
Abstract
Benign dendritic melanocytic proliferation is usually observed in the skin. We report an extremely rare case of a melanocytic lesion in the middle ear mucosa. Only 3 cases of melanocytic lesions in the middle ear have been reported. Our report is the only one that describes an adult with a melanocytic lesion in the middle ear that extended to the inner ear and nasopharyngeal mucosa. A 23-year-old female presented with profound sensory neural hearing loss and recurrent discharge from the right ear. Examination revealed a blue right tympanic membrane with a small perforation. Computed tomography scans and magnetic resonance imaging were performed. After surgical exploration and histopathological examination, the patient was found to have a benign melanocytic lesion in the right middle ear. Melanocytic lesions are commonly found in the skin. There are no previous reports have described adult patients with melanocytic lesions in the middle ear that extend to the inner ear and nasopharynx, which cause profound hearing loss with recurrent ear discharge. These patients require regular follow-up to assess the progression of the lesion and to watch for any malignant behavior.
Introduction
Melanocytes are pigment-producing cells that differentiate from melanoplasts, which originate from the neural crest during embryogenic development; melanocytes are distributed in the epidermis, hair follicles, mucosa, cochlea, iris, and meninges. 1 In the inner ear, melanocytes are distributed in the modiolus, stria vascularis, spiral ligament and cochlea. 2 Dendritic melanocytic proliferation lesions in the skin are a group of pigmented lesions characterized by the presence of immature melanocytes that migrate from the neural crest, and these lesions are classified as dermal melanocytosis, benign blue nevus and malignant blue nevus. The most common lesions are benign with a favorable clinical course. 3
Identification of pigmented lesions in the middle ear is extremely rare; to the best of our knowledge, only 3 cases have been reported: 2 adult patients with blue nevi confined to the middle ear without extension to the inner ear or the nasopharynx and 1 pediatric female patient with a pigmented middle ear lesion that extended to the inner ear and nasopharynx. 4 -6
We present a case of an adult female who presented with a middle ear pigmented lesion that extended to the inner ear and nasopharynx. Moreover, we provide a review of the literature.
Case report
A 23-year-old female with a history of recurrent right ear discharge and hearing loss started at 8 years of age, was referred to our department. More than 3 years ago, this patient had undergone 2 right tympanoplasties and 1 mastoidectomy. She did not notice any improvement after the surgeries. Upon otomicroscopic examination of the right ear, a blue tympanic membrane with small central perforation was observed. In the Tuning Fork examination, Rinne was positive on the left side and false negative on the right side, and Webber showed lateralization to the left. Nasopharyngeal examination identified mucosal blue pigmentation just above the opening of the Eustachian tube (Figure 1). Nasopharyngoscopic view revealing pigmented lesion above Eustachian tube opening (arrow).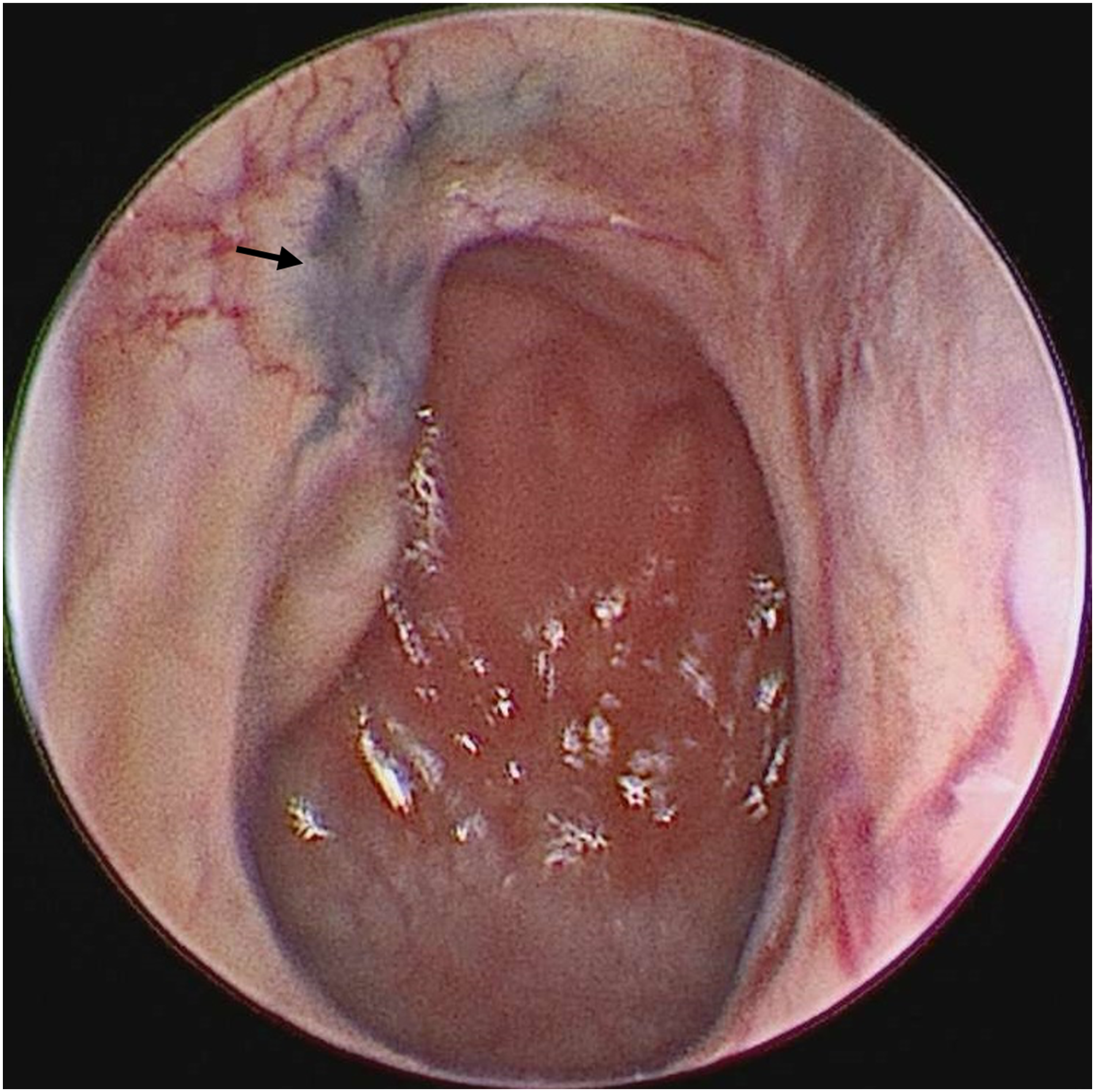
A pure tone audiometry test showed profound sensory neural hearing loss on the right side. A computed tomography (CT) scan showed complete opacification of the right mastoid with post-mastoidectomy changes but a normal tympanic cavity and normal inner ear without bony destruction (Figure 2A). Because the CT scan was not conclusive, magnetic resonance imaging (MRI) was performed and revealed a right tympanic cavity lesion that was enhanced on T1-weighted imaging (Figures 2B and 2C) but hypointense on T2-weighted imaging. (A) Computed tomography image showing complete opacification in the right mastoid with post mastoidectomy changes (Star), but normal tympanic cavity and inner ear. (B) Magnetic resonant image, axial cut (T1 weighted image) showing right tympanic cavity enhancing lesion (arrow). (C) Magnetic resonant image, coronal cut (T1 weighted image) showing right tympanic cavity enhancing lesion (arrow).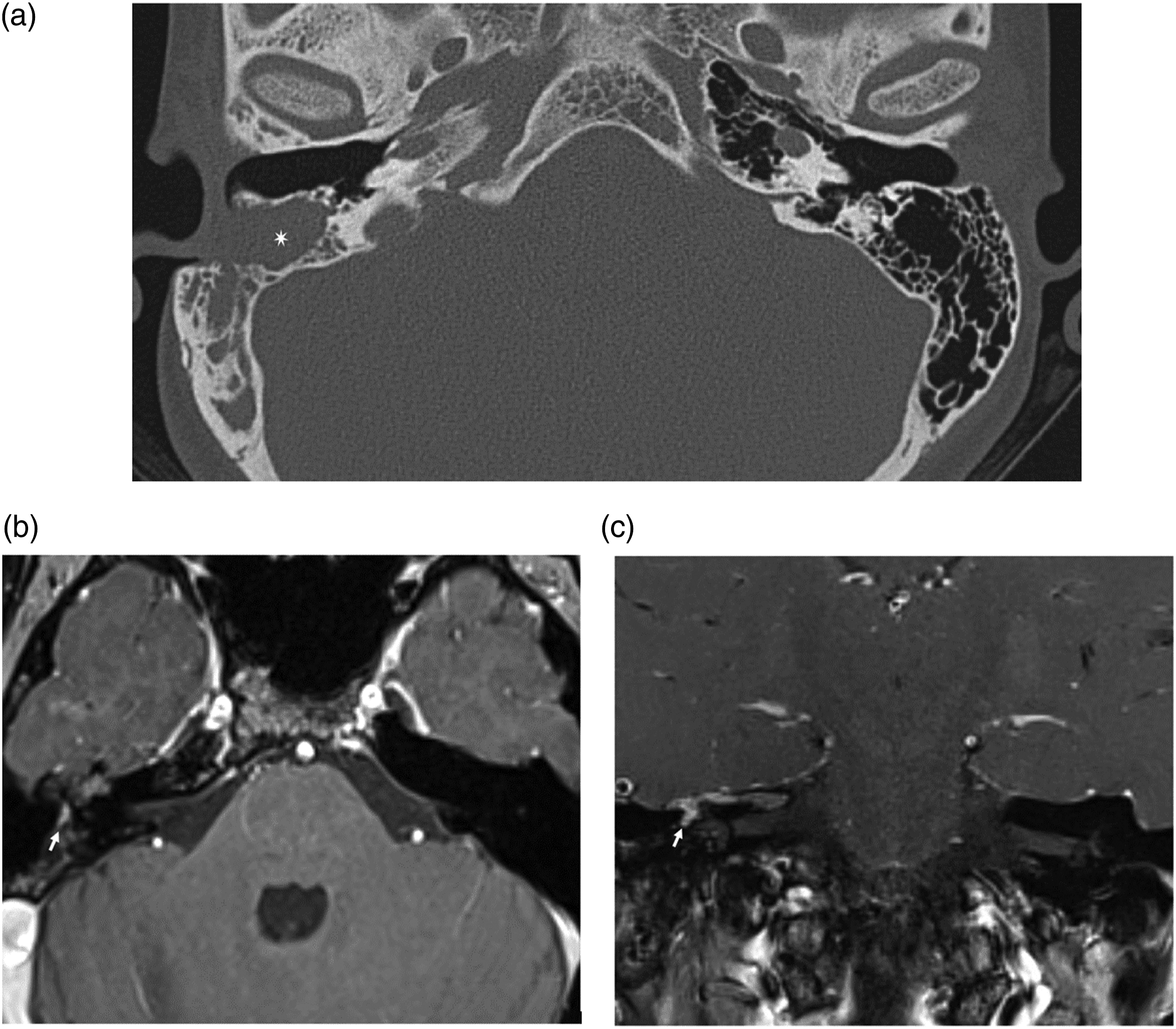
The patient underwent right revision canal wall down mastoidectomy and meatoplasty. Intraoperative findings showed multiple sites of pigmentation in the middle ear mucosa, at the promontory and extending through the round window, anteriorly to the eustachian tube. Sites of pigmentation were also observed in the mastoid, extending to the sigmoid sinus and the dura of the middle and posterior cranial fossa and surrounding the mastoid segment of the facial nerve (Figure 3). Due to diffuse extension of the lesion, it was impossible to remove it completely, so multiple biopsies were obtained, and canal wall down with good meatoplasty was performed to allow easy future clinical follow-up to monitor disease extension or transformation. Intraoperative images showing multiple pigmentations in the middle ear mucosa. (A) Mastoid part of facial nerve (star). Blue pigmentation around the mastoid part of the facial nerve (arrow). (B) Blue pigmentation over the skull base (arrow) and sigmoid sinus (star). (C) Eustachian tube (Star). Blue pigmentation anteriorly to the eustachian tube (arrow).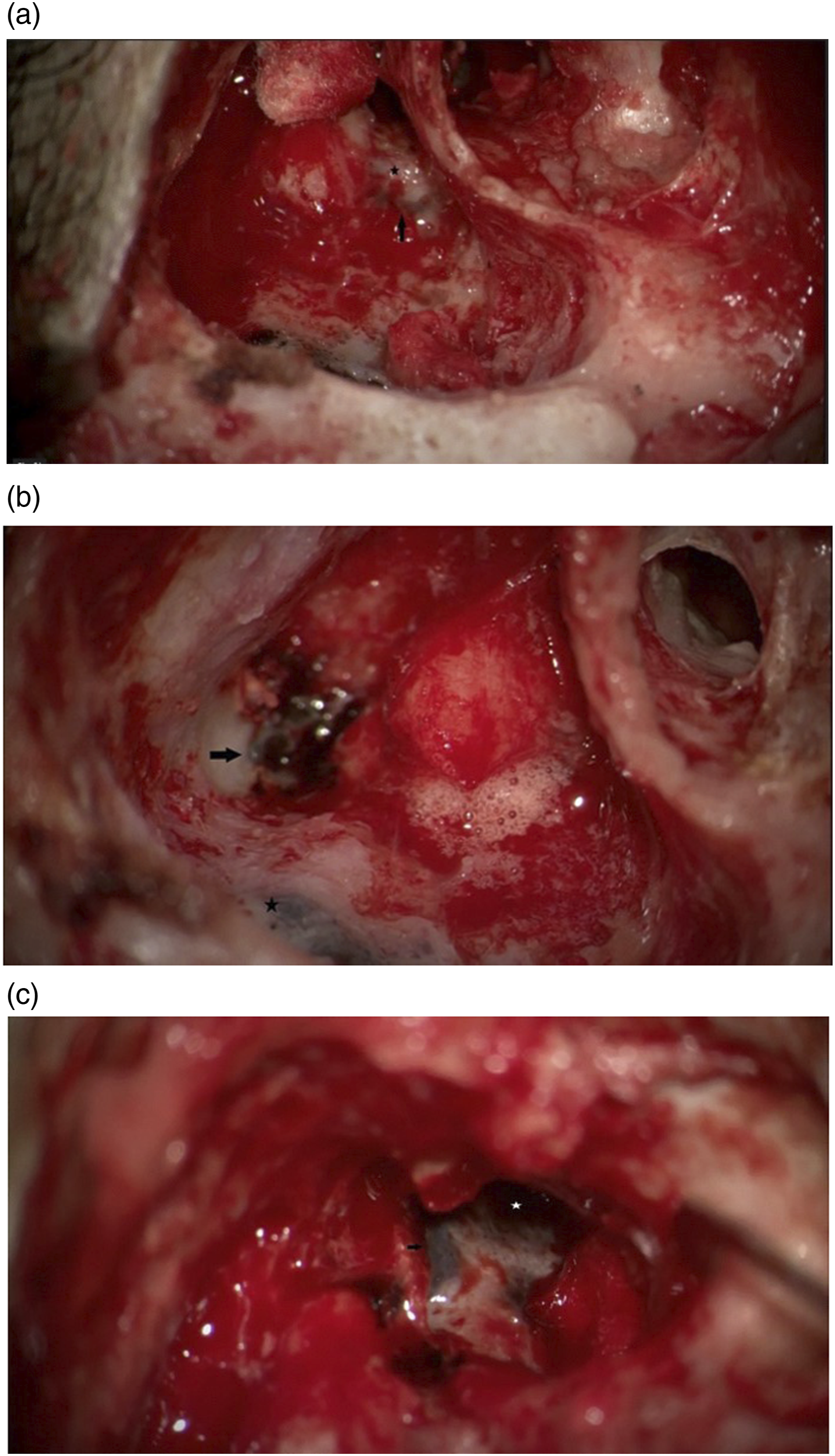
Histopathological examination revealed heavily pigmented submucosal melanocytes with fibrosis. Fontana-Masson staining was positive, consistent with melanin pigments. Melan-A immunostaining identified melanocytes (Figure 4). (A) Photomicrograph of the middle ear biopsy shows submucosal pigmented lesion, (hematoxylineosin, original magnification 40×). (B) Heavly pigmented microphages (Milanophages), (hematoxylin-eosin, original magnification 400×). (C) Melan A immunohistochemistry reveales scanty scattered milanocytes (400×).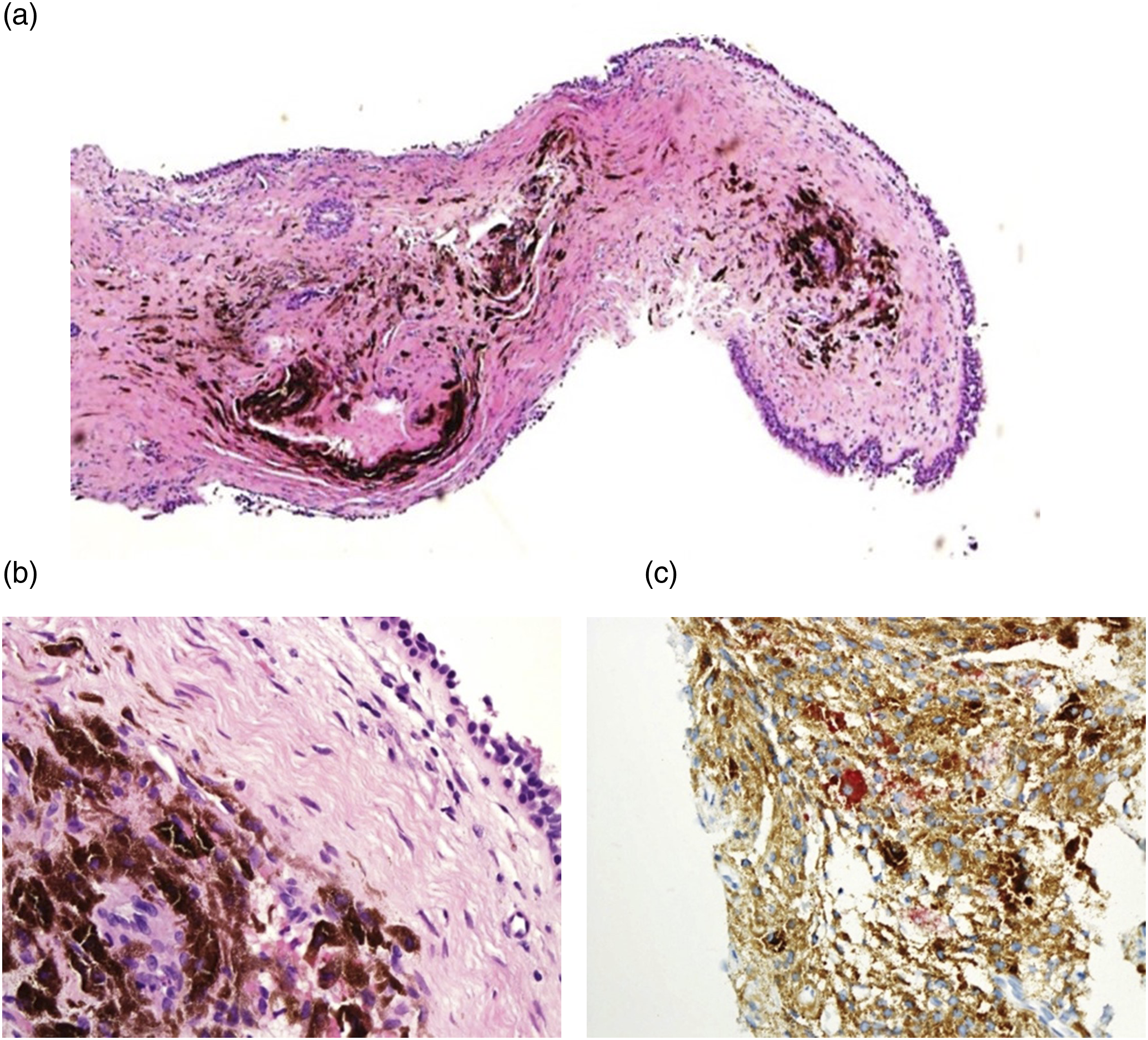
Postoperatively, the patient was followed up monthly for 5 months, and she had no clinical complaint and stable nasopharyngeal pigmentation.
Discussion
The presence of an extended melanocytic lesion in the middle ear of an adult patient with otological symptoms is worrisome. Nevertheless, the first differential diagnosis in this case was benign melanocytic lesions, as they are more common than malignant melanoma. However, we cannot overlook the possibility of malignancy. Malignant melanoma can arise from the middle ear mucosa and extend to the nasopharynx through the Eustachian tube or in the opposite direction. 7 Mucosal melanomas are very rare compared to cutaneous melanomas. They are found mostly in the sinonasal region and oral cavity, and extremely rare, they can be found in the pharynx and larynx. Middle ear melanomas are much less common, with an age of diagnosis ranging from 41 to 88 years. 7
In our case, the clinical and histological findings of the lesion were similar to dermal dendritic melanocytic proliferation, but the histopathological findings were not conclusive regarding the subclassification to which this lesion belongs. The clinical features are more suggestive of dermal melanocytosis (especially nevus of Ota), as the lesion was patch-like, widely spreading and not confined to a small area, as seen in common blue nevus. 8 Additionally, cellular blue nevi are clinically similar because they can reach large sizes. 9 The histological features of our patient showed submucosal pigmented lesions. With high power, the lesion contained heavily pigmented macrophages and few scattered melanocytes with fibrosis. Malignant blue nevus was excluded because there was no malignant histological finding. Although the lesion was surely benign, it was difficult to classify it into a specific subclass. The histological hallmark of benign blue nevus (common blue nevus and cellular blue nevus) is the presence of dendritic melanocytes associated with a variably fibrotic stroma. The prognosis of both benign blue nevus and dermal melanocytosis is favorable, but these conditions require regular follow-up observation for any atypical histopathological finding. 8
Follow-up of our case with radiological imaging showed benign features with no malignant behavior, such as bony invasion or metastasis to other structures. 10 Finally, histopathological findings were consistent with benign mucosal melanosis. Similar lesions are Naves of Ota, Naves of Ito and Benign blue nevus.
To the best of our knowledge, our report is the first to describe an adult patient with a pigmented middle ear lesion that extended to the inner ear and nasopharynx. The presence of melanocytic lesions in the middle ear mucosa was first described in 1976 by Babin and Benjamin. They reported a 28-year-old female patient with a 5 year history of progressive hearing loss who was found to have a pigmented lesion confined to the middle ear and was diagnosed with blue nevus. 6 In 2015, Saito and Ishikawa reported a 2-year-old female patient who presented with a blue tympanic membrane in the right ear. Radiological imaging and surgical exploration revealed a diffuse pigmented lesion in the middle ear that extended to the inner ear and nasopharynx through eustachian tube. 5 The last case was reported by Cho and Baek in 2018 and involved a 38-year-old female with a complaint of intermittent dizziness. After surgical exploration, they found a small, pigmented lesion within the middle ear. The lesion was diagnosed as Benign blue nevus. 4
All 3 previously reported patients were females. Two patients were adults and one was a pediatric patient. Unilateral profound hearing loss was observed in the pediatric patient on the same side of the lesion. Among the adult patients, one had bilateral hearing loss that did not seem to be associated with a unilateral lesion, the second adult patient had complaints of dizziness, and the lesion was incidentally discovered during examination. The middle ear lesion was confined to the middle ear only in the 2 adult female patients, while in the pediatric patient, the lesion extended to the inner ear and nasopharynx through eustachian tube.
Computed tomography scanning is helpful as the first imaging modality to establish the diagnosis, to collect information about the location and extent of the lesion, and to identify any malignant behavior, such as invasion to adjacent structures and bony erosion. 10 Computed tomography scans of previously reported cases identified mucosal thickening in diffuse lesions. However, in defined lesions, CT scans showed well-demarcated soft tissue density. Magnetic resonance imaging can provide more information about soft tissue and local extension and invasion of the lesion to soft tissue and is better in locating other similar lesions. High intensity on T1-weighted images and low intensity on T2-weighted images were obtained for the previous 2 patients. However, for the third patient, MRI was not performed. Radiologically, our case was consistent with previously reported cases. Although CT scans were not conclusive, MRI showed high-intensity lesions on T1-weighted images with low intensity on T2-weighted images. Imaging modalities are also helpful in following up these patients and monitoring any aggressive behavior or recurrence if the previous lesion was excised completely. 4 -6
Histopathological findings were reported as heavily pigmented elongated melanocytes in a compact collagenous stroma, oval-shaped cells containing abundant melanin pigment and spindle-to-epithelioid-shaped melanocytes with high levels of melanin. All the previous cases of lesions were not completely removed due to difficulty in performing the excision. However, all patients were followed up and described as having a benign clinical course without complications. 4 -6 A similar finding was observed in the present case, where the lesion was extensively and diffusely disseminated, which makes complete surgical excision impossible.
In conclusion, mucosal melanocytic proliferation should be included in the differential diagnosis of benign dark mucosal lesions in the middle ear. Reporting of similar cases is needed to establish knowledge of the effect of melanocytic lesions on hearing and other otological functions. Computed tomography scans and MRI are helpful in diagnosing these cases and providing more lesion descriptions. In the case of a lesion that is confined to the middle ear mucosa, it should be removed completely for diagnostic purposes and to prevent the lesion from spreading. Pigmented lesions in the middle ear can spread to the inner ear and to the eustachian tube, reaching the nasopharynx. Regular clinical follow-up with radiological imaging to monitor recurrence and malignant behavior is necessary. Histological findings are not always conclusive for categorizing already described dermal similar lesions. The hallmark of histopathological testing is the presence of heavily pigmented cells.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.