
Abstract
Blue nevus is a type of uncommon benign pigmented lesion in the skin or the mucosa of human body which is featured by pigmented dendritic melanocytes and spindled melanocytic cells. Sinonasal blue nevus is extremely rare. We reported a sinonasal blue nevus case with the background of pituitary adenoma, type 2 diabetes mellitus, and hypertension (including endoscopic and histological pictures). Further, the existing literature about blue nevus is reviewed. This paper puts a spotlight on the potential correlation between blue nevus with the endocrine system disorder and provides support for further experimental research.
Introduction
Pigmented lesions are common in the skin and the mucous of the human body, while sinonasal pigmented lesions are rare. Blue nevus, a kind of uncommon benign pigmented lesions, is characterized by the proliferation of deeply pigmented dendritic melanocytes and spindled melanocytic cells. It has been reported in the bronchia area, 1 subungual area, 2 rectal mucosa, 3 vagina, 4 and extensive intraoral area. 5 Furthermore, blue nevus has been found in the Carney complex, 6 a complex of myxomas, spotty pigmentation, endocrine overactivity, and schwannomas. Since few studies have paid attention to blue nevus and endocrine overactivity, we reported a sinonasal blue nevus case of a potential correlation with the endocrine system and review the literature about the blue nevus.
Case presentation
A 58-year-old, Chinese man presented to the otorhinolaryngology head and neck surgery clinic with a persistent nasal obstruction after the resection of a pituitary adenoma (measured 1.2×1×.3 cm3). He received endoscopic transnasal transsphenoidal pituitary surgery. The immunophenotype of the adenoma tissue indicated a gonadotropin cell adenoma after the immunohistochemical analysis. Positive expressions were detected of SF-1, LH (partial), FSH (partial), and Ki-67 (the positive rate was 2%) in immunohistochemistry, while the expressions of PIT, ACTH, hGH, PRL, and TSH were not detected. Subsequently, he had a symptom of a bilateral and persistent nasal obstruction 1 month after the operation. Additionally, he had a background of hypertension and type 2 diabetes mellitus more than 5 years which were well controlled under the regular medication.
Physical examination showed that bilateral nasal cavities had severe adhesion. Subsequently, the patient received adhesiolysis nasal surgery. A pigmented lesion was found in the mucosa of the left nasal floor (Fig. 1). Endoscopic photograph of the blue nevus before the removal. Pigmented lesion (white arrow) was in the mucosa of the left nasal floor, the surface of which was smooth. The blue arrow pointed out the left inferior turbinate.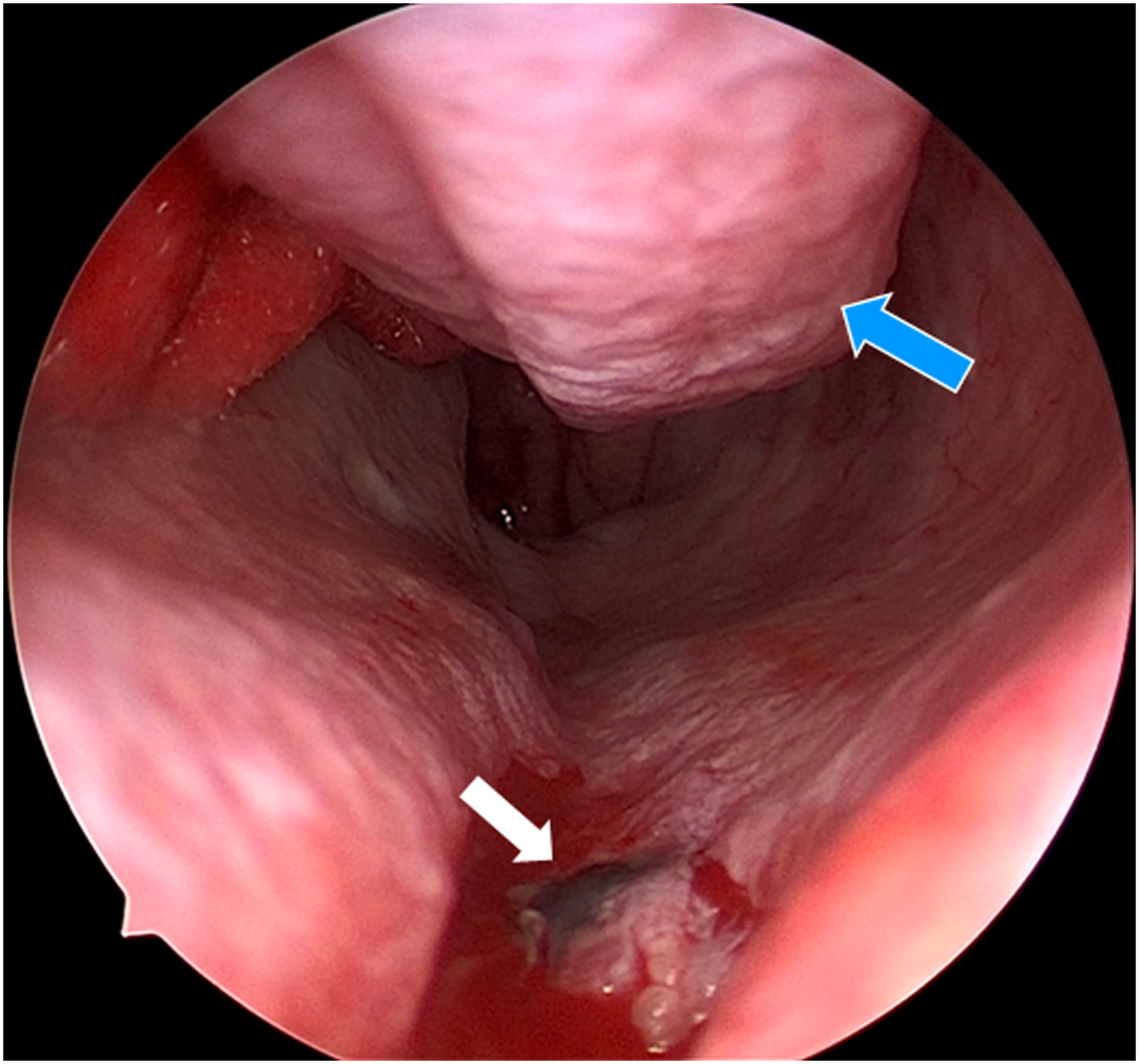
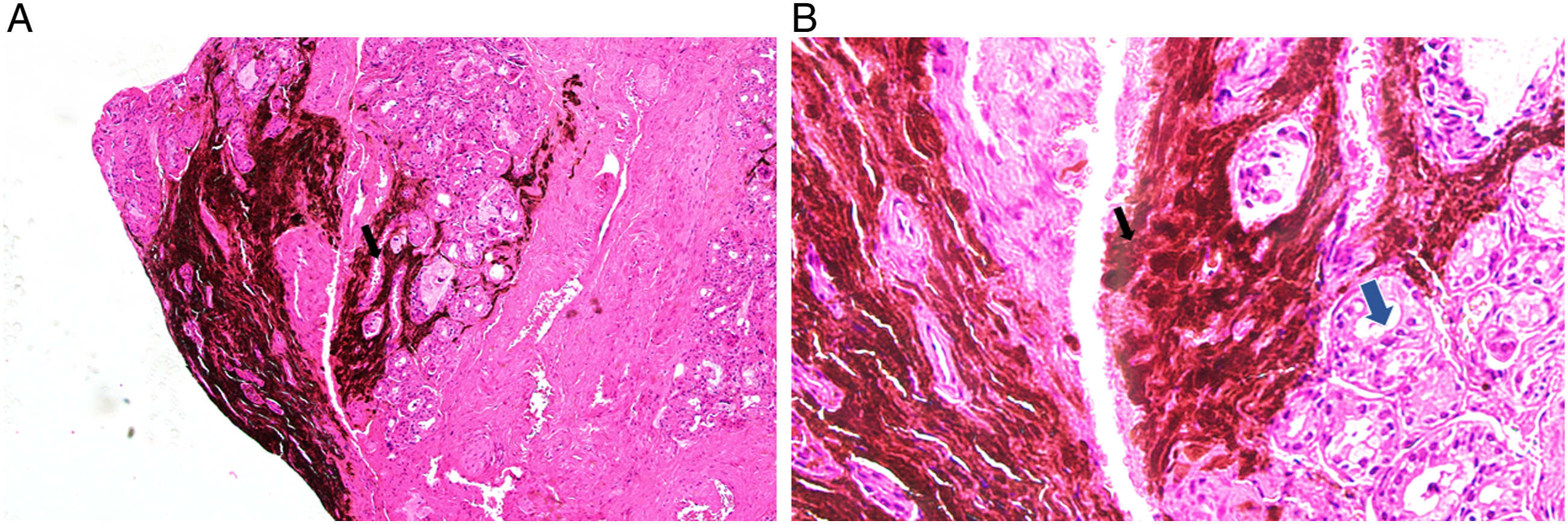
The pigmented lesion was completely resected in the operation room for surgical therapy of the patient with local anesthesia (Fig. 2). Histological examination showed that heavily pigmented dendritic cells and spindle cells accumulated within the stromal tissue, and bland nuclei occurred among the mucosal glands of the nasal mucosa (Fig. 3). Endoscopic photograph of the blue nevus after the removal. The pigmented lesion was completely resected, and the mucosa around the lesion was cauterized by radiofrequency for the additional removal and coagulation. Histopathology of pigmented lesion. (hematoxylin and eosin stain). (a) (Original magnification ×100), (b) (Original magnification ×400). Heavily pigmented dendritic cells and spindle cells accumulated within the stromal (dark arrow). Bland nuclei occurred among the mucosal glands of the nasal mucosa (blue arrow).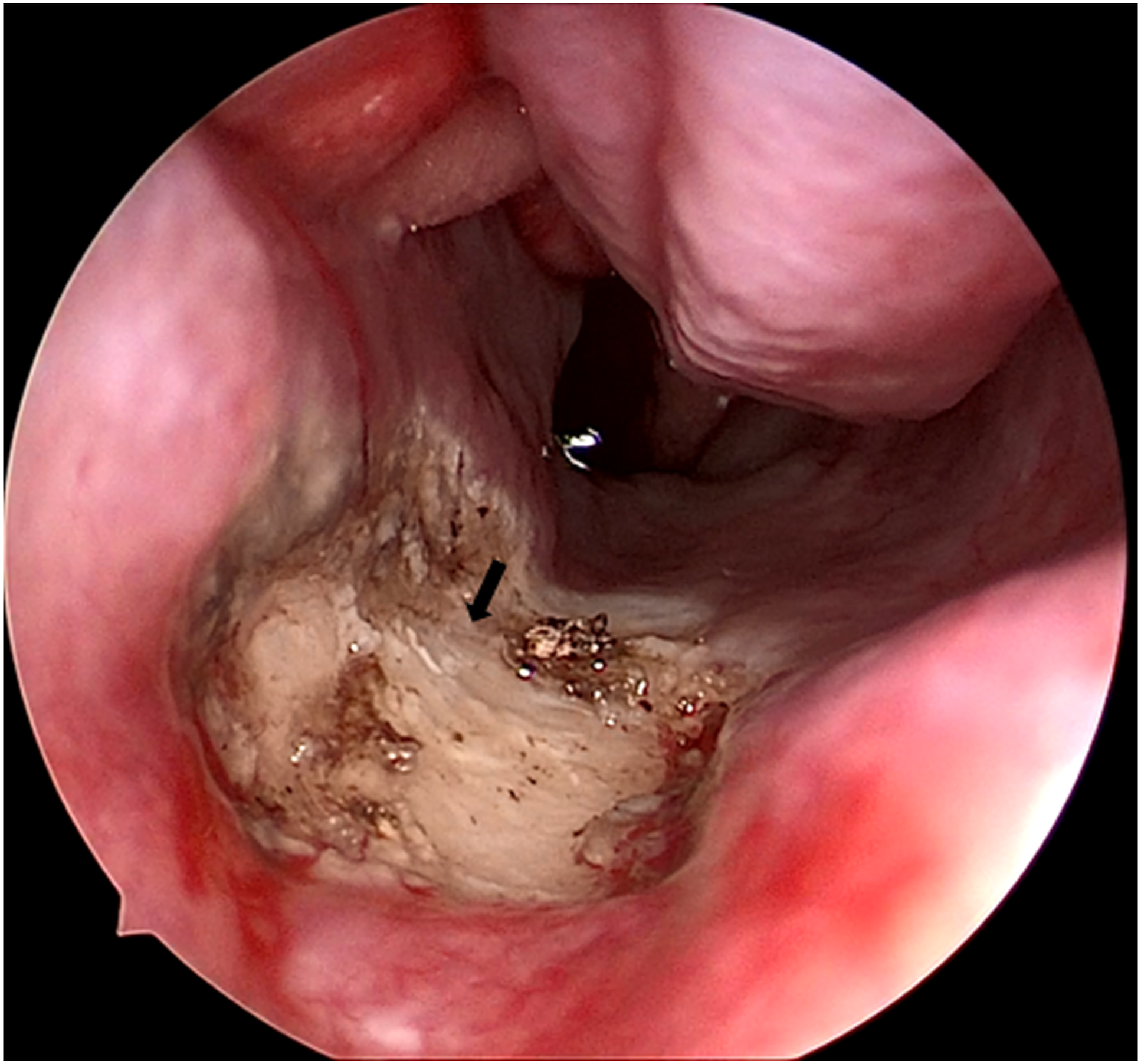
Blue nevus was the diagnosis after the integrated analysis of the clinical and the histological information. At 1-month follow-up, the patient had good wound healing outcome after operation (Fig. 4) and had no recurrent indication of blue nevus. Endoscopic photograph of the blue nevus after the resection. (a) 2 weeks after the operation. (b) 4 weeks after the operation. Repair and epithelization occurred on the wounded mucosa.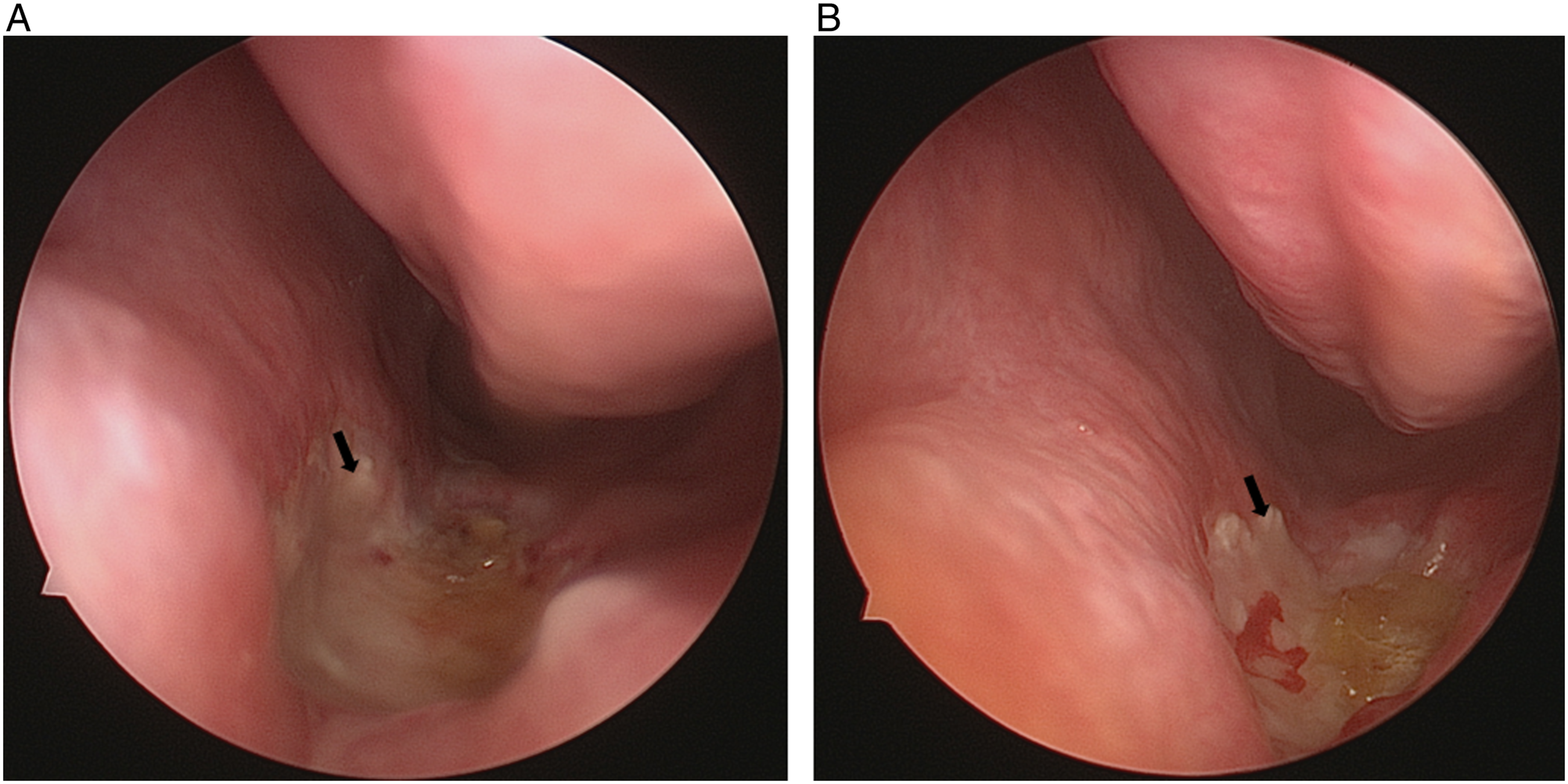
Discussion
Although it has been reported in many parts of the human body, blue nevus in the nasal cavity and sinuses remains rare. J Aneiros first reported the blue nevus in the maxillary sinus, 7 a case of a 28-year-old white woman with blue nevus which was found in the resection of maxillary sinus mucosa and confirmed eventually by immunohistochemical and electron microscopic analysis. The crucial diagnostic factor of the sinonasal blue nevus is histological diagnosis, 8 it is characterized by heavily pigmented dendritic melanocytes within the blue nevus.
As a type of pigmented lesions, blue nevus is supposed to be considered in the differential diagnosis with malignant melanoma. On the one hand, dendritic melanocytes in blue nevus are conformed to be infrequent mitotic activity and show no atypia. On the other hand, based on human melanoma black-45 (HMB-45), blue nevus had uniform immunoreactivity, while melanomas showed a patchy reaction type by the immunohistochemistry analysis.
Several cases of sinonasal blue nevus have been reported previously,8,9 but little background of the endocrine system disease was mentioned. In this case, blue nevus was found in a patient with pituitary adenoma, type 2 diabetes mellitus, and hypertension. These diseases of the endocrine system indeed led to a hormone disorder. Significantly, researches have indicated that hormone therapy had a positive association with the melanocytic nevi count in melanocytic nevi patients 10 and local hormones had an effect on nevus-related reduction of fat and muscle in children with congenital melanocytic naevi. 11 Besides, evidence showed that hormone supplements might be associated with the increased rate of dysplastic nevus. 12
Pituitary adenoma was commonly related to the growth of hormones including prolactin, corticotropin, or thyrotropin. 13 The hormones may play an important role in the occurrence and the development of nevus, and further research is needed in the exploration of the relationship between blue nevus and the endocrine disease.
Conclusion
In this paper, we reported a sinonasal blue nevus case with the background of pituitary adenoma, type 2 diabetes mellitus, and hypertension, and reviewed the existing literature about the blue nevus. This case, we believe, will put a spotlight on the potential correlation of blue nevus with the endocrine system disorder and provide support for further experimental research.
Footnotes
Author Contributions
This research was conducted in collaboration with all authors.Rui Lu and Zhiyong Li have been involved in drafting the manuscript and revising it critically for important intellectual content.Zhiyong Li and Wei Xiao gave final approval of the version to be published.Rui Lu, Zhiyong Li, Wei Xiao, and Xiong Chen have made contributions to conception and design.All authors agreed to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The authors declare that they have no competing interests.
Funding
This study was supported by National Natural Science Foundation of China (NSFC) grants 81900913(Zhiyong Li).
Ethical approval
The patient involved in this study gave his informed consent. Institutional review board approval of our hospital was obtained for this study.
Informed consent
The patient involved in this study gave his informed consent.