRB# 21D.260). Volunteer participants were recruited from the Jefferson Otolaryngology department and clinical offices. Exclusion criteria included: those under the age of 18, non-English speakers, those unable to provide informed consent, and any participants with a medical history of neuropathy or a neuromuscular disorder that could alter the perception of pain (complex regional pain syndrome, fibromyalgia, etc.). Patients were further excluded if anatomic abnormalities, including a grossly deviated septum, septal spurs, ipsilateral turbinate hypertrophy, or other anatomic cause of turbinate hypertrophy, were identified on anterior rhinoscopy performed by otolaryngology resident physicians.
An outline for the study design is shown in Figure 1
Study design and randomization procedures. Image of vibration device used in the study and method of swab. The vibration device was used to stimulate the infraorbital nerve at the midpupillary line, approximately 1 cm below the infraorbital rim, while a minitip nasopharyngeal swabbing was performed by a trained otolaryngology physician in accordance published CDC swab protocol guidelines.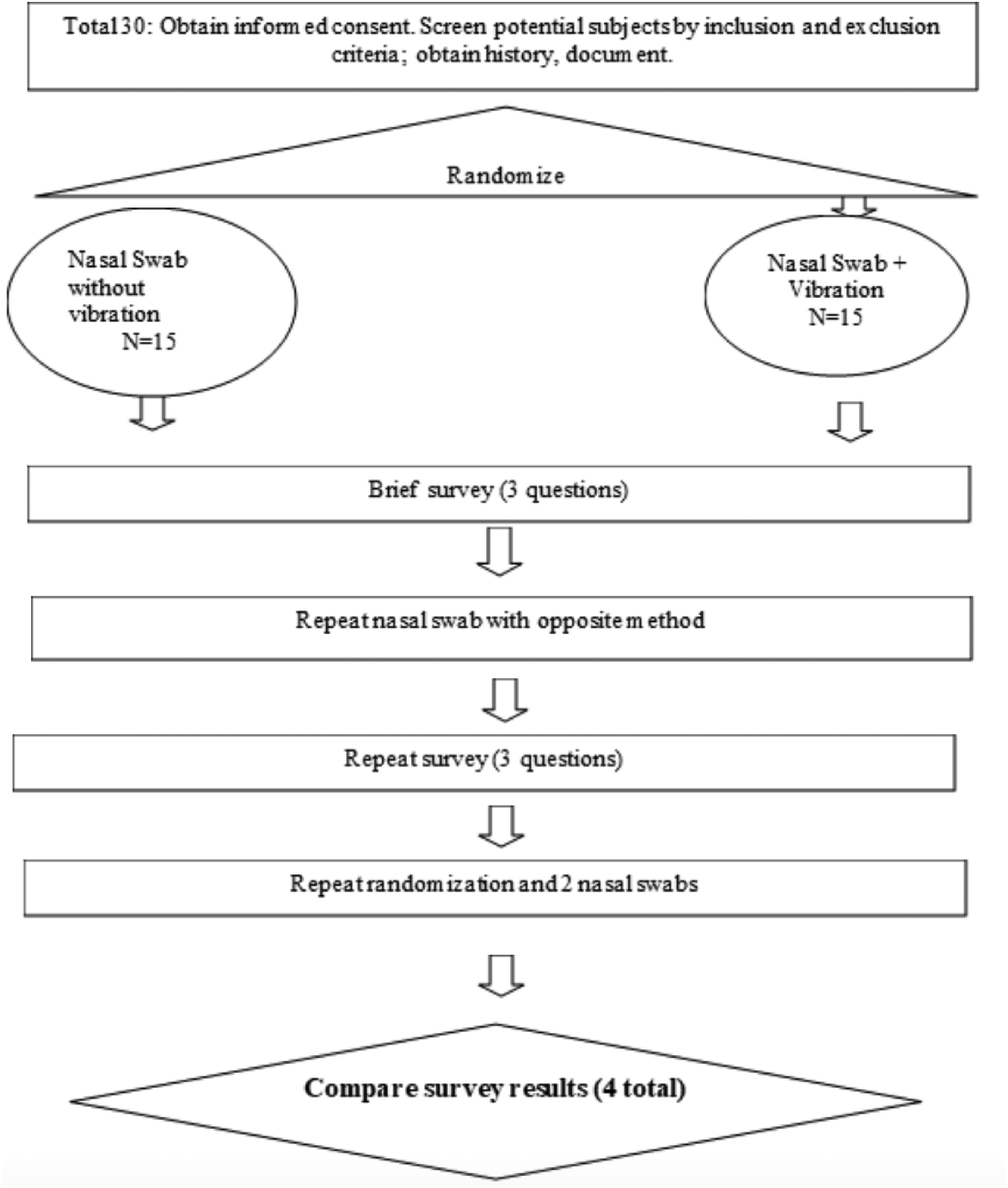

Statistical analysis
The median and interquartile range (IQR) of the pain/discomfort/tearing scores between both nostrils for each treatment type was calculated so that every patient had 2 data points (median score with vibration and median with no-vibration) each for pain, discomfort, and tearing. Data analysis was conducted using a Wilcoxon signed-rank test. Data were analyzed within each treatment group (Treatment-c and Control-t) to evaluate whether each treatment group experienced a significant change; data from both Treatment-c and Control-t were then pooled and analyzed together to assess total treatment response. Additionally, the change (delta, Δ) in pain, discomfort, and tearing between the control and vibration swabs was then calculated within each group. The delta of pain, discomfort, and tearing in treatment-control and control-treatment groups were then compared using a Mann–Whitney U test. P-values and 95% Confidence Intervals (CI) were reported. All statistical analyses were performed using GraphPad Prism 8 with an alpha level of significance of 0.05.
Results
Change in pain, discomfort, and tearing between groups.
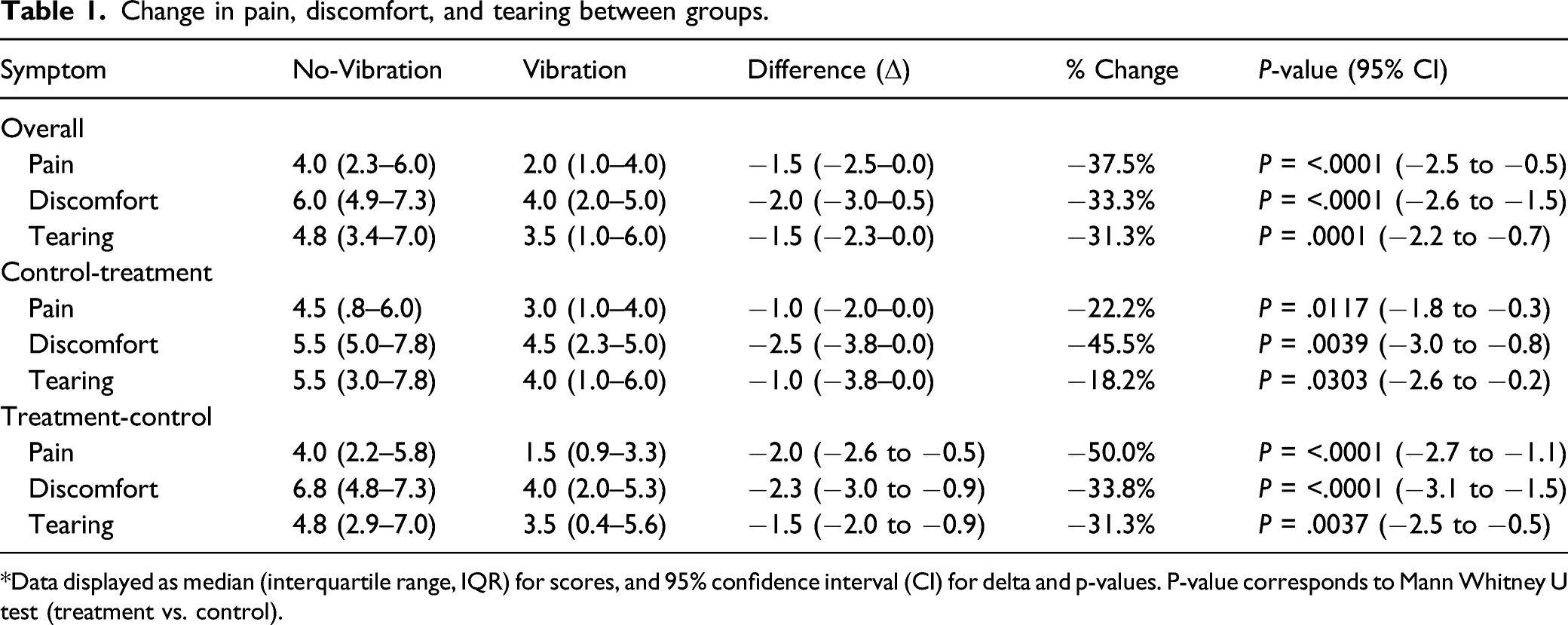
*Data displayed as median (interquartile range, IQR) for scores, and 95% confidence interval (CI) for delta and p-values. P-value corresponds to Mann Whitney U test (treatment vs. control).
Overall
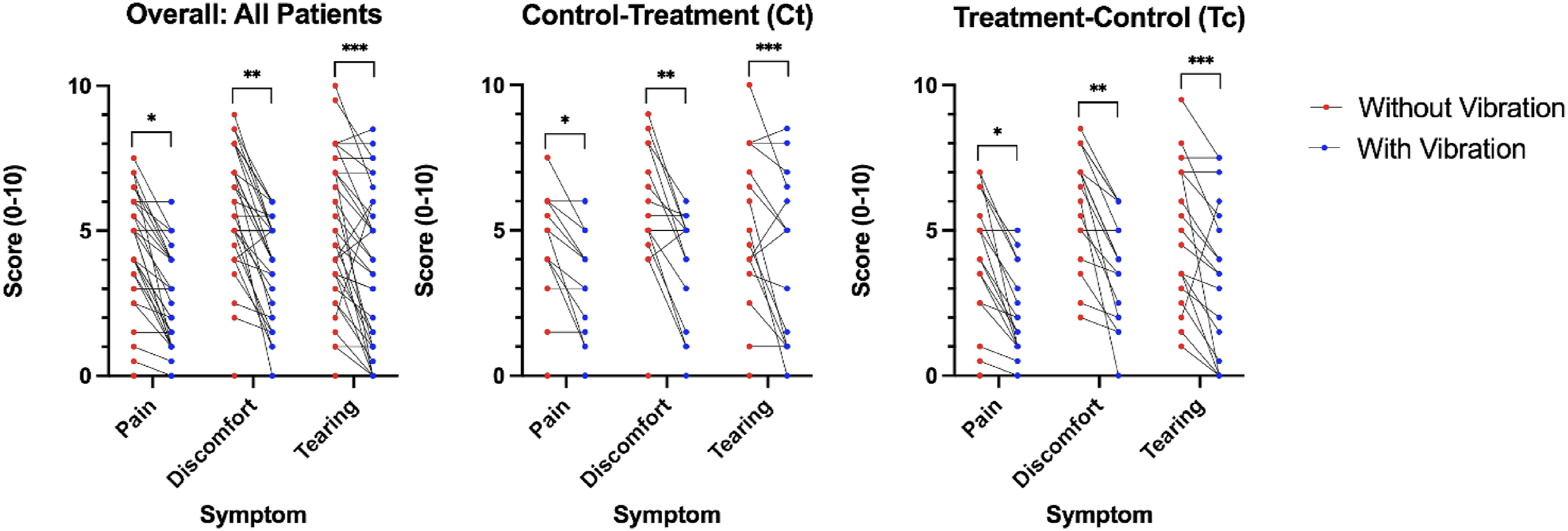
Summary analysis containing all data points from both Control-t and Treatment-c groups revealed the median (IQR) pain score without vibration was 4.0 (2.3–6.0) and 2.0 (1.0–4.0) with vibration (median decrease of 1.5, 95% CI [−2.5, −0.5]; P < .0001 Box and whisker plots showing the overall summary of pain, discomfort, and tearing scores with vibratory device and without for all patients, control-treatment, and treatment-control groups. Raw data points are shown, including median, interquartile range, and P-values corresponding to Mann–Whitney test. P-values are (A) *< .0001, **P < .0001, ***P = .0001 (B) *P = .0117, **P = .0039, ***P = .0303, and (C) *P < .0001, **P <.0001, ***P = .0037. Scatter plots showing pairwise comparison of pain, pain, discomfort, and tearing scores without vibratory device and without for all patients, control-treatment, and treatment-control groups. Raw data points are shown with a line connecting each participants’ score with and without vibration. P-values correspond to Mann–Whitney test and are the same values as in Figure 2.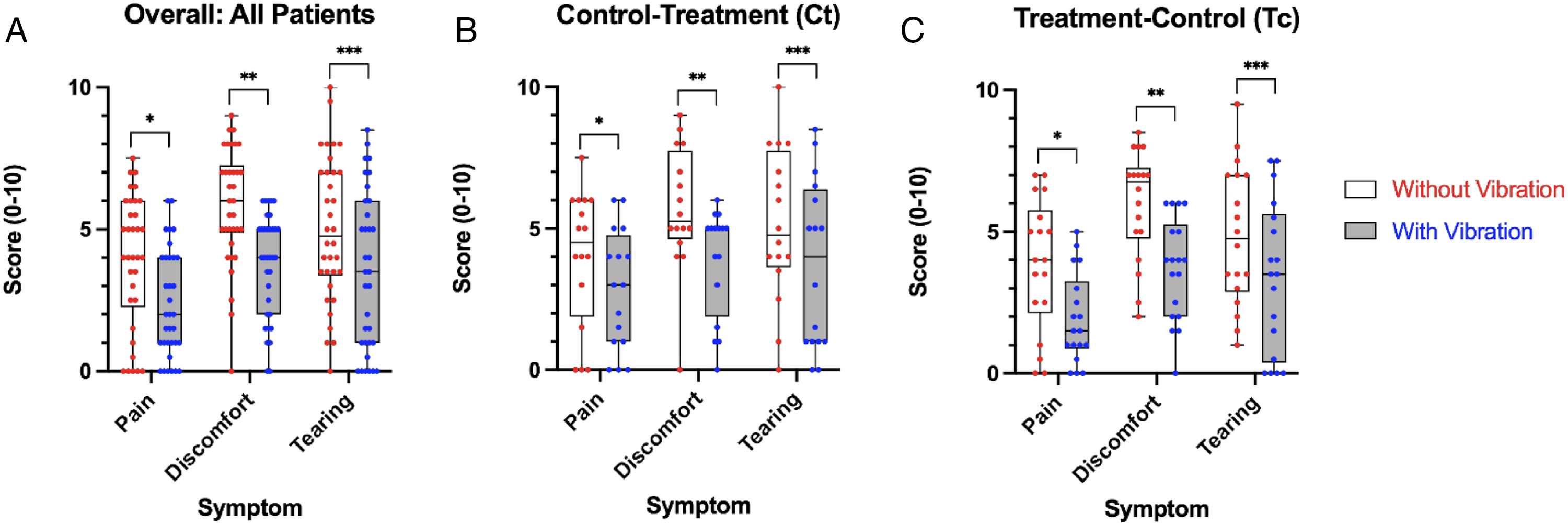
Pain
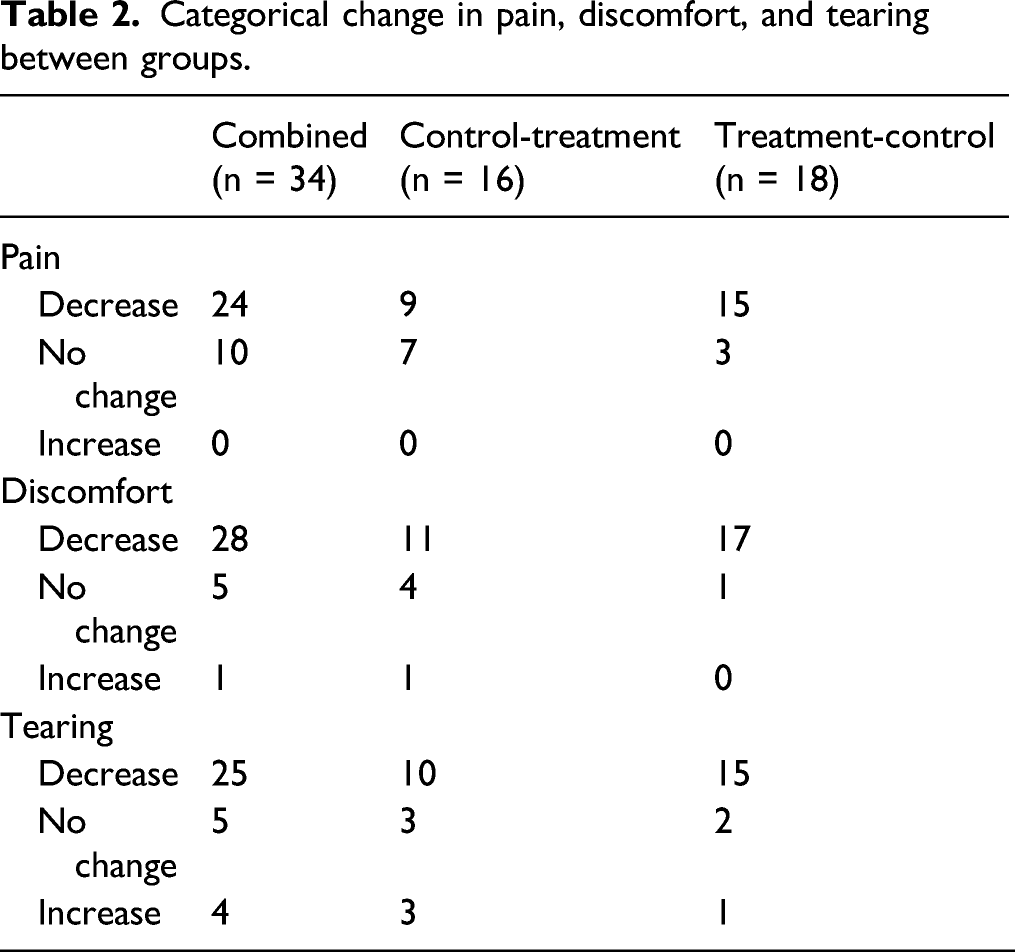
Categorical change in pain, discomfort, and tearing between groups.
Discomfort
The median (IQR) discomfort for the control-treatment group with no-vibration was 5.5 (5.0–7.8) and 4.5 (2.3–5.0) with vibration (median 1.0 decrease with vibration, 95% CI [−3.0, −0.8]; P = .0039). The median discomfort for the treatment-control group for no-vibration was 6.8 (4.8–7.3) and with vibration was 4.0 (2.0–5.3) (median 2.3-point decrease, 95% CI [−3.1, −1.5]; P < .0001). Thus, there was a significant decrease in discomfort experienced with the use of vibration during NPS in both groups. Of the 34 patients, 28 reported a decrease in discomfort with vibration (Ct = 11 and Tc = 17), 5 reported no change (Ct = 4 and Tc = 1), and 1 reported increased discomfort (Ct = 1 and Tc = 0) (Table 2
Tearing
In the control-treatment group, the median (IQR) tearing for the no-vibration swab was 5.5 (5.0–7.8), and 4.0 (1.0–6.0) with vibration (median 1.0-point decrease with vibration, 95% CI [−2.6, −0.2]; P = 0.0303). The median tearing in the treatment-control group for no-vibration and with vibration was 4.8 (2.9–7.0) and 3.5 (0.4–5.6) (median 1.5-point decrease, 95% CI [-2.5, −0.5]; P = 0.0037). There was a significant decrease in tearing experienced with the use of vibration during NPS in both groups. Of the 34 patients, 25 experienced a decrease in tearing with vibration (Ct = 10 and Tc = 15), 5 reported no change (Ct = 3 and Tc = 2), and 4 reported increased tearing (Ct = 3 and Tc = 1) (Table 2). There was no significant difference in delta tearing with vibration between the control-treatment and treatment-control groups (95% CI [−1.5, 1.5]; P = 0.6494).
Discussion
The rates of COVID-19 infection in the US may rise and fall in waves, but even when they are decreasing testing is necessary for many purposes, from hospital admission to infection exposure to international travel. Additionally, nasopharyngeal swabs will continue to be used to diagnose other upper and lower respiratory tract infections. Minimizing patients’ pain and discomfort during nasopharyngeal swab testing is important in the COVID-19 era to both maximize the patient experience and minimize any potential for testing avoidance, particularly in asymptomatic or mildly symptomatic individuals. 1,3 Previous studies have demonstrated the safety and efficacy of vibration as a neural distractor in reducing pain and anxiety during various dental and cosmetic procedures. 4,7 -9 Vibration has not been associated with any significant adverse effects, with minor reported adverse effects including a transient sensation of tingling, increased bruising (when vibration was used with an injection), and a headache in one patient in one study. 7 -9
Vibratory stimulation of areas corresponding to the 3 major branches of the trigeminal nerve (V1, V2, and V3) has been demonstrated to be effective in alleviating dental pain, as well as increasing the threshold for pain perception and pain tolerance. 9,10 Additionally, the use of the vibratory device has the advantage that it is easy to use and adds no additional time to specimen collection. It is also low cost (some studies have even used a $5 electric toothbrush as a vibration device), is small enough that it is easy to store in a drawer or cabinet in an office/patient room and has few associated adverse effects. 7 -10,14
Our results demonstrate that the use of a vibration device during nasopharyngeal swabbing significantly reduced patient reported pain, discomfort, and tearing in both groups, regardless of intervention order. We did not see any statistically significant difference in pain, discomfort, or tearing between the 2 treatment groups (Tc and Ct), suggesting that there was no difference in response to vibration based on treatment order alone, and no significant increase in sensitivity with subsequent swabbing. The effectiveness of vibration may be explained by stimulation of inhibitory interneurons in accordance with Melzack’s gate control theory of pain. 5,6 We saw the greatest reduction overall in pain (37.5%), but also saw significant reduction in discomfort (33.3%) and tearing (31.3%) in the pooled group.
While the individual patient’s experience may vary, 24 out of 34 patients reported decreased pain (with 10 reporting no change) and zero patients reported that the vibration increased their pain. While a few patients did report increased discomfort (n= 1) and tearing (n= 4) with vibration, they were distinctly in the minority (28 reported decreased discomfort, and 25 decreased tearing). As such, this suggests that vibration may be useful in clinical practice as the majority of patients experienced either a reduction in pain or no change in pain. Additionally, our data showed that of the patients who did not report improvement with vibration (either no change or increased symptoms, n= 12), many of these patients (n= 5) reported zero pain, discomfort, or tearing for the swab without vibration. In fact, all patients reporting zero pain, discomfort, or tearing for the no-vibration swab fell within this group of non-responders. This suggests that patients who do not find NPS testing particularly uncomfortable at baseline might be a large part of the population that does not benefit from vibratory neural distraction. Interestingly, previous research in the use of vibration with botulinum toxin injections has shown that even patients who did not feel that vibration reduced their pain during injections still preferred to use vibration with subsequent treatments, suggesting that their preference was influenced by factors other than pain reduction. 7 Although this study did not explore subjects’ preference for vibration with future NPS testing, it stands to reason that even patients who did not experience relief of pain/discomfort/tearing may still benefit from other effects of vibration, such as reduction of anxiety. 8
Although the differences in relief of pain, discomfort, and tearing were not significantly different between the 2 groups, there were more participants in the control-treatment (Ct) group, who received the swab without vibration first, that experienced no change in pain/discomfort/tearing or increases in these measures with vibration (Table 2). Additionally, there was a smaller degree of reduction of pain and tearing in the Control-t group, which received the first swab without vibration, than in the Treatment-c group (Ct vs Tc: 22.2% vs 50% decrease in pain and 18.2% vs 31.3% in tearing)
Limitations of this study include its relatively small sample size (n = 34; n = 16 and n = 18 per treatment group) and inability to have a control group due to the inherent variability of pain experiences between individuals. Additionally, subjects were unable to be blinded due to the nature of the intervention, leaving this study vulnerable to subject bias. The study population here is another potential source of subject bias, as all study participants were recruited from within Thomas Jefferson’s Otolaryngology office and may therefore have had previous knowledge of the use of the vibration device in other procedures such as in botulinum toxin injections. Additionally, our limited subject demographics may limit the generalizability of this study.
Future studies could include a larger sample size and a true placebo arm, perhaps using vibration to stimulate an unrelated area of the body during NPS testing. Previous studies have shown that using another form of non-vibration counter-stimulation in the same area, such as a switched off vibratory device, does not represent a true placebo as the sensation of pressure or even skin stroking may have enough of a counter-stimulatory effect to activate inhibitory interneurons and inhibit pain signaling. 7 Additionally, future studies should investigate the effects of vibration on anxiety associated with NPS testing; anxiety reduction has been demonstrated in the use of vibration in dental injections, and previous studies have suggested that even patients who were non-responders to vibration with injections preferred the use of vibration with subsequent injections. 7,8 If this method were also effective at reducing anxiety, this would lend it an additional advantage in clinical practice. Another further direction of study could be the use of vibration during NPS testing in pediatric populations, as vibration has previously been demonstrated to be effective at reducing venipuncture pain in older children. 14,15 Additionally, vibration as a neural distractor has potential for use in other common procedures within otolaryngology, such as fine needle aspiration or nasopharyngolaryngoscopy.
Conclusion
Despite its limitations, this study demonstrates that vibratory stimulation of the infraorbital nerve effectively reduces pain, discomfort, and tearing during nasopharyngeal swab testing. Vibration is safe and effective to use with little cost to providers. As long as the COVID-19 pandemic continues, so too will our need for accurate microbiological testing. Since NPS testing remains the gold standard in microbiologic testing for COVID-19, it is in clinicians’ best interest to take steps to make this testing as tolerable as possible for patients both to improve patient experience and maximize testing utilization.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.