
Abstract
Objectives
This study investigated the effectiveness of a specialized manual physical therapy (PT) program at improving voice among patients diagnosed with concomitant muscle tension dysphonia (MTD) and cervicalgia at a tertiary care voice center.
Materials and Methods
Cervicalgia was determined by palpation of the anterior neck. Both voice therapy (VT) and PT was recommended for all patients diagnosed with MTD and cervicalgia. PT included full-body manual physical therapy with myofascial release. Patients underwent: 1) VT alone, 2) concurrent PT and VT (PT with VT), 3) PT alone, 4) VT, but did not have PT ordered by treating clinician (VT without PT order) or 5) VT followed by PT (VT then PT). The pairwise difference in post–Voice Handicap Index-10 (VHI-10) controlling for baseline variables was calculated with a linear regression model.
Results
178 patients met criteria. All groups showed improvement with treatment. The covariate-adjusted differences in mean post–VHI-10 improvement comparing the VT alone group as a reference were as follows: PT with VT 9.95 (95% confidence interval 7.70, 12.20); PT alone 8.31 (6.16, 10.45); VT without PT order 8.51 (5.55, 11.47); VT then PT 5.47 (2.51, 8.42).
Conclusion
Among patients diagnosed with MTD with cervicalgia, treatment with a specialized PT program was associated with improvement in VHI-10 scores regardless of whether they had VT. While VT is the standard of care for MTD, PT may also offer benefit for MTD patients with cervicalgia.
Introduction
Muscle tension dysphonia (MTD) is a voice disorder commonly encountered by otolaryngologists and voice speech language pathologists that is characterized by increased laryngeal musculoskeletal tension with excessive muscular recruitment in the larynx and pharynx with disruption of efficient vibratory parameters.1,2 MTD is classified as primary or secondary. Primary MTD occurs in the absence of identifiable fixed laryngeal pathology (e.g., vocal fold lesions, paralysis), while secondary MTD refers to that occurring concomitantly with such pathologies. Clinically, both types present with variable symptomology including hoarseness, vocal fatigue, effortful voice production, change in habitual pitch, reduced vocal range, pain with voice use, muscular cramping, and neck stiffness.2,3
Cervicalgia (i.e., neck pain) is the fourth leading cause of years lost to disability and commonly co-occurs with MTD. 4 It ranks just behind low back pain, depression, and arthralgia according to the Global Burden of Disease 2010 Study. 4 Cervicalgia can have many etiologies and commonly relates to spinal facet joints (e.g., arthritis), intervertebral discs, and surrounding fascia. 5 Most epidemiological studies report an annual prevalence ranging between 15% and 50%, with one systematic review reporting a mean rate of 37.2%. 6 The prevalence of neck pain is higher in females and peaks in middle age. 7
There is growing recognition that optimal voice production requires whole-body muscular engagement. Posture related to the spine, shoulders, heel and hip position can affect the voice.8–11 Core muscles and passive recoil of the thorax act to maintain adequate subglottic pressure for breath support. 12 Sternocleidomastoid, scalene, and trapezius muscle recruitment allow greater control of thoracic contraction during singing and complex speech tasks in which loudness and pitch are varied. This recruitment permits greater regulation of the subglottic pressures required to complete these demanding tasks. 13 Resonance also necessitates intricate coordination of muscles that alter tongue position, larynx height, and mouth opening. 14 Consequently, muscle imbalances can disrupt respiration, phonation, and articulation/resonance, subsequently producing symptoms of MTD.
In a systematic review from the Cochrane Collaboration, a combination of direct and indirect methods was found to be effective treatment for MTD. 15 Indirect methods include vocal hygiene and voice conservation education. Direct methods use vocal exercises and facilitators often combined with circumlaryngeal massage to increase efficiency of voice production and reduction of extra-laryngeal muscle tension. Manual circumlaryngeal massage is used to regulate and restore the balance of intrinsic and extrinsic laryngeal musculature during phonation. 14 Some have attributed a portion of MTD therapy failures to inadequate attention and treatment of extralaryngeal musculature imbalance in areas not typically considered essential to efficient vocal production (e.g., neck, back, shoulders, abdomen).16,17 Of note, previous preliminary studies regarding voice and physical therapy at Vanderbilt University did not specifically evaluate those with both MTD and cervicalgia with treatment modalities of voice therapy alone and physical therapy alone.16,17
Traditional MTD treatment includes therapy for the anterior neck.18,19 Holistic treatment of the vocal mechanism, however, requires collaboration with practitioners adept at treating neck, back, shoulder, thoracic, extremity, and diaphragmatic/abdominal muscular tension. Herein, we more thoroughly examine the effectiveness of a manual physical therapy treatment program for patients diagnosed with MTD and cervicalgia as an adjunct to traditional voice therapy.16,17 The aim of this study was to evaluate whether the addition of physical therapy with myofascial release improves patient-reported voices of those diagnosed with MTD and cervicalgia.
Materials and Methods
This study was approved by the Vanderbilt University Medical Center Institutional Review Board (#181502). No adverse events were encountered. A query of the electronic medical record identified adult patients based on ICD-9 codes 784.42 and 723.1 between 2012 and 2018 treated at the Vanderbilt Voice Center. Medical records of patients were hand searched to assess candidacy for study inclusion. To be included, patients had to have 1) concomitant diagnoses of primary MTD and cervicalgia made by a laryngologist; 2) two completed VHI-10 scores with an initial score ≥7 during a continuous treatment period; 3) had no prior laryngeal surgery; 4) had no treatment lapses >90 days (defined as 90 days without any laryngology visit or VT or PT intervention); and 5) ≥18 years of age.
Primary MTD was defined as dysphonia in the absence of laryngeal lesions, neurological laryngeal disorders or prior laryngeal surgery.1,15 Cervicalgia was defined as prominent elicited tenderness on digital palpation of the strap, digastric, base of tongue/geniohyoid and/or sternocleidomastoid muscles, which was often accompanied by muscle hypertonicity, cervical trigger points or thyrohyoid space tenderness. Therefore, all patients in this study had clinically significant cervicalgia and MTD on evaluation by the treating laryngologist and were counseled on PT and VT. The VHI-10 threshold of excluding those with a score of <7 was chosen for two reasons. First, it represents one standard deviation (SD) above the normative mean value for the VHI-10 which is 6.76 20 and second, because when the VHI-10 was originally developed and validated, one SD below the mean value for those diagnosed with MTD was a VHI-10 score of 7.70. 21 Patients with lapses in care were excluded because recommended treatment was interrupted, thus affecting its potential effectiveness. Such a lapse may also imply a cessation of treatment by the patient against clinician recommendation.
Treatment Groups
The treating laryngologist counseled all affected patients on vocal hygiene and recommended them for VT and PT. All patients had a PT order in place except the VT without PT order group as seen below. The temporal order of these treatments was not prescribed; thus, patients underwent: 1) VT alone, 2) concurrent PT and VT (PT with VT), 3) PT alone, 4) VT, but did not have PT ordered by treating clinician (VT without PT order) and 5) VT followed by PT (VT then PT). The VT without PT order group was included because it is indicative of the shared decision-making involved in a patient-centered approach to medicine. After presenting and recommending the option of PT, some patients were not interested, and therefore, no PT order was placed. Besides the VT without PT order group, all groups had a PT order in place to include the VT alone group. Therefore, VT and PT were ordered for the VT alone group but only VT was completed due to patient choice or circumstances.
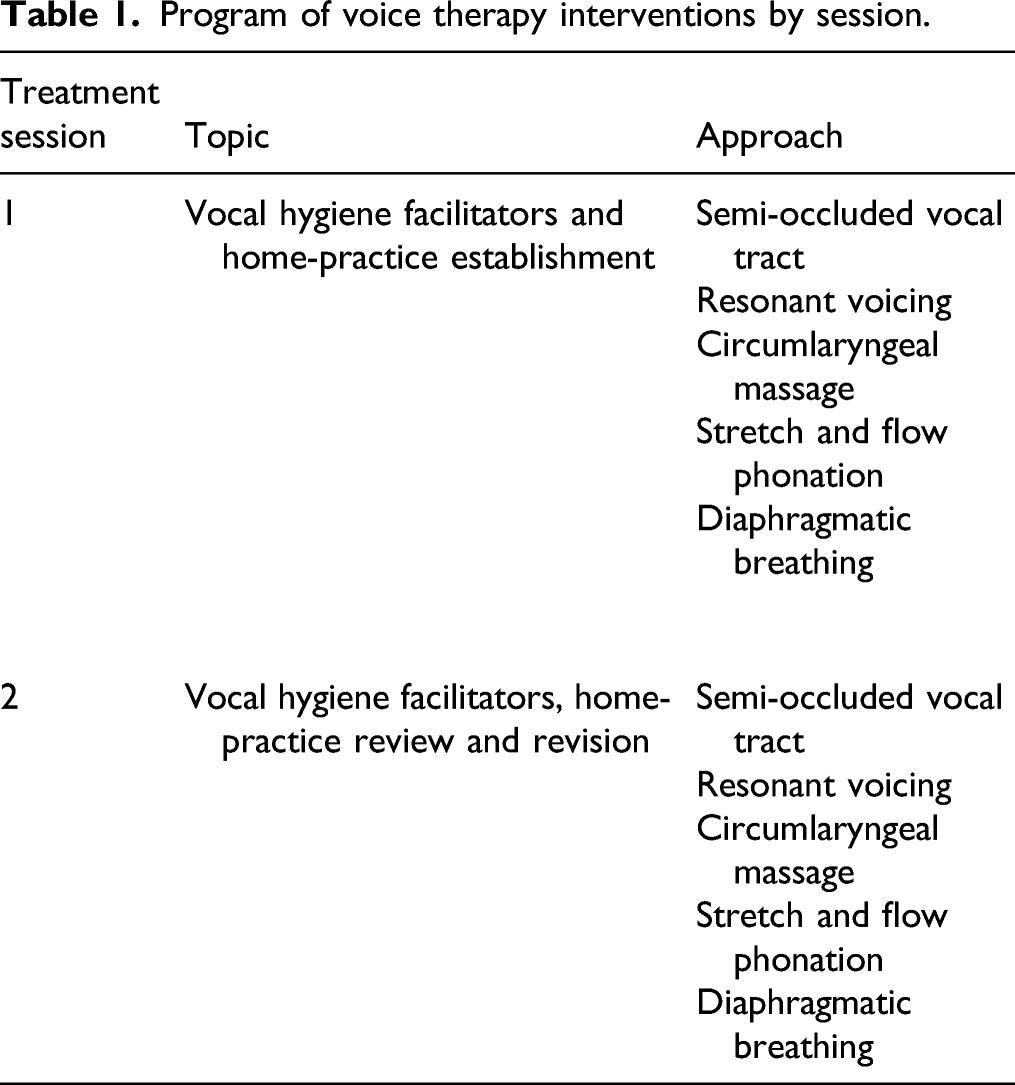
Program of voice therapy interventions by session.
Program of physical therapy interventions by session.
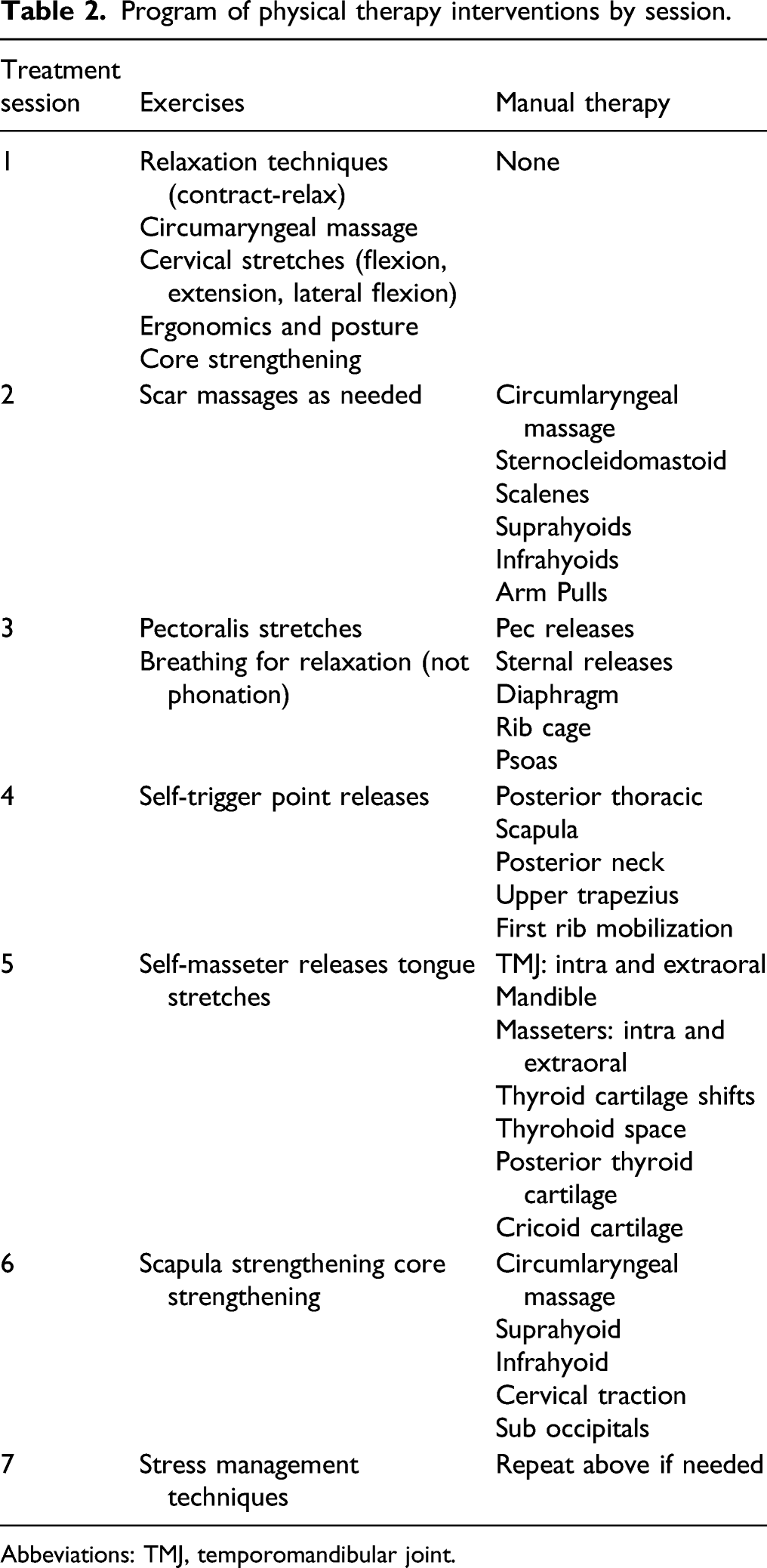
Abbeviations: TMJ, temporomandibular joint.
PT clinicians assessed patient functional status improvement using the Patient-Specific Functional Scale (PSFS). The PSFS tracks changes within individuals and is validated for cervicalgia.26,27 The minimal important difference (MID) of the PSFS is two points for cervicalgia patients. 28 The PSFS was taken at the beginning and end of the PT treatment period. For the VT then PT treatment group, the PSFS was taken before and after the physical therapy portion of therapy only. In addition, the PSFS was not utilized at all for the VT only group or VT without PT order group.
Data Abstraction and Variables
One investigator extracted patient information from the medical record and an independent second investigator confirmed and validated data integrity. Specific components included patient characteristics, diagnosed disorders, treatments and VHI-10 scores. 21 Past medical history with a focus on psychosomatic and pain related comorbidities were extracted from medical records as well. These included, but were not limited to, chronic pain, anxiety, and depression; and were selected because they often coexist with MTD and can be treatment effect modifiers.29–32 The Charlson Comorbidity Index (CCI) was calculated. 33 All abstracted data was entered into a secure Research Electronic Database Capture System (REDCap) database. 34
Statistical Analysis
Comparison of median patient characteristics by treatment group.
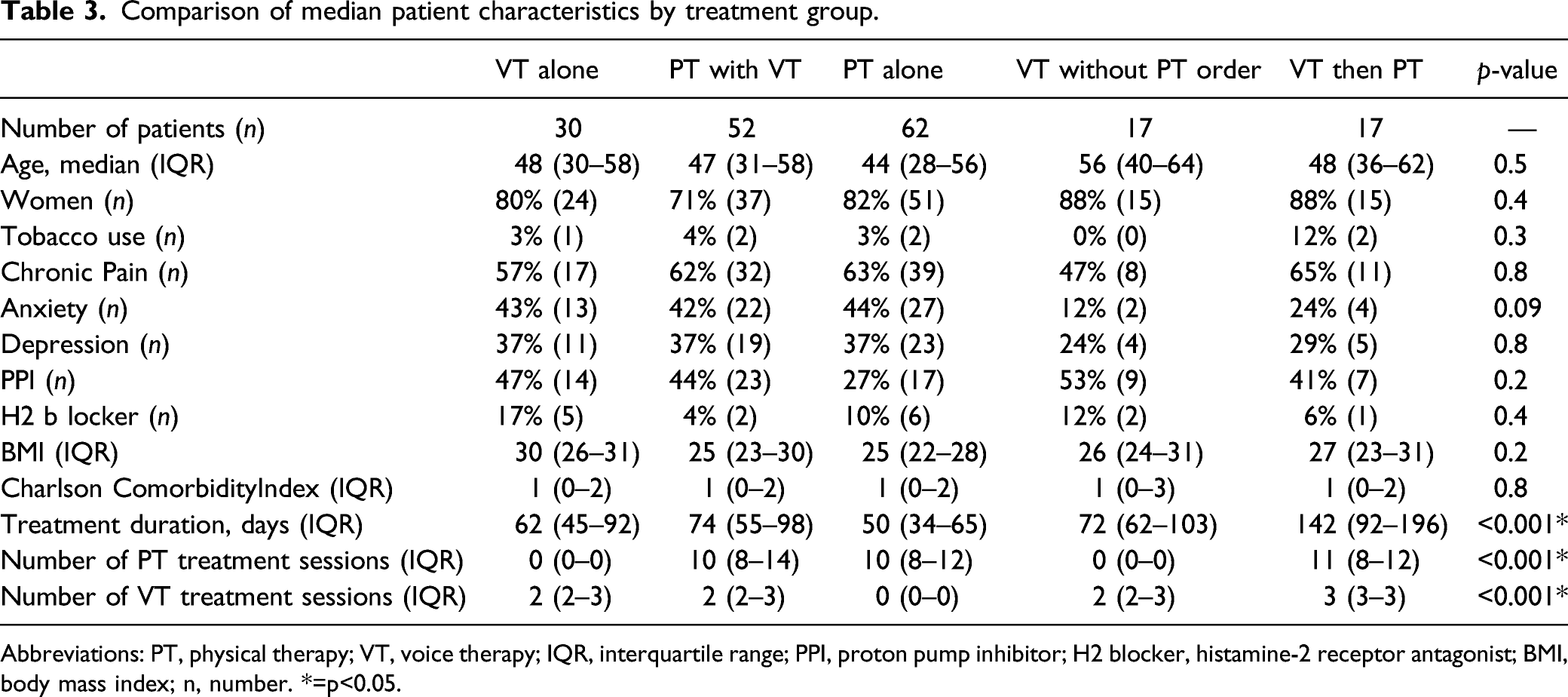
Abbreviations: PT, physical therapy; VT, voice therapy; IQR, interquartile range; PPI, proton pump inhibitor; H2 blocker, histamine-2 receptor antagonist; BMI, body mass index; n, number. *=p<0.05.
A host of secondary post-treatment endpoints were evaluated by fitting cumulative probability models with logit link, often called the proportional odds ordinal regression model. The only covariates included were pre-treatment scores and treatment group. The ordinal regression model is highly flexible and ideal for settings where a linear regression might not provide adequate fit. The resulting regression parameters can be interpreted as log relative odds. For each secondary endpoint, odds ratio (OR) and corresponding 95% confidence interval (CI) where calculated for each treatment group using the VT alone group as reference.
Results
Comparison of Voice Handicap Index-10 by treatment group.
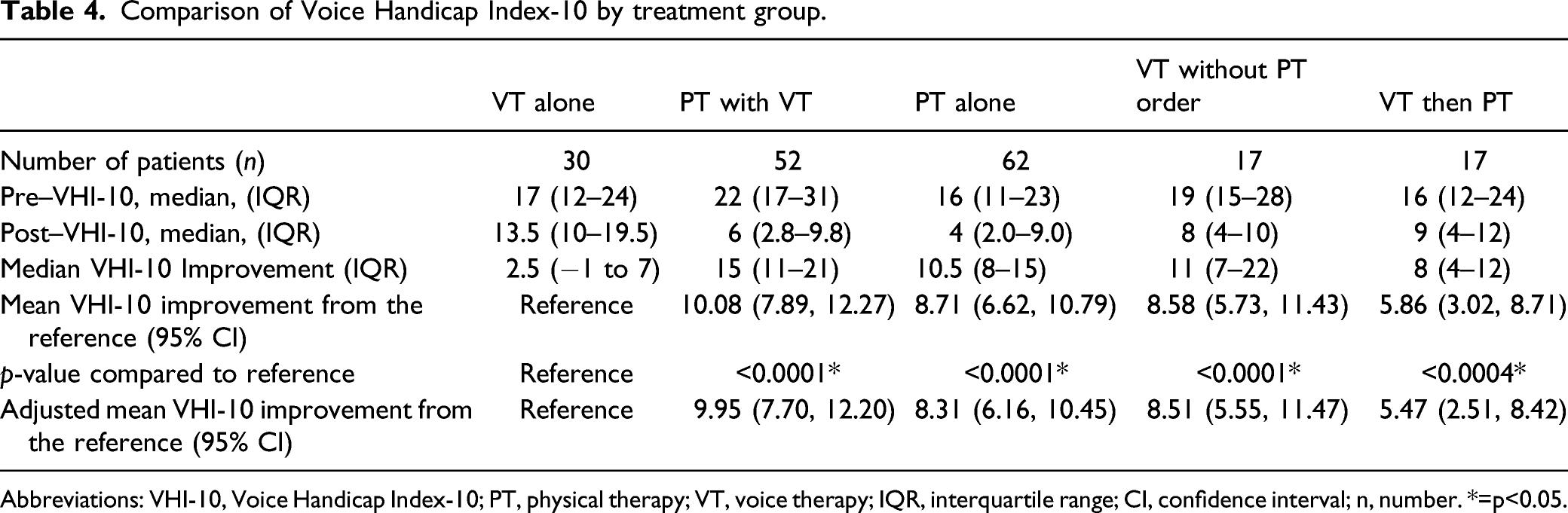
Abbreviations: VHI-10, Voice Handicap Index-10; PT, physical therapy; VT, voice therapy; IQR, interquartile range; CI, confidence interval; n, number. *=p<0.05.
Voice Outcomes
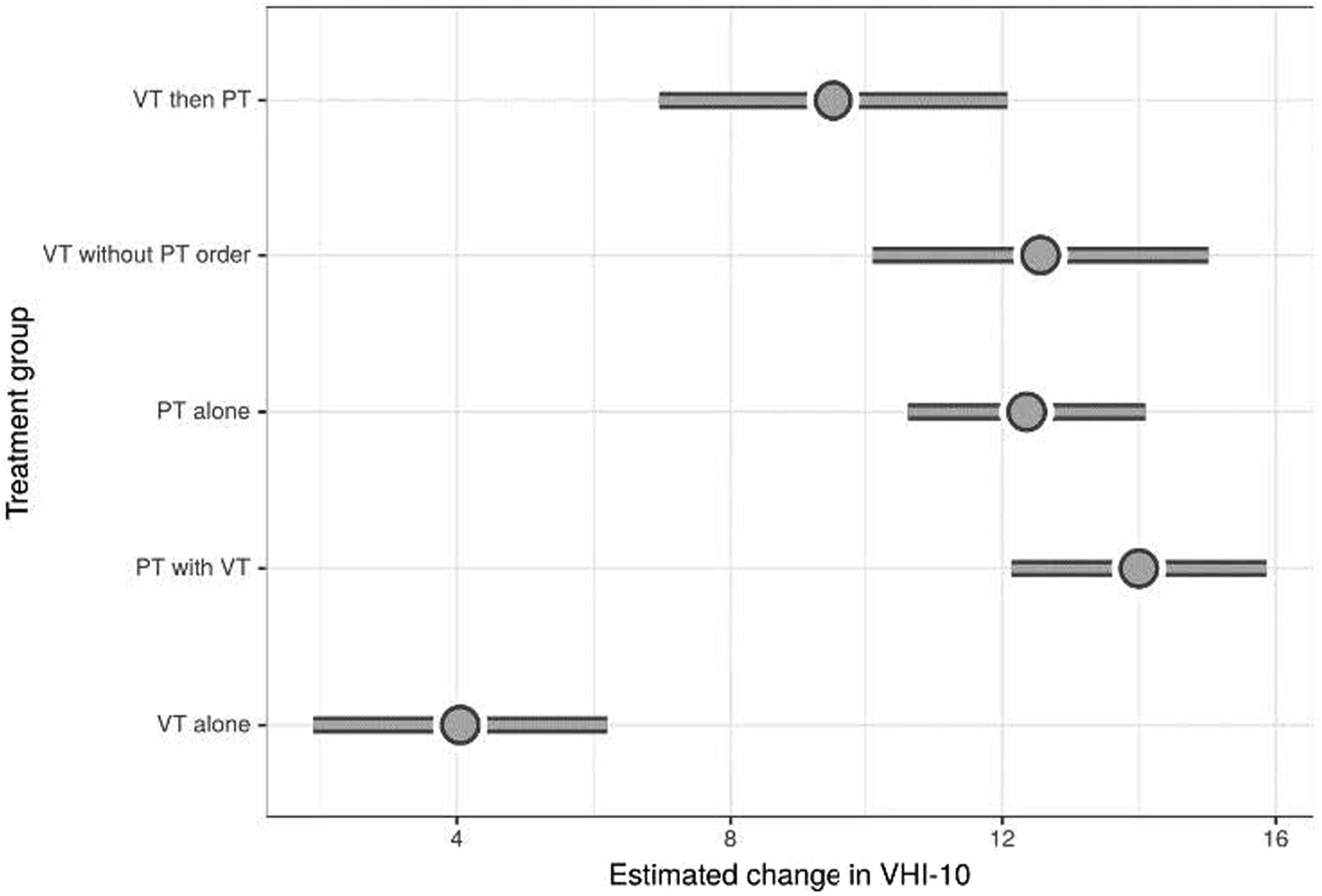
Median VHI-10 scores improved in all treatment groups. In order of greatest improvement, patients in the PT with VT treatment group had a median reduction in VHI-10 scores of 15 (IQR 11–21) followed by PT alone (10.5, IQR 8–15), VT then PT (8; IQR 4–12) and VT alone 2.5 (IQR −1 to 7). Scores of patients treated with VT without PT order improved by 11 (IQR 7–22; Table 4 and Figure 1). Using VT alone group as the reference, covariate-adjusted differences in mean post–VHI-10 improvement were: PT with VT 9.95 (95% Confidence Interval 7.70, 12.20); PT alone 8.31 (6.16, 10.45); VT without PT order 8.51 (5.55, 11.47); VT then PT 5.47 (2.51, 8.42; Table 4). Differences are shown graphically in Figure 2, which depicts VHI-10 improvements adjusted for a 47-year-old female without depression, anxiety, chronic pain or a smoking history with a pre–VHI-10 of 19. Dot plot of the median improvement in Voice Handicap Index-10 scores by treatment group with interquartile range; Abbreviations: PT, physical therapy; VT, voice therapy; Δ, change. Forest Plot of the adjusted estimated improvement in Voice Handicap Index-10 (VHI-10) scores by treatment group; Abbreviations: PT, physical therapy; VT, voice therapy.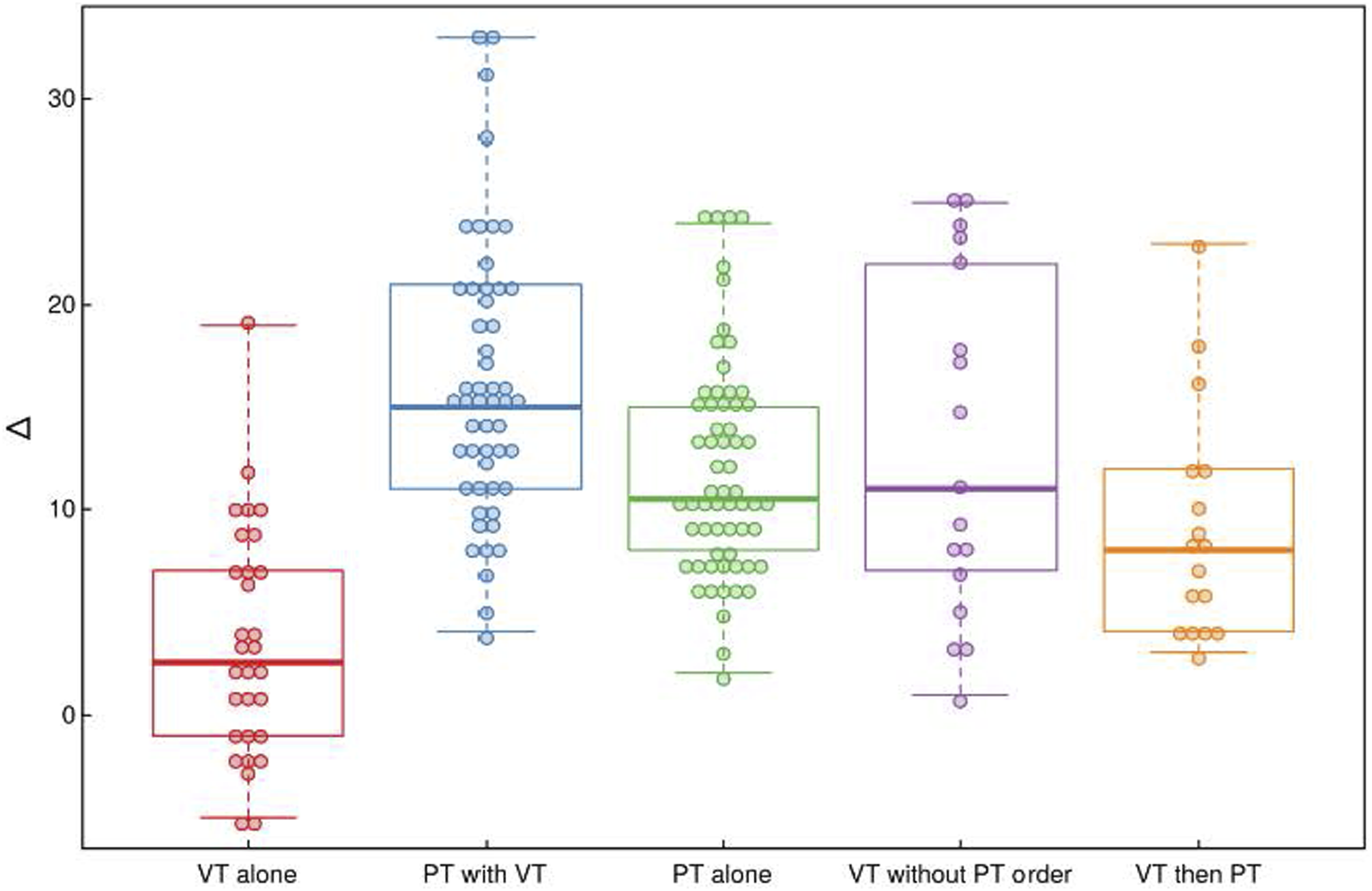
PSFS Outcomes
Comparison of Patient Specific Functional Score by treatment group.
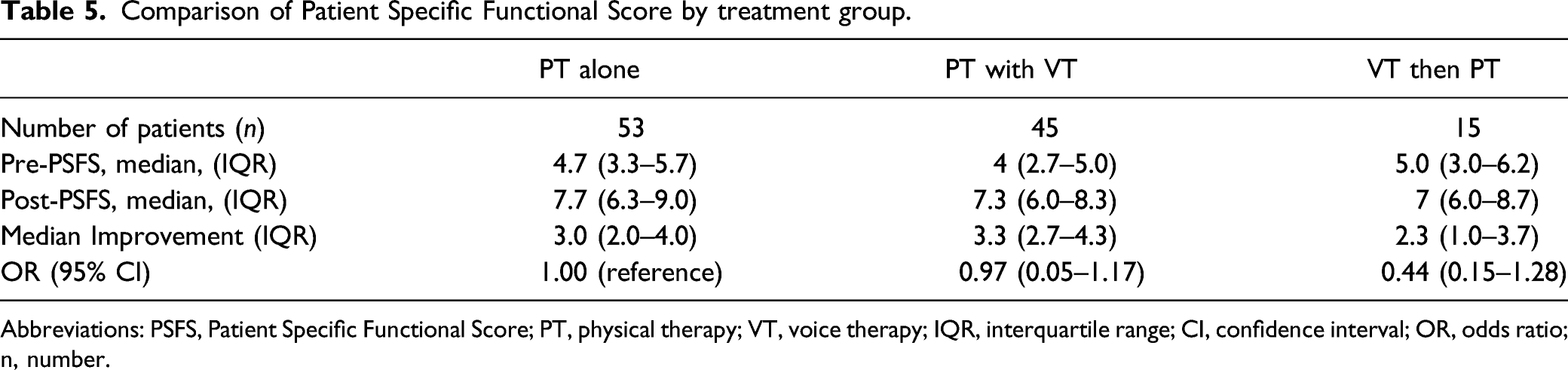
Abbreviations: PSFS, Patient Specific Functional Score; PT, physical therapy; VT, voice therapy; IQR, interquartile range; CI, confidence interval; OR, odds ratio; n, number.
Discussion
Muscle tension dysphonia is the most common voice condition seen in voice centers and its treatment remains challenging. The primary treatment modality is voice therapy, ideally, with a voice-specialty trained speech language pathologist.2,3 This treatment has shown to be effective for most primary MTD patients; however, there is a subset of patients with MTD and significant cervicalgia which tends to be more recalcitrant to improvement with standard approaches. This study shows, in a series of patients with primary MTD and cervicalgia, that voice-directed PT treatment offers an additional effective treatment option that can improve voice as demonstrated through both VHI-10 and PSFS scores. In fact, it is essential to note that those completing the PT program had significant improvement in VHI-10 scores regardless of undergoing VT or not. All patients in the study had a diagnosis of primary MTD as well as cervicalgia and so were counseled and offered voice therapy and physical therapy. It was only those in the VT without PT order group that did not have a PT order in place. Of note, those in the VT alone group had a PT order in place but did not undergo PT.
Based on the data in this study, whole-body manual physical therapy should be considered for those with MTD and cervicalgia. It is possible that extra-laryngeal and extra-cervical components of the voicing mechanism (e.g., neck, back, shoulders, and diaphragm musculature) are contributing to the MTD and are not sufficiently treated with traditional voice therapy techniques alone. Circumlaryngeal massage and whole-body manual therapy have similar foundational underpinnings, but the latter addresses muscular areas not typically considered when treating dysphonia. The results of this study emphasize that a more holistic approach to treating muscle tension dysphonia may be warranted in select patients with cervicalgia. 16 Finding a physical therapist open to addressing this unique set of cervical issues is valuable. It is preferred to find a physical therapist who can assess and treat muscle imbalances and substitution patterns in the scalenes and diaphragm, infrahyoids/straps and transverse abdominis/rhomboids as well as anterior neck tissue restrictions. To address the tissue restrictions, one would want to find a physical therapist versed in soft tissue manual therapy skills such as myofascial release or lymphatic drainage to bring this skill set to benefit your laryngology team for improved patient care.
It remains undetermined if MTD promotes, or is the consequence of, extra-laryngeal muscle tension or cervicalgia. Interesting is the finding that a high percentage of our patients had concomitant chronic pain, anxiety and/or depression (Table 3). These conditions have been considered to mitigate therapy effectiveness. This assertion is supported by prior studies that have found that dysphonia in these populations is often refractory to standard of care voice therapy.29,31,32 In this current study, it is intriguing that patients that underwent VT, but did not have PT ordered had similarly positive clinical outcomes to all groups except VT alone (Table 4). The theorized explanation is that these patients had less severe cervicalgia that was easily ameliorated with standard voice therapy with circumlaryngeal massage. Also interesting is that those in the VT then PT group did not fare as well as those in the VT without PT order group or PT alone group. It was hypothesized that those in the VT then PT group were possibly more treatment resistant because if this VT then PT group of patients were that much better with VT alone then they would have possibly not then undergone PT as originally suggested by the referring laryngologist.
Cervicalgia is not monolithic and can be muscular, as described herein, and can be additionally due to a number of other serious etiologies. As such, it is important to emphasize that many forms of cervicalgia can have other origins including radiculopathy and rheumatological causes. Thus, many patients with non-traditional muscular cervicalgia may need referrals to other specialties (e.g., neurology, neurosurgery, orthopedics, rheumatology or physical medicine and rehabilitation). However, physical therapists are trained to monitor for worrisome radicular signs that can be associated with cervicalgia.
These findings are important; however, study limitations deserve mention. First, definitions of cervicalgia are not standardized across all centers, which could affect generalizability of results. Also, VHI-10 scores were not systematically collected on all patients at the voice center, which could lead to selection bias. Despite this concern, no differences in patient characteristics were noted across treatment types; therefore, systematic bias in treatment selection seems unlikely. In most cases, patients that underwent voice therapy had only two treatment sessions of voice therapy beyond the initial SLP assessment session (Table 3). However, it should be noted that those in the VT without PT order group responded well with voice therapy as the only treatment modality with two treatment sessions (Table 4). This demonstrated that some patients with only two treatment sessions of voice therapy beyond the initial SLP assessment session did respond well. Another important limitation of this study is that patients self-selected into the treatment arms. Reasons for this may include improvement with the initial therapy, insurance or other financial considerations, and availability of appropriate therapists in their community. It is possible that the associations observed in this study are a consequence of unobserved patient characteristics that are correlated with the choice of treatment modality.
This study is among the first to show that a manual PT treatment regimen encompassing a full-body approach was associated with voice improvement. It is not our intention to imply that PT is an alternative to VT for MTD. Rather, PT should be considered an adjunct for select patients. Caution must be exercised in interpreting these findings as the causal association of PT and VHI-10 score improvement cannot be definitively shown until randomized controlled trials are performed. Prospective studies are needed to delineate factors that predict degree of benefit with either or both therapies in order to better guide clinicians in cost-effective management.
Conclusion
Whole body manual physical therapy is an important adjunctive therapy for patients with MTD and cervicalgia. In select patients, PT treatment significantly improved VHI-10 scores when used alone. Further study is needed to clarify whether these results are generalizable across centers. However, we believe that for those that are refractory or not responsive to the standard treatment of MTD, cervicalgia should be considered in view that manual PT may be beneficial for these patients.
Previous Presentation as a Podium presentation at the 2019 Fall Voice Conference, Dallas, TX, 19 October 2019.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The Physical Therapy intervention in this study is a copyrighted program. Vanderbilt University Medical Center, 2013 with revisions 2019: All Rights Reserved. Created by co-author Carey A. Tomlinson, Physical Therapist for the Vanderbilt Dayani Center. All necessary permission was obtained for use of this program in this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Clinical and Translational Science Awards number UL1 TR002243 from the National Center for Advancing Translational Sciences. Its contents are solely the responsibility of the authors and do not necessarily represent official views of the National Center for Advancing Translational Sciences or the National Institutes of Health.