
Abstract
Objective
The study aimed to investigate the clinical characteristics of patients with multi-canal benign paroxysmal positional vertigo (MC-BPPV).
Methods
We performed a retrospective analysis of 927 patients with BPPV who were admitted to our hospital between January 1, 2016 and December 31, 2019. The clinical data of all patients were collected. The Dix-Hallpike, straight head-hanging, and supine Roll tests were performed in all patients. The nystagmus was recorded using videonystagmography. The clinical characteristics of patients with MC-BPPV and single canal BPPV (SC-BPPV) was analyzed and compared.
Results
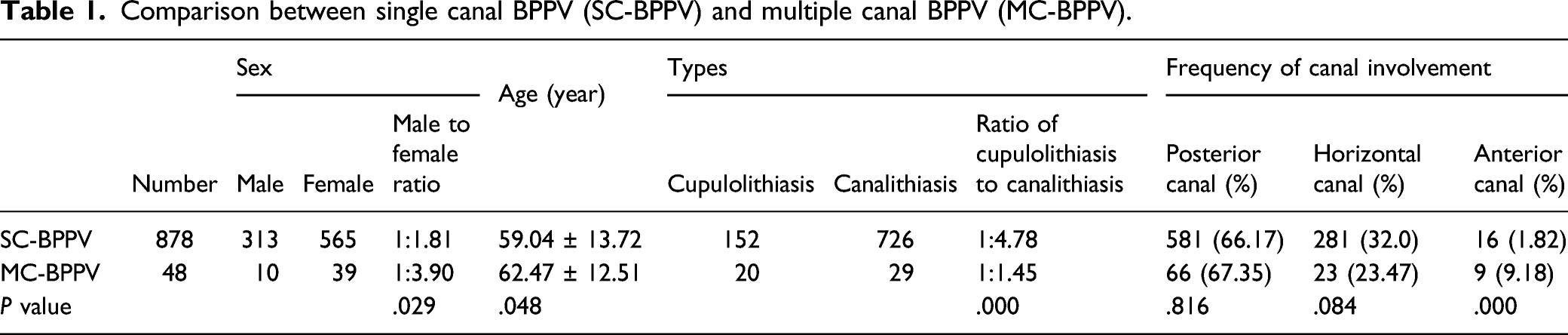
Among 927 patients included, 49 (5.29%) patients had MC-BPPV, 878 (94.71%) patients had SC-BPPV. There were significant differences in the male to female ratio (1:3.90 vs 1:1.81, P < .05), mean age (62.47±12.51 vs 59.04±13.72, P < .05), as well as the ratio of cupulolithiasis to canalithiasis (1:1.45 vs 1:4.78, P < .01) between patients with MC-BPPV and SC-BPPV. The frequency of involvement of PC, HC, and AC were involved for 66 (67.35%), 23 (23.47%), and 9 (9.18%) times, respectively, in patients with MC-BPPV, which were involved in 581 (66.17%), 281 (32.0%), and 16 (1.82%) patients, respectively, in patients with SC-BPPV. No significant difference was found in the frequency of involvement of PC and HC between patients with MC-BPPV and SC-BPPV, while there was significant difference in the frequency of AC involvement between 2 groups (P < .01). Ipsilateral PC-HC-BPPV (n = 18) and bilateral PC-BPPV (n=19) were the most common among patients with MC-BPPV. Twenty-six (53.06%) patients had ipsilateral MC-BPPV, 23 (46.94%) had bilateral MC-BPPV. Of the 26 patients with ipsilateral MC-BPPV, 7 patients combined with unilateral peripheral vestibular disorder.
Conclusion
Patients with MC-BPPV had a significantly older mean age at disease onset and a higher proportion of females compared with patients with SC-BPPV. Cupulolithiasis was more common in MC-BPPV. AC involvement was also much more common in MC-BPPV than in SC-BPPV.
Keywords
Introduction
BPPV is a peripheral vestibular disease induced by changes in the head position relative to the direction of gravity, which is characterized by recurrent transient vertigo and characteristic nystagmus. 1 BPPV is self-limiting and recurrent. It is generally believed that BPPV is caused by detached otoliths from the utricular macula that fall into the semicircular canals or adhere to the cupula, resulting in a series of symptoms and signs.2,3 BPPV mostly involves a single canal (SC-BPPV), the posterior canal (PC) is the most frequently affected canal, followed by the horizontal canal (HC), while BPPV involving the anterior canal (AC) is rare. BPPV can also involve multiple canals (MC-BPPV). 4 Compared with SC-BPPV, various forms of nystagmus can be observed in MC-BPPV, which can be easily confused with central positional nystagmus. Nystagmus generated by some type of SC-BPPV may be similar to that found in MC-BPPV, which bring difficulties for clinical diagnosis and treatment of MC-BPPV. In this study, we aimed to analyze the clinical features of patients with MC-BPPV.
Materials and methods
Patients
We retrospectively recruited 927 patients with BPPV who were admitted to the Vertigo Center of Xiangyang Central hospital between January 1, 2016 and December 31, 2019.
Inclusion criteria were (1) patients who had symptoms of paroxysmal positional vertigo and (2) patients who had characteristic nystagmus seen by video-oculography (VNG). Detailed medical history of all patients were collected. Dix–Hallpike (D–H), Roll and straight head-hanging (SHH) tests were performed in all patients. Nystagmus was recorded using VNG. All patients underwent electro-otoscopy and caloric test, some patients underwent blood routine, biochemical tests, and audiology examination. Brain MRI was performed on atypical patients.
Diagnosis of different types of BPPV 5
(1) PC-BPPV was diagnosed if up-beating nystagmus with torsional component was induced by D–H test when the affected ear is directed towards the earth, and the torsional component was directed to the affected ear, the nystagmus direction reversed upon sitting up. (2) HC-BPPV was diagnosed if geotropic, apogeotropic horizontal nystagmus on both sides was induced by supine Roll test. (3) AC-BPPV was diagnosed if vertical down-beationg nystagmus with/without torsional component was induced by D–H and SHH tests. (4) MC-BPPV was diagnosed if the typical nystagmus of multiple canals involved on D-HT, SHH and supine Roll tests was observed. Patients who had HC-BPPV with light cupula (geotropic horizontal nystagmus on both sides induced by Roll Test, lasting >1min) was excluded from this study.
Statistical Analysis
Statistical analyses were performed using SPSS24.0 software. The differences in the male to female ratio, the incidence ratio of different types of MC-BPPV, and frequency of involvement of different canals were analyzed by χ2 test. The difference in age between the groups was analyzed using independent sample t test. Results were considered statistically significant if P < .05.
Results
A total of 927 patients with BPPV were included in the study. Among these patients, 581 (62.68%) patients had PC-BPPV, 281 (30.31%) patients had HC-BPPV, 16 (1.73%) patients had AC-BPPV, and 49 (5.29%) patients had MC-BPPV (Figure 1). The incidence of different types of BPPV.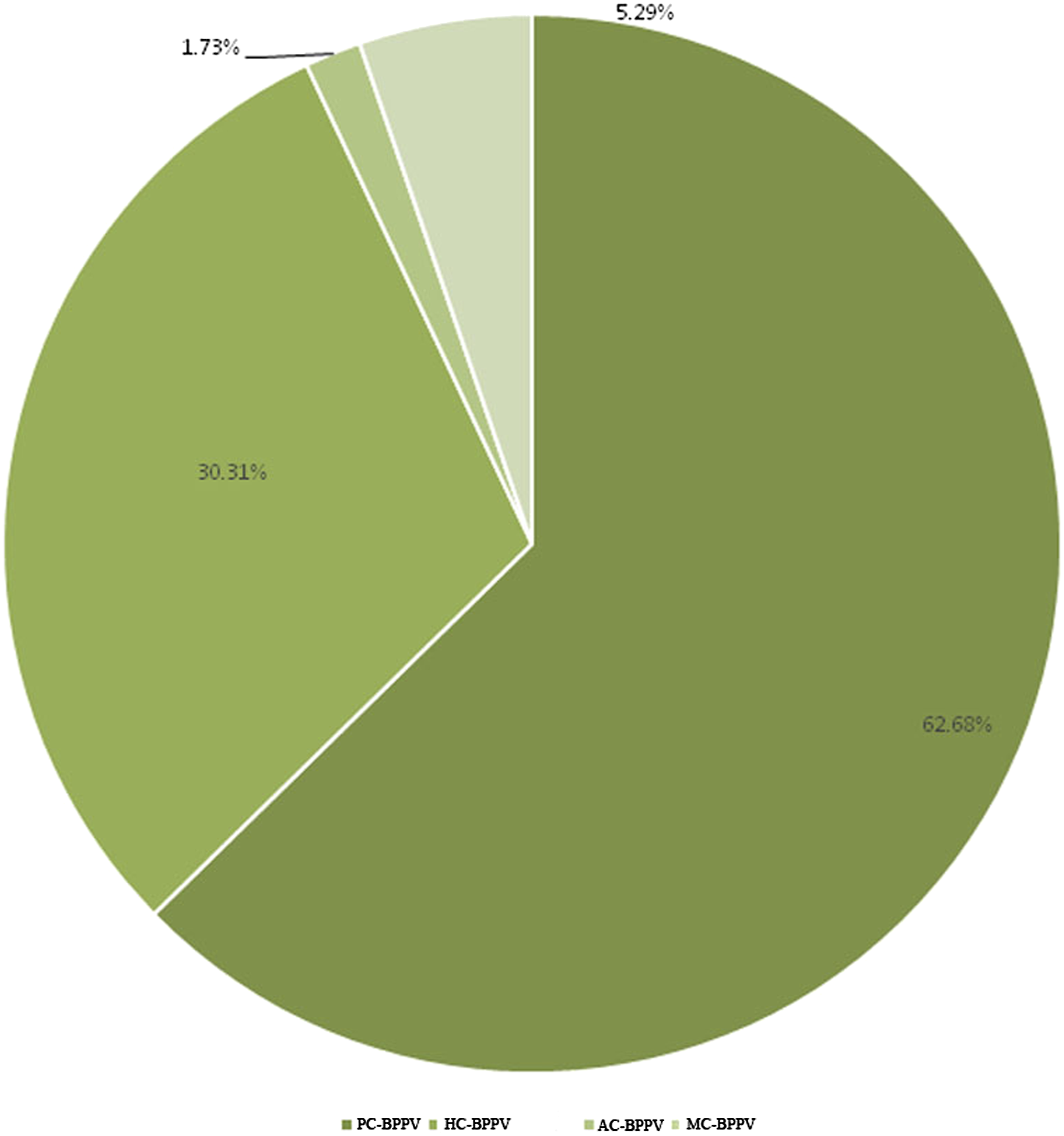
Among 878 patients with SC-BPPV, there were 313 males and 565 females, with a male to female ratio of 1:1.81, the mean age was 59.04±13.72 years. Among 49 patients with MC-BPPV, there were 10 males and 39 females, with a male to female ratio of 1:3.90, the mean age was 62.47±12.51. The ratio of cupulolithiasis to canalithiasis in patients with SC-BPPV was 1:4.78, which was 1:1.45 in patients with MC-BPPV (P < .01). There were significant differences in the male to female ratio, mean age, and the ratio of cupulolithiasis to canalithiasis between patients with MC-BPPV and SC-BPPV (P < .05, P < .05, P < .01, respectively).
Comparison between single canal BPPV (SC-BPPV) and multiple canal BPPV (MC-BPPV).
Involvement of different canals in patients with multiple tube stones (MC-BPPV).
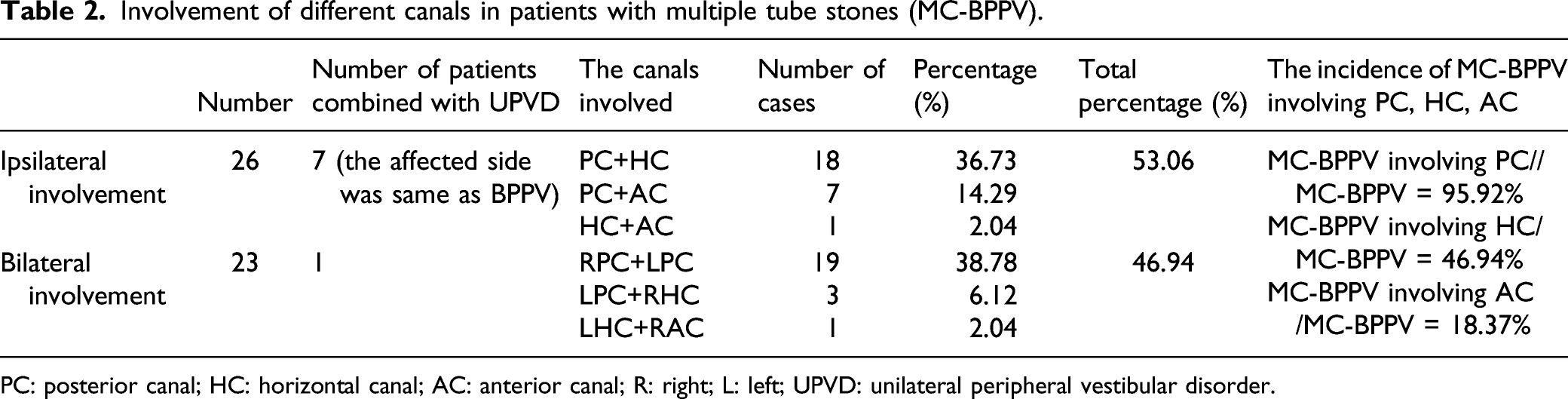
PC: posterior canal; HC: horizontal canal; AC: anterior canal; R: right; L: left; UPVD: unilateral peripheral vestibular disorder.
Discussion
The incidence of multiple canal BPPV (MC-BPPV) and different canal involvement reported in the present study and previous studies.
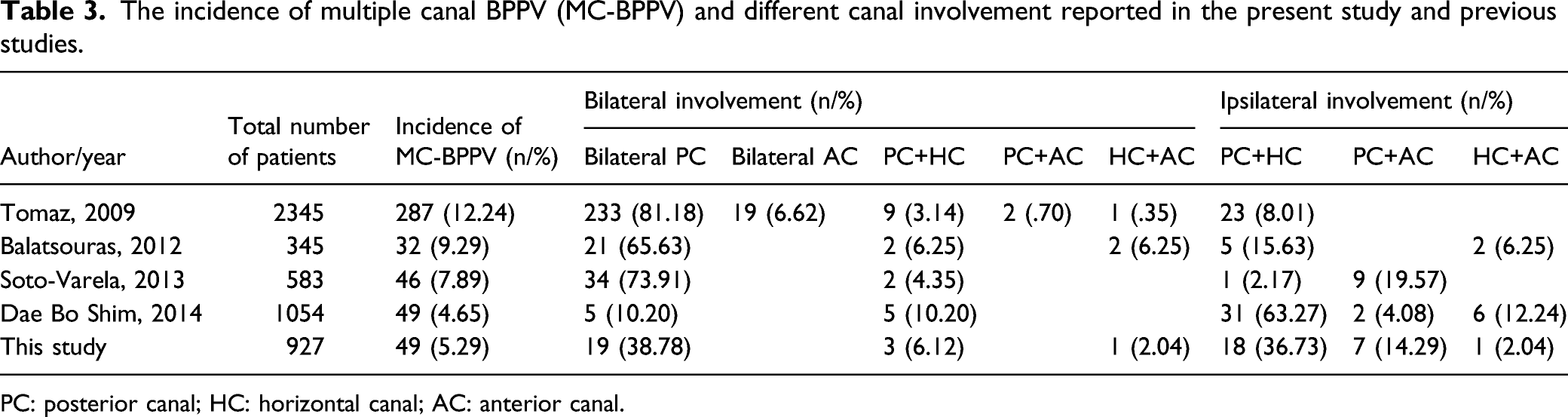
PC: posterior canal; HC: horizontal canal; AC: anterior canal.
Current theories generally believe that BPPV is caused by the detached otoliths from the macula that fall into the semicircular canals. When the head moves in the plane of the affected semicircular canal, the otoliths move under the action of gravity, that drives endolymphatic fluid flow, leads to cupula displacement, thereby inducing positional vertigo and nystagmus, this condition is known as canalithiasis. 16 Another much rarer type of BPPV is cupulolithiasis, when otoliths adhere to the cupula of the semicircular canal, the density of the cupula is higher than that of the endolymph, then changes in head position can cause the displacement of cupula under the action of gravity, thus inducing positional vertigo and nystagmus. 17 The proportion of MC-BPPV involving different semicircular canals, is rarely reported in previous studies. A study included 176 patients with BPPV conducted by Claudio et al 18 showed that 3 patients had MC-BPPV, including 2 patients of PC-HC-BPPV-cupulolithiasis, and 1 patient of PC-HC-BPPV-canalithiasis. And compared with patients with canalithiasis, canalith repositioning maneuver was not effective in these 2 patients who had cupulolithiasis, and repeated canalith repositioning maneuvers and Brandt–Daroff exercises were needed in order to achieve good results. Si et al 19 performed an analysis of 41 patients with MC-BPPV and found that 46.3% patients had nystagmus that lasted more than 1 min, 14.6% patients had cupulolithiasis, and 31.7% patients had mixed cupulolithiasis and canalithiasis, they also found that canalith repositioning maneuver was more effective in patients with canalolithiasis compared to those with cupulolithiasis and mixed canalolithiasis-cupulolithiasis. In this study, we found that among the 878 patients with SC-BPPV, there were 152 patients of cupulolithiasis and 726 patients of canalolithiasis, with a cupulolithiasis-canalolithiasis ratio of 1:4.78, while among 49 patients with MC-BPPV, 20 patients had cupulolithiasis and 29 patients had canalolithiasis, the cupulolithiasis-canalolithiasis ratio is 1:1.45, there was a statistical difference in the cupulolithiasis-canalolithiasis ratio between patients with BPPV and MC-BPPV. The higher proportion of patients with MC-BPPV who had cupulolithiasis may be due to that the when the original cupulolithiasis is not treated successfully, the otoliths detach from the utricles, and then enter into other semicircular canals, resulting in multiple canal involvement.
Among 49 patients with MC-BPPV included in this study, the 3 semicircular canals were involved for a total of 98 times, AC was involved for 9 (9.18%) times, while AC was involved in16 (1.82%) patients with SC-BPPV. Significant differences in the frequency of AC involvement were found between patients with MC-BPPV and SC-BPPV. Previous studies investigating the involvement of different semicircular canals in MC-BPPV showed that incidence of MC-BPPV involving the AC was 7.67% to 19.57%.10–13 In this study, we found that AC was involved in 9 patients, accounting for 18.37% of all MC-BPPV cases, this result is consisted with the above-mentioned findings. However, Si et al 19 reported that the incidence of MC-BPPV involving the AC was as high as 48.8%, the reason for the high incidence rate may be that patients admitted to vertigo centers of different levels have different disease severity, patients with BPPV who had typical symptoms can be diagnosed and treated in primary vertigo centers, and the proportion of patients with complex nystagmus admitted to higher-level vertigo center is high. Further multi-center studies with large sample sizes are needed to investigate the clinical characteristics of patients with different types of MC-BPPV.
MC-BPPV can involve either the ipsilateral or bilateral canals. In this study, 26 (53.06%) patients had ipsilateral MC-BPPV, and the incidence of ipsilateral PC-HC-BPPV was high, this result is consistent with the findings of previous studies,10,11,13 which is also consistent with the fact that otoliths are more likely to affect the PC and HC. 20 Simultaneous involvement of ipsilateral AC and PC was less common than involvement of PC and HC. The reason may be that the ends of AC and PC are joined to form common crus at the nonampullary end, the otoliths are more likely to enter the common crus when lying down, and fall off simultaneously into the 2 semicircular canals when turning from one side to the other.12 In this study, simultaneous involvement of ipsilateral AC and HC was observed in 1 patient. Bilateral MC-BPPV was identified in 23 patients, accounting for 46.94% of all MC-BPPV cases. Among these 23 patients, bilateral PC-BPPV was more common, with an incidence rate of 38.78%, which is lower than that reported in the studies of Tomaz et al, 10 Balatsouras et al 11 and Soto-Varela et al 12 (81.18%, 65.63%, and 73.91% , respectively). The reason may be that in these studies, patients with unilateral PC-BPPV who showed typical nystagmus during bilateral Dix–Hallpike test were misdiagnosed as bilateral PC-BPPV. 21 As early as 1994, Steddin et al 22 showed that in some patients with unilateral pc-BPPV, Dix–Hallpike test performed on the healthy side can cause the movement of otoliths in the posterior canal on the contralateral (affected) side to the ampulla, that rises inhibitory stimulus, thereby inducing torsional nystagmus with the horizontal component beated towards the healthy side and vertical component directed upward, which is considered as bilateral PC-BPPV. Lea Pollak et al 23 proposed the following method to distinguish unilateral and bilateral PC-BPPV: for patients presenting with up-beating torsional nystagmus during bilateral Dix-Hallpike, straight head-hanging (SHH) test should be performed, if torsional component disappears, and only the vertical up-beating nystagmus can be observed, the diagnosis of bilateral PC-BPPV is considered; if nystagmus induced by bilateral Dix-Hallpike is asymmetric, and bilateral nystagmus disappears after reduction performed on the side with stronger nystagmus and severe dizziness using Epley maneuver, unilateral PC-BPPV is considered. Because during SHH test, the PC on both sides is stimulated, and the nystagmus with torsional component has opposite directions and cancels each other out, while nystagmus with vertical components has same direction and is stronger. If nystagmus with torsional component directed towards the affected ear still exists, unilateral BPPV is considered. In this study, left PC combined with right HC were involved in 3 patients, left HC combined with right AC were involved in 1 patient.
Patients with bilateral AC-BPPV and bilateral HC-BPPV were not seen in our study. The main reason is that the diagnosis of bilateral AC-BPPV and bilateral HC-BPPV is more difficult in clinical practice. Theoretically, in patients with AC-BPPV, down-beating nystagmus with torsional component directed toward the affected ear is generated by the contraction of ipsilateral superior rectus and contralateral inferior oblique muscles during positional tests.24,25 The torsional component of the nystagmus may facilitate the determination of the affected side in patients with AC-BPPV. But in some patients, due to the anatomical structure of the canal, the Dix–Hallpike test can often stimulate the ampullary crest of the AC on both sides and induce bilateral down-beating nystagmus with no obvious torsional component,26,27 which makes it difficult to determine the affected side of AC-BPPV. Therefore, for the patients with BPPV, Yacovino maneuver that does not require determination of the affected side should be performed. 28 Similarly, the diagnosis of bilateral HC-BPPV is also very difficult, if patients had canalolithiasis or cupulolithiasis of the bilateral HC, the Roll Test can cause canal excitement on one side and inhibition on the other side when turning the head to either side. For the horizontal tube BPPV, the nystagmus produced by Roll test is more symmetrical in bilateral HC-BPPV as compared to unilateral HC-BPPV. However, this method is not reliable, because asymmetric involvement of the bilateral HC may also occur, so audiological evaluation, the presence of peripheral vestibular diseases, and the effectiveness of canalith repositioning maneuvers can be used to assist in identifying the affected side.
In this study, we found that among 26 patients with ipsilateral MC-BPPV, 7 patients combined with ipsilateral peripheral vestibular dysfunction, while only 1 patient with bilateral MC-BPPV patients combined with peripheral vestibular dysfunction. Ipsilateral MC-BPPV usually develops when patients have ipsilateral peripheral vestibular diseases such as Meniere’s disease and sudden deafness, and is prone to recurrence. 29 Bilateral MC-BPPV may be secondary to head trauma.10,30,31 The limitations of our study are that the etiology of MC-BPPV was not systematically investigated, and treatment efficacy in patient included in the study was not analyzed. In the future, we will evaluate patients' past medical history, complications, and vestibular function evaluation results in detail, and perform a long follow-up investigation in order to explore the pathogenesis, clinical characteristics, diagnosis, and treatment strategies of MC-BPPV.
Footnotes
Declaration of Competing Interest
The authors declare that they have no competing interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by 2018 Science and Technology Project of Health Commission of Hubei Province (No. WJ2019F095), and the 2017 project of Xiangyang Science and technology bureau (Xiangkeji [2017] No. 10-41), and the 2021 project of Xiangyang Science and technology bureau (No. 2021YL13).